



Case Report - (2023) Volume 8, Issue 2
How Should I Treat Under Expanded Coronary Stents Due to Severe Coronary Calcification?
2ASST Lecco - Ospedale Alessandro Manzoni, Italy
Received Date: Jul 27, 2023 / Accepted Date: Aug 20, 2023 / Published Date: Aug 28, 2023
Copyright: ©Â©2023 F Napoli, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Napoli, F., Tiberti, G. (2023). How Should I Treat Under Expanded Coronary Stents Due to Severe Coronary Calcification? Cardio Open, 8(2), 52-55.
Abstract
With aging society, one of the more challenging obstacles in percutaneous coronary interventions (PCI) are calcified coronary lesions (CAC). CAC may impede stent delivery; limit balloon and stent expansion, which result in lower minimal stent area (MSA), cause uneven drug distribution, and even hinder wire advancement [1-4]. Lower MSA and stent under-expansion are associated with adverse outcomes, including stent thrombosis, restenosis, and major adverse cardiac outcomes (MACE) [5,6].
Background
With aging society, one of the more challenging obstacles in percutaneous coronary interventions (PCI) are calcified coronary lesions (CAC). CAC may impede stent delivery; limit balloon and stent expansion, which result in lower minimal stent area (MSA), cause uneven drug distribution, and even hinder wire advancement [1-4]. Lower MSA and stent under-expansion are associated with adverse outcomes, including stent thrombosis, restenosis, and major adverse cardiac outcomes (MACE) [5,6].
In order to effectively manage such lesions, dedicated technologies have been developed. Rotational (RA) and orbital atherectomy (OA) are the devices mainly used to ablate superficial calcium in the coronary artery. Using coronary lithotripsy, lesion modification is achieved by pulsatile mechanical energy delivered to calcified lesions. The result is an amplified effect in calcified tissues and a much weaker impact on healthy tissue. Unlike rotational or orbital atherectomy, IVL can affect deeper tissues, which enables the modification of calcified plaque behind a stent. Furthermore, IVL does not produce particles that embolize; therefore, less slow-flow phenomena can be seen. In this setting, we discuss the clinical case in which an IVL was required to treat under expanded coronary stents due to severe CAC.
Case Presentation
An 58-year-old male patient was electively admitted to our hospital’s Cardiology Department with stable angina and two coronary plaques in two major vessel showing on coronary tomography. He has an active history of smoking 40 cigarettes per day and hypertension.
Coronary angiography revealed extensively calcified left anterior discendent (LAD) coronary artery with critical calcified lesions in the middle tract. Lesion preparation was done using non-compliant balloon (NCB) 2.5 x 20 mm followed by a drug- eluting stent (DES) implantation 2.75 x 38 mm.

Figure A: LAO Cranial View Demonstrating Severe LAD Stenosis

Figure B: LAO Cranial View Demonstrating LAD Stenosis with under Expansion of 2.75 x 38 mm DES
DES was sub-optimally expanded after standard deployment compared with nominal sizes. Post-dilatation using 2.75 x 12 NCBs following 3 x 6 mm NCB and 3.25 x 8 mm NCB was performed. Unfortunately, LAO cranial view still demonstrated DES under expansion. In this setting Rotational atherectomy, RA and OA were contraindicated for intrastent treatment. At the contrary intravascular lithotripsy (IVL) was indicated.

Figure C: LAO Cranial View Demonstrating Adequate DES Expansion
IVL balloon 3.0 x 12 mm was easy delivered to the desired location over a 0.014 guidewire. Once the position was confirmed, the IVL balloon was inflated to 4 atm using a 1:1 water and contrast mixture, then by pressing the button on the delivery catheter, 10 pulsed electrical impulses were delivered up within 10s (one pulse per second). Successively the IVL balloon was inflated further to 6 atm and 80 totally pulses were applied (eight cycles). Thereafter LAO cranial view showed DES fully expanded.
Discussion
Intravascular coronary lithotripsy is useful in more challenging scenarios. One of the promising potential indications in the treatment of in-stent restenosis associated with calcium and under expanded DES with underlying calcification. Patients with severe stent under expansion due to CAC are at a higher risk of stent failure and future adverse events. Under expanded stents are currently being treated with off-label use of other atherectomy devices [7,8].
Nevertheless, the effectiveness of those techniques is limited by the presence of metallic struts, deeper calcifications remain unaffected, and the risks of procedural complications and stent damage are unpredictable. Conversely, the circumferential sonic waves of coronary IVL have the advantage of extending beyond stent struts and are thus capable of disrupting and fracturing deeper calcium deposits. Several case reports have supported the use of the technology for optimizing stent expansion without complications [9,10].

