



Case Report - (2022) Volume 7, Issue 1
Heart Involvement in Hemoglobinopathies: Two Case Reports and Brief Review of Literature
Received Date: Feb 15, 2022 / Accepted Date: Feb 20, 2022 / Published Date: Feb 25, 2022
Copyright: ©Wael