
COVID Research: Open Access(CROA)
ISSN: 2995-7826 | DOI: 10.33140/CROA


Research Article - (2024) Volume 2, Issue 2
High Asymptomatic Presentation of Covid-19 in Ghana: Factors to Consider for Enhanced Pandemic Control
2Ghana Field Epidemiology and Laboratory Training Programme, Department of Epidemiology and Disease Control, School of Public Health, University of Ghana, Ghana
Received Date: Apr 24, 2024 / Accepted Date: May 16, 2024 / Published Date: May 28, 2024
Copyright: ©©2024 Keziah L. Malm, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Malm, K. L., Bekoe, F. A., Adu, G. A., Lwanga, C. N., Sarkodie, B., et al. (2024). High Asymptomatic Presentation of Covid-19 in Ghana: Factors to Consider for Enhanced Pandemic Control. COVID Res OA, 2(2), 01-09.
Abstract
Background: Ghana recorded its first two COVID-19 cases on March 12, 2020; and as of May 05, 2020, a total of 2719 confirmed cases and 18 deaths were recorded in ten (10) regions of Ghana with Greater Accra Region been the epicenter of the outbreak. Analysis of patient data by the Ghana Health Service (GHS) revealed an asymptomatic carrier rate of 93%. This was higher compared with the 25-50% rates for China, Singapore and other parts of the world. Consequently, this study sought to determine factors associated with the asymptomatic presentation of Ghana’s COVID-19 cases to inform design and targeting of control interventions.
Methods: A cross-sectional survey was conducted from 20th July to 14th August 2020 in all 10 regions that had confirmed up to 20 cases as of May 14, 2020. Study participants were randomly selected and asked questions on socio-demographics, lifestyle, medical history among others. Data was described using frequencies, proportions, means and standard deviation. Association between patient asymptomatic status and the predictive variables were determined by logistic regression.
Results: In all, 672 patients participated in this study, mean age been 31.0 years (standard deviation, SD) ±5.3), and majority been male 388 (57.7%). Eighty-five percent (571) of participants showed no symptom of the disease. Factors associated with asymptomatic presentation included: patient having three (3) meals in a day [cOR=0.56 (0.33-0.97)], adding green leafy vegetables to meal [cOR=0.41 (0.19-0.88)], drinking hibiscus flower tea (“Sobolo”) [cOR=0.56 (0.31-0.98)], performing extra physical activity [cOR=0.7 (0.17-2.88)], patient attaining some level of formal education [Primary cOR=0.16 (0.03- 0.93); Junior High School (JHS) cOR=0.24 (0.08-0.75); and Senior High School (SHS) cOR=0.14 (0.05-0.41)]. Hypertension increased the odds [cOR=1.71 (1.21-2.99)] of symptom(s) presentation among its victims.
Conclusion: This study found an asymptomatic proportion of 85%, slightly lower than the 93% reported by GHS. Factors associated with asymptomatic COVID-19 status were patients having three (3) meals per day, adding green leafy vegetables to meal, drinking hibiscus flower (“Sobolo”) tea, indulging in extra physical activity, and attaining Primary, JHS and SHS education. On the other hand, patients with hypertension were more prone to show symptom(s) of the disease than non- hypertensives. Efforts at controlling the disease should include education on adding green leafy vegetables to meals and hypertension prevention and management. Designated state institutions and the research fraternity should carry out further studies to give guidance on use of hibiscus flower.
Keywords
Covid-19, Asymptomatic, Lifestyle, Nutrition, Medical History, GhanaIntroduction
Severe Acute Respiratory Syndrome Coronavirus-2 (SARS- CoV-2) causes COVID-19 disease in people and spread from person to person through infected droplets and droplet nuclei. It presents with symptoms such as cough, fever, difficulty in breathing, sore throat, runny nose, body aches among others. The novel case of the virus was identified on 31st December, 2019 in Wuhan, city of China. Since its emergence, several cases of the virus were reported around the world and on January 30, 2020, the World Health Organization (WHO) declared it as a Public Health Emergency of International Concern. Owing to the rapid continuing spread of the virus, the WHO on March 11, 2020 officially declared it as a pandemic. As of August 20, 2021, more than 210 million cases with over 4.41 million deaths have been recorded worldwide.
Ghana recorded its first two COVID-19 cases on March 12, 2020; and many cases have been confirmed in several parts of the country since introduction. As of May 05, 2020, a total of 2719 confirmed cases and 18 deaths had been recorded in Ghana, with Greater Accra Region been epicenter of the outbreak (1).