Figure: DES under Expansion before Intravascular Litotripsy
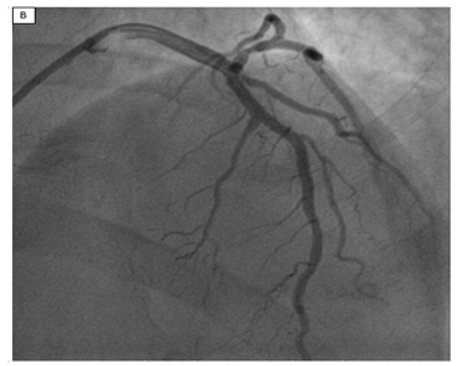
Figure: DES Expansion after Intravascular Litotripsy
Nevertheless, the efficacy of the system in lesions previously treated with multiple layers of the stent has not been demonstrated, and its impact on the stent backbone, polymer integrity, and drug elution is unknown.
References
- Gilutz, H., Weinstein, J. M., & Ilia, R. (2000). Repeated balloon rupture during coronary stenting due to a calcified lesion: an intravascular ultrasound study. Catheterization and Cardiovascular Interventions, 50(2), 212-214.
- Moussa, I., Di Mario, C., Moses, J., Reimers, B., Di Francesco, L., Martini, G., ... & Colombo, A. (1997). Coronary stenting after rotational atherectomy in calcified and complex lesions: Angiographic and clinical follow-up results. Circulation, 96(1), 128-136.
- Nakano, M., Otsuka, F., Yahagi, K., Sakakura, K., Kutys, R., Ladich, E. R., ... & Virmani, R. (2013). Human autopsystudy of drug-eluting stents restenosis: histomorphological predictors and neointimal characteristics. European heart journal, 34(42), 3304-3313.
- Creel, C. J., Lovich, M. A., & Edelman, E. R. (2000). Arterial paclitaxel distribution and deposition. Circulation research, 86(8), 879-884.
- Mosseri, M., Satler, L. F., Pichard, A. D., & Waksman,R. (2005). Impact of vessel calcification on outcomes after coronary stenting. Cardiovascular Revascularization Medicine, 6(4), 147-153.
- Mintz, G. S. (2015). Intravascular imaging of coronary calcification and its clinical implications. JACC: Cardiovascular Imaging, 8(4), 461-471.
- Whiteside, H. L., Nagabandi, A., & Kapoor, D. (2019). Stentablation with rotational atherectomy for the management of underexpanded and undilatable coronary stents. Cardiovascular Revascularization Medicine, 20(12),1203-1208.
- Wilson, A., Ardehali, R., Brinton, T. J., Yeung, A. C., & Lee, D. P. (2006). Cutting balloon inflation for drug-eluting stent underexpansion due to unrecognized coronary arterial calcification. Cardiovascular Revascularization Medicine, 7(3), 185-188.
- Salazar, C., Escaned, J., Tirado, G., & Gonzalo, N. (2019).Undilatable calcific coronary stenosis causing stentunderexpansion and late stent thrombosis: a complex scenario successfully managed with intravascular lithotripsy. JACC: Cardiovascular Interventions, 12(15), 1510-1512.
- Tovar Forero, M. N., Wilschut, J., Van Mieghem, N. M., & Daemen, J. (2019). Coronary lithoplasty: a novel treatment for stent underexpansion. European Heart Journal, 40(2), 221-221.