Numerous strategies and interventions were instituted by the Government of Ghana to halt the spread of the virus. Among these interventions included: closing of all borders to prevent further importation of the virus, training of health workers and provision of relevant PPEs, preparing health facilities for isolation, prompt identification and management of cases, Enhanced Contact Tracing (ECT), improved personal hygiene practices and restrictions on human movements (5).
From March through to May 2020, as part of efforts to curb the spread of the disease, the country undertook an Enhanced Contact Tracing which identified people in the community who were infected by SAR-COV 2, it was estimated then that, 93% of all the SARS-COV 2 positive cases were asymptomatic (3). This was high compared with the 35% global average reported by CDC (2). COVID-19 asymptomatic case proportion of 33.3% has been reported in South Korea which is closer to that reported by Nishiura et al. (2020) in Japan where a prevalence of 30.8% was reported (10,11). Available studies suggest that asymptomatically infected individuals are much less likely to transmit the SARS-CoV-2 virus than those with symptoms (WHO, June 2020). Scientific report has suggested that the transmissibility of these asymptomatic cases might be smaller than that of the symptomatic cases (7). Additionally, there is a better prognosis for the disease if an infected person does not show symptoms. The propagation from asymptomatic PCR positive individuals represents a complicating factor in the efforts to control COVID-19 (9). This makes knowledge on factors influencing asymptomatic presentation crucial for pandemic control. The Ghana Health Service saw the need to carry out this survey to identify factors associated with the asymptomatic presentation to inform decision making on control strategies.
Methods
Study Area
All 10 regions which had confirmed up to 20 cases as of May 14, 2020, were part of the study. The study regions included Greater Accra, Ashanti, Eastern, Central, Volta, Oti, Western, Northern, Upper East, and West regions (Figure 1).

Figure 1: Map Showing Study area in Red.
Study Design and Population
This was an exploratory cross-sectional survey conducted on patients who tested positive for SAR-COV 2 between March 12, and May 14, 2020.
Exclusion Criteria
o Since questionnaires were administered via phone calls, cases without phone numbers were excluded.
o Cases who were declared dead were excluded from the sample frame.
o Cases who did not consent to the study.
Sample Size Estimation
The study considered asymptomatic proportion as unknown and used 50% as assumed prevalence for sample size estimation. Using the formula, n = DE * [(z2pq)/d2] with n = sample size; p = estimated proportion of asymptomatic cases (50% = 0.5); q = 1 – p; z = 1.96 and d =5% at 95% confidence interval and a design effect (DE) of 2, a minimum sample size of 704 was estimated for the study. But the study finally collected data from 672 respondents due to the decline of participation by a number of participants, particularly those who denied been cases due to their asymptomatic presentation.
Sampling Procedure
A list of all COVID-19 cases in the 10 regions was obtained from the National Surveillance Department of the Ghana Health Service. After which cases with phone numbers were selected as the sampling frame. Random numbers were assigned to cases and a table of random numbers used to select number of participants for the study.
Data Collection and Variables
Data collection spanned from 20th July to 14th August 2020, trained data collectors used a Semi-structured questionnaire deployed on Kobo collect mobile App to collect information from participants. Questionnaires were administered via phone calls to avoid breach of COVID protocols and minimize risk of spread of the virus among data collectors and study participants. Variables collected includes; socio-demographic characteristics (Age, sex, education, occupation, marital status), lifestyle factors (smoking, drinking, nutrition, physical activities), previous medical history, underlining medical conditions, status of COVID symptoms among others. The study defined asymptomatic COVID-19 patient as anyone who tested positive for COVID-19 but showed no sign or symptom of the disease. Symptomatic cases were people who tested positive for COVID-19 and showed at least one sign or symptom of the disease.
Data Analysis
The dataset was extracted from Kobo collect into Microsoft Excel 2013 and cleaned. Data was then imported to STATA Version 13.0 for analysis, where frequencies were generated for socio-demographic characteristics such as age, sex, marital status, level of education, and occupation. Proportions and means were generated for all continuous data while association between outcome and the explanatory variables were determined through univariate analyses (Chi-square and Fishers exact tests significant at p<0.05). Variables proving significant in the univariate analysis were subsequently put into a multiple logistic regression to determine their independent effects. Though insignificant at univariate analysis, hypertension was included in the multiple logistic regression due to its known association with severe form of the disease (15).
Limitations of the Study
This study has few limitations. Symptom status of patient on survey day was enquired through phone call without any physical assessment. Some patients may have experienced mild symptoms in the past or on survey day without recognition. The cross-sectional design restricts the establishment of causal relationships between variables. Additionally, the reliance on self-reported data might introduce recall bias, influencing the accuracy of symptom reporting. Future longitudinal studies encompassing larger and diverse cohorts could provide more nuanced insights into the multifaceted determinants of COVID-19 outcomes in Ghana.
Ethical Statement
This study forms part of a bigger study titled “Clinical Characterization and Outcome of COVID-19 in Ghana” which was granted approval (GHS-ERC/006/05/20) by the Ghana Health Service Ethics Review Committee. Oral consent via phone was obtained from all participants before enrollment. Participants were informed of the voluntary nature of their participation, and right to decline at any point of the study. Confidentiality of data was ensured by using questionnaire codes instead of names of study subjects.
Results
Socio-Demographics and Symptoms Presentation of Participants
A total of 672 patients participated in this study. The mean age of participants was 31.0 years (standard deviation, SD) ±5.3), majority 388 (57.7%) being males, and 395 (58.8%) engaged in the informal sector employment. Of the patients sampled, 85% (571) did not show any symptom at the time sample was taken or any time before and after sample was taken (Table 1). For the symptomatic, the common symptoms cited included cough (45.1%), headache (38.2%), fever (34.3%), bodily pain weakness (33.3%) among others (Figure 2).
|
Variables |
Frequency (N) |
Percent (%) |
|
Age (years) |
|
|
|
<20 |
42 |
6.3 |
|
20 – 29 |
203 |
30.2 |
|
30 – 39 |
218 |
32.4 |
|
40 – 49 |
120 |
17.9 |
|
50 – 59 |
63 |
9.4 |
|
60 + |
26 |
3.9 |
|
Sex |
|
|
|
Female |
284 |
42.3 |
|
Male |
388 |
57.7 |
|
Level of education |
|
|
|
No formal education |
31 |
4.6 |
|
Primary |
29 |
4.3 |
|
JHS |
116 |
17.3 |
|
SHS/Vocational |
244 |
36.3 |
|
Tertiary |
252 |
37.5 |
|
Marital status |
|
|
|
Single |
321 |
47.8 |
|
Married/cohabiting |
323 |
48.1 |
|
Divorced/Separated/Widowed |
28 |
4.2 |
|
Occupation |
|
|
|
Informal sector |
395 |
58.8 |
|
Private formal |
107 |
15.9 |
|
Public formal sector |
103 |
15.3 |
|
Unemployed |
67 |
10.0 |
|
Household size |
|
|
|
1 |
141 |
21.0 |
|
2 – 4 |
320 |
47.6 |
|
5 – 7 |
162 |
24.1 |
|
8 + |
49 |
7.3 |
|
Number of rooms |
|
|
|
1 |
263 |
39.2 |
|
2 |
200 |
29.8 |
|
3 |
86 |
12.8 |
|
4 + |
122 |
18.2 |
|
Presentation |
|
|
|
Asymptomatic |
570 |
85.0 |
|
Symptomatic |
102 |
15.0 |
Table 1: Demographic Characteristics and Symptom Status of Covid 19 Patients in Ghana, 2020
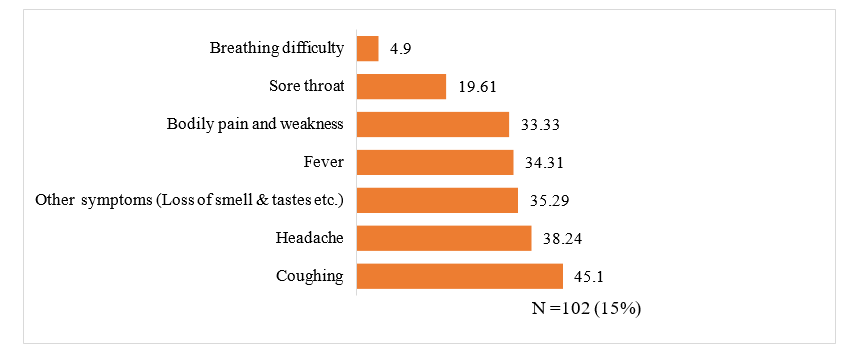
Figure 2: Types of Covid 19 Symptoms Presented by Participants, Ghana, 2020
Patients’ Socio-Demographic Factors Associated with Asymptomatic Covid-19 Presentation, Ghana, 2020
Patients’ formal educational status and type of employment proved significantly associated with their symptom status. The results showed that patients who had attained Junior high school education had reduced odds [cOR= 0.27 (0.10-0.76)] of showing symptoms of COVID-19 compared with those with no formal education. Also, participants who had attained SHS education showed reduced odds [cOR= 0.23 (0.09-0.58)] of presenting with symptoms compared to those without any formal education. Patients who belonged to the public formal sector had 83% increased odds of presenting with symptoms than those of the informal sector (Table 2).
|
|
COVID-19 Asymptomatic |
|
|
|
Characteristics |
Yes (%) |
No (%) |
cOR (95% CI) |
|
Age, years |
|
|
|
|
< 20 |
37 (6.5) |
5 (4.9) |
1.00 [reference] |
|
20 – 29 |
176 (30.9) |
27 (26.5) |
1.14 [0.41-3.14] |
|
30 – 39 |
173 (30.4) |
45 (44.1) |
1.92 [0.72-5.18] |
|
40 – 49 |
107 (18.8) |
13 (12.8) |
0.90 [0.30-2.69] |
|
50 – 59 |
55 (9.7) |
8 (7.8) |
1.08 [0.33-3.55] |
|
60 + |
22 (3.9) |
4 (3.9) |
1.35 [0.33-5.55] |
|
Sex |
|
|
|
|
Female |
244 (42.8) |
40 (39.2) |
1.00 [reference] |
|
Male |
326 (57.2) |
62 (60.8) |
1.16 [0.75-1.78] |
|
Level of education |
|
|
|
|
No formal education |
23 (4.0) |
8 (7.8) |
1.00 [reference] |
|
Primary |
27 (4.7) |
2 (2.0) |
0.21 [0.04-1.10] |
|
JHS |
106 (18.6) |
10 (9.8) |
0.27 [0.10-0.76] * |
|
SHS/Vocational |
226 (39.7) |
18 (17.7) |
0.23 [0.09-0.58] * |
|
Tertiary |
188 (33.0) |
64 (62.8) |
0.98 [0.42-2.30] |
|
Marital status |
|
|
|
|
Married/cohabiting |
269 (47.2) |
54 (52.9) |
1.00 [reference] |
|
Single |
277 (48.6) |
44 (43.1) |
0.79 [0.51-1.22] |
|
Divorced/Separated/ Widowed |
24 (4.2) |
4 (3.9) |
0.83 [0.28-2.49] |
|
Occupation |
|
|
|
|
Informal sector |
344 (60.4) |
51 (50.0) |
1.00 [reference] |
|
Private formal |
88 (15.4) |
19 (18.6) |
1.46 [0.82-2.59] |
|
Public formal sector |
81 (14.2) |
22 (21.6) |
1.83 [1.05-3.19] * |
|
Unemployed |
57 (10.0) |
10 (9.8) |
1.18 [0.57-2.46] |
|
Household size |
|
|
|
|
1 |
115 (20.2) |
26 (25.5) |
1.00 [reference] |
|
2 – 4 |
271 (47.5) |
49 (48.0) |
0.80 [0.47-1.35] |
|
5 – 7 |
138 (24.2) |
24 (23.5) |
0.77 [0.42-1.41] |
|
8 + |
46 (8.1) |
3 (2.9) |
0.29 [0.08-1.00] |
|
Number of rooms |
|
|
|
|
1 |
223 (39.2) |
40 (39.2) |
1.00 [reference] |
|
2 |
170 (29.9) |
30 (29.4) |
0.98 [0.59-1.64] |
|
3 |
76 (13.4) |
10 (9.8) |
0.73 [0.35-1.54] |
|
4 + |
100 (17.6) |
22 (21.6) |
1.23 [0.69-2.17] |
COR=Crude Odds Ratio
Table 2: Patients Socio-Demographic Factors and Asymptomatic COVID 19 Status in Ghana, 2020
Patients’ Nutritional, Lifestyle And Medical Factors Associated With Asymptomatic Covid-19 Presentation, Ghana, 2020
Drinking 2.5 liters or more of water per day, eating 3 times a day, eating green leafy vegetables, consumption of hibiscus flower tea (“locally called Sobolo”) and engaging in physical activity were the nutritional and lifestyle factors significantly associated with asymptomatic presentation. The study discovered that patients who drunk 2.5 - 4.5 liters of water per day were less likely to show symptoms than those who consumed less [cOR= 0.49 (0.30-0.79)], and protection is better if daily water intake exceeds 4.5 liters of water per day [cOR= 0.35 (0.16-0.77].
Patients who had three (3) meals in a day were also less likely to come down with symptoms compared to those who had less than three (3) meals in a day [cOR= 0.59 (0.37-0.94)]. Further, patients who added green leafy vegetables to their meal were better protected from COVID-19 symptoms than those who did not [cOR= 0.37 (0.20-0.68)]. Patients who drunk a tea prepared out of hibiscus flower (“Sobolo”) also had reduced odds of showing symptoms than those who did not [cOR= 0.56 (0.34- 0.90)] (Table 3).
|
|
|
COVID-19 Asymptomatic |
|
|
Characteristics |
Yes (%) |
No (%) |
cOR (95% CI) |
|
Consumption of water per day |
|
|
|
|
< 2.5 liters |
104 (18.3) |
33 (32.4) |
1.00 [reference] |
|
2.5 – 4.5 liters |
385 (67.5) |
60 (58.8) |
0.49 [0.30-0.79] * |
|
>4.5 liters |
81 (14.2) |
9 (8.8) |
0.35 [0.16-0.77] * |
|
Meals per day |
|
|
|
|
< 3 |
147 (28.5) |
38 (39.2) |
1.00 [reference] |
|
3 |
346 (67.2) |
53 (54.6) |
0.59 [0.37-0.94] * |
|
4 + |
22 (4.3) |
6 (6.2) |
1.06 [0.40-2.78] |
|
Eats green leafy vegetables |
|
|
|
|
No |
40 (7.8) |
18 (18.6) |
1.00 [reference] |
|
Yes |
475 (92.2) |
79 (81.4) |
0.37 [0.20-0.68] * |
|
Consumes garlic |
|
|
|
|
No |
66 (12.5) |
10 (10.5) |
1.00 [reference] |
|
Yes |
463 (87.5) |
85 (89.5) |
1.21 [0.60-2.45] |
|
Consumes Ginger |
|
|
|
|
No |
43 (8.1) |
11 (11.2) |
1.00 [reference] |
|
Yes |
489 (91.9) |
87 (88.8) |
0.70 [0.35-1.40] |
|
Consumes Sobolo |
|
|
|
|
No |
99 (17.4) |
28 (27.5) |
1.00 [reference] |
|
Yes |
471 (82.6) |
74 (72.6) |
0.56 [0.34-0.90] * |
|
Consumed any vitamin supplements |
|
|
|
|
No |
327 (58.7) |
57 (56.4) |
1.00 [reference] |
|
Yes |
230 (41.3) |
44 (43.6) |
1.10 [0.72-1.68] |
|
Consumed Vitamin D supplements |
|
|
|
|
No |
491 (95.0) |
95 (95.0) |
1.00 [reference] |
|
Yes |
26 (5.0) |
5 (5.0) |
0.99 [0.37-2.65] |
|
Drinks alcohol |
|
|
|
|
No |
455 (81.0) |
76 (75.3) |
1.00 [reference] |
|
Yes |
107 (19.0) |
25 (24.8) |
1.40 [0.85-2.30] |
|
Exposure to dust |
|
|
|
|
No |
163 (58.8) |
39 (61.9) |
1.00 [reference] |
|
Yes |
114 (41.2) |
24 (38.1) |
0.88 [0.50-1.54] |
|
Does extra physical activities |
|
|
|
|
No |
281 (49.3) |
64 (62.8) |
1.00 [reference] |
|
Yes |
289 (50.7) |
38 (37.3) |
0.58 [0.37-0.89] * |
|
|
|
|
|
|
Suffers Diabetes |
|
|
|
|
No |
43 (89.6) |
16(80.0) |
1.00 [reference] |
|
Yes |
5 (10.4) |
4 (20.0) |
2.15 [0.51-9.03] |
|
Hypertension |
|
|
|
|
No |
27 (56.3) |
9 (45.0) |
1.00 [reference] |
|
Yes |
21 (43.8) |
11 (55.0) |
1.57 [0.55-4.49] |
|
Suffers Asthma |
|
|
|
|
No |
42 (87.5) |
18 (90.0) |
1.00 [reference] |
|
Yes |
6 (12.5) |
2 (10.0) |
0.78 [0.14-4.23] |
|
Suffered Malaria in past 3 years |
|
|
|
|
No |
24 (46.2) |
10 (41.7) |
1.00 [reference] |
|
Yes |
28 (53.9) |
14 (58.3) |
1.20 [0.45-3.19] |
COR=Crude Odds Ratio
Table 3: Patient’s Nutritional, Lifestyle and Medical Factors Associated with Asymptomatic Covid 19 Status, Ghana, 2020
Factors Associated with Symptomatic COVID Status in Ghana, 2020
After adjusting for confounders, patients’ formal educational status, number of meals per day, including green leafy vegetables in meal, consumption of “Sobolo” and being hypertensive were the factors associated with asymptomatic presentation. Compared with those without any formal education, patients who had attained at least Primary, JHS, and SHS education had reduced odds of showing symptoms of COVID-19. Those with primary education had [aOR= 0.16 (0.03-0.93)], those with JHS had [aOR= 0.24 (0.08-0.75)] and those with SHS/vocational education had [aOR= 0.14 (0.05-0.41)] of showing symptoms of COVID-19. Patients who usually have three (3) meals in a day had lower odds of coming down with symptoms than those who had less than three (3) meals in a day [0.56 (0.33-0.97)]. Adding green leafy vegetables to meals was also protective against COVID-19 related symptoms, those whose meals included green leafy vegetables had reduced odds [0.41 (0.19- 0.88)] of coming down with symptoms than those who included no green leafy vegetable. Patients who drunk hibiscus flower tea (“Sobolo”) also had reduced odds of presenting symptoms than those who did not [0.56 (0.31-0.98)]. However, patients who were hypertensive had increased odds of been symptomatic than those with no hypertension [1.71 (1.21-2.99)] (Table 5).
|
|
COVID-19 Asymptomatic |
|
|
|
|
Characteristics |
Yes (%) |
No (%) |
AOR (95% CI) |
P-value |
|
Formal Education |
|
|
|
|
|
No formal education |
23 (4.0) |
8 (7.8) |
1.00 [reference] |
|
|
Primary |
27 (4.7) |
2 (2.0) |
0.16 [0.03-0.93] |
0.042* |
|
JHS |
106 (18.6) |
10 (9.8) |
0.24 [0.08-0.75] |
0.014* |
|
SHS/Vocational |
226 (39.7) |
18 (17.7) |
0.14 [0.05-0.41] |
<0.001* |
|
Tertiary |
188 (33.0) |
64 (62.8) |
0.65 [0.23-1.84] |
0.420 |
|
Occupation |
|
|
|
|
|
Informal sector |
344 (60.4) |
51 (50.0) |
1.00 [reference] |
|
|
Private formal |
88 (15.4) |
19 (18.6) |
1.68 [0.86-3.31] |
0.130 |
|
Public formal sector |
81 (14.2) |
22 (21.6) |
1.24 [0.63-2.43] |
0.537 |
|
Unemployed |
57 (10.0) |
10 (9.8) |
1.52 [0.62-3.69] |
0.358 |
|
Consumption of water per day |
|
|
|
|
|
< 2.5 liters |
104 (18.3) |
33 (32.4) |
1.00 [reference] |
|
|
2.5 – 4.5 liters |
385 (67.5) |
60 (58.8) |
0.98 [0.54-1.77] |
0.943 |
|
>4.5 liters |
81 (14.2) |
9 (8.8) |
0.70 [0.28-1.75] |
0.448 |
|
Meals per day |
|
|
|
|
|
< 3 |
147 (28.5) |
38 (39.2) |
1.00 [reference] |
|
|
3 |
346 (67.2) |
53 (54.6) |
0.56 [0.33-0.97] |
0.038* |
|
4 + |
22 (4.3) |
6 (6.2) |
1.26 [0.42-3.76] |
0.676 |
|
Eats green leafy vegetables |
|
|
|
|
|
Yes |
40 (7.8) |
18 (18.6) |
1.00 [reference] |
|
|
No |
475 (92.2) |
79 (81.4) |
0.41 [0.19-0.88] |
0.023* |
|
Consumes Sobolo |
|
|
- |
|
|
Yes |
99 (17.4) |
28 (27.5) |
1.00 [reference] |
|
|
No |
471 (82.6) |
74 (72.6) |
0.56 [0.31-0.98] |
0.043* |
|
Does extra physical activities |
|
|
|
|
|
Yes |
281 (49.3) |
64 (62.8) |
1.00 [reference] |
|
|
No |
289 (50.7) |
38 (37.3) |
0.70 [0.17-2.88] |
0.618 |
|
Hypertension |
|
|
|
|
|
No |
62 (84.93) |
275 (92.91) |
1.00 [reference] |
|
|
Yes |
11 (15.07) |
21 (7.09) |
1.71 [1.21-2.99] |
0.031* |
AOR=Crude Odds Ratio
Table 5: Association Between Patients’ Factors and Asymptomatic COVID 19 Status, Ghana, 2020
Discussion
This study focused on COVID-19 patients in Ghana in 2020, revealing critical understanding on predictors for symptomatic presentation of the disease. Majority of participants were males who were working in the informal sector, consistent with similar demographic patterns noted in other global and regional COVID-19 studies (6,7).
The study confirmed a high asymptomatic proportion of 85%, though slightly lower, finding compares with the 93% reported earlier by the GHS. This finding significantly differs from the lower asymptomatic percentage of 15.6% from a systematic review and meta-analysis (8). Factors that protected patients from showing COVID-19 related symptoms were patients’ formal education [Primary, JHS, SHS/vocational]. Patients having three (3) meals in a day, adding green leafy vegetables to meal, drinking hibiscus flower tea (“Sobolo”) and indulging in extra physical activities. However, patients who had hypertension were more likely to show symptom(s) of the disease than those who had no hypertension.
Patients who had attained Primary, JHS and SHS education were less likely to come up with COVID-19 related symptoms. As one advances in formal education, they are more likely to be health conscious and adopt healthy behaviour like proper hydration (9) adding green leafy vegetables to meals which also proved significant in this study. They are also more likely to seek treatment for any underlining health conditions making them less likely to show symptoms of the disease. Though acquiring tertiary education rendered patients less likely to come up with symptoms, its strength of association was not significant. This might have resulted from the overly sedentary lifestyle this class of patients are likely to be indulged in. Tertiary education mostly places its achievers in white colored jobs thereby reducing the amount of time for physical activities. Persons in this class are also more likely to come up with non-communicable diseases such as hypertension, which was significantly associated with symptomatic cases by this study.
Similarly, dietary habits, including the consumption of green leafy vegetables and hibiscus flower tea ("Sobolo"), demonstrated a protective association against symptomatic COVID-19 presentation (10). The potential role of dietary factors in modulating immune responses and disease outcomes has been documented in various infectious diseases (11). Patients who reported to be consuming this tea on daily basis were less likely to show symptoms than those who did not. This finding might have resulted from the rich antioxidant content of this special flower. Hibiscus tea is made by brewing dried petals of hibiscus flowers and has been known to have significant antioxidant and hypolipidemic properties (12). But the use of herbal drugs in the treatment of COVID-19 should be done with great caution (13). Though no documented evidence exists on the use of hibiscus tea for management of SARS-CoV-2, the flower is proven to have a high pharmacological potential to treat disorders such as hypertension, pyrexia and many forms of cancers (14). This makes further research on hibiscus necessary to inform decision on the pandemic control.
Patients having three (3) meals in a day and those who added green leafy vegetables to meals were less likely to present with symptoms. Adequate nutrition remains one of the crucial building blocks of one’s immune system. Persons who can have three (3) meals in the day are more likely to keep a good immune system than those who eats less. Green leafy vegetables on the other hand are mostly packed with vitamins and antioxidants which can protect consumers against worse outcomes of diseases.
This study found hypertension as a precursor for COVID-19 symptoms, this might have resulted from the already moribund state of their health. This finding agrees with the study of (15). Some hypertensives already suffer symptoms such as headaches, difficulties in breathing due to restricted blood flow to the lungs. This normally results from difficulties encountered as the right side of the heart pushes blood through the lungs. Having SARS- CoV-2 as a co-morbidity worsens the already malfunctioning airways thereby leading to increase respiratory difficulties (5,15). Finding compares with that of a similar study carried out in South Korea where asymptomatic patients with cardiovascular disease were more likely to progress into symptomatic than those without (15). Early identification and adequate management of hypertension among COVID-19 patients is key for minimizing adverse outcomes of the disease.
Conclusion
This study found an asymptomatic proportion of 85%, slightly lower than reported (93%) by the GHS. Factors that protected patients from showing COVID-19 related symptoms were patient's formal education, having three (3) meals in a day, adding green leafy vegetables to meal, performing extra physical activity, and drinking hibiscus flower tea ("Sobolo"). However, patients who had hypertension were more likely to show symptom(s) of the disease than those who had no hypertension. Elucidating factors influencing asymptomatic COVID-19 presentation in Ghana underscores the need for tailored interventions addressing these determinants. By integrating these findings into public health policies and awareness campaigns, a concerted effort can be made to curb the impact of COVID-19 in Ghana and similar contexts. This study, therefore, recommends that control efforts at COVID-19 should include education on adding green leafy vegetables to meals, and hypertension prevention and appropriate management. Designated state institutions and the research fraternity should carry out further studies to give guidance on the use of hibiscus flower.
Acknowledgements
We are grateful to all who made this study possible. Our special appreciation goes to the leadership of the Ghana Health Service and supporting partners. We also give special thanks to the patients who spent valuable time with us during the interviews amidst their ill health. Finally, this study would not have been successful without the active participation of residents of the Ghana Field Epidemiology and Laboratory Training Programme (GFELTP) who served as data collectors for this study. We are grateful for the commitment throughout the data collection of the study.
Funding
No research grant/funding was awarded this study. The study was self-funded by the Ghana Health Service through resources earmarked for COVID-19 management by the government of Ghana and partners.
References
- Nishiura, H., Kobayashi, T., Miyama, T., Suzuki, A., Jung,S. M., Hayashi, K., ... & Linton, N. M. (2020). Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). International journal of infectious diseases, 94, 154-155.
- Workman, J. (2020). The proportion of COVID-19 cases that are asymptomatic in South Korea: Comment on Nishiura et al. International Journal of Infectious Diseases, 96, 398.
- He, D., Zhao, S., Lin, Q., Zhuang, Z., Cao, P., Wang, M. H., & Yang, L. (2020). The relative transmissibility of asymptomatic COVID-19 infections among close contacts. International Journal of Infectious Diseases, 94, 145-147.
- Miyamae, Y., Hayashi, T., Yonezawa, H., Fujihara, J., Matsumoto, Y., Ito, T., ... & Ishii, K. (2020). Duration of viral shedding in asymptomatic or mild cases of novel coronavirus disease 2019 (COVID-19) from a cruise ship: A single-hospital experience in Tokyo, Japan. International Journal of Infectious Diseases, 97, 293-295.
- Shi, S., Qin, M., Shen, B., Cai, Y., Liu, T., Yang, F., ...& Huang, C. (2020). Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA cardiology, 5(7), 802-810.
- Sacchetto, C., Daniel, E., Danquah, M., & Telli, H. (2020). Informality and COVID-19 in sub-Sarahan Africa.
- Kansiime, M. K., Tambo, J. A., Mugambi, I., Bundi, M., Kara, A., & Owuor, C. (2021). COVID-19 implications on household income and food security in Kenya and Uganda: Findings from a rapid assessment. World development, 137, 105199.
- He, J., Guo, Y., Mao, R., & Zhang, J. (2021). Proportion of asymptomatic coronavirus disease 2019: A systematic review and metaâ?analysis. Journal of medical virology, 93(2), 820-830.
- Popkin, B. M., D'Anci, K. E., & Rosenberg, I. H. (2010). Water, hydration, and health. Nutrition reviews, 68(8), 439- 458.
- Mireku-Gyimah, N. A., Donkor, P. O., Kitcher, C., Sarkodie,J. A., Bekoe, E. O., Boateng, O. K., & Nyarko, A. K. (2021). Response to Covid-19 disease in Ghana: a review of the herbs. Journal of Natural Remedies, 283-290.
- Serban, C., Sahebkar, A., Ursoniu, S., Andrica, F., & Banach, M. (2015). Effect of sour tea (Hibiscus sabdariffa L.) on arterial hypertension: a systematic review and meta-analysis of randomized controlled trials. Journal of hypertension, 33(6), 1119-1127.
- Ochani, P. C., & D’Mello, P. (2009). Antioxidant and antihyperlipidemic activity of Hibiscus sabdariffa Linn. leaves and calyces extracts in rats.
- Yang, Y. (2020). Use of herbal drugs to treat COVID-19 should be with caution. The Lancet, 395(10238), 1689- 1690.
- Faraji, M. H., & Tarkhani, A. H. (1999). The effect of sour tea (Hibiscus sabdariffa) on essential hypertension. Journal of Ethnopharmacology, 65(3), 231-236.
- Aslanbeigi, F., Rahimi, H., Malekipour, A., Pahlevani, H., Najafizadeh, M., Ehteram, H., ... & Kashani, H. H. (2023). Association between hypertension and clinical outcomes in COVID-19 patients: a case-controlled study. Annals of Medicine and Surgery, 85(7), 3258-3263.
- Chang, M. C., Park, Y. K., Kim, B. O., & Park, D. (2020).Risk factors for disease progression in COVID-19 patients.BMC infectious diseases, 20, 1-6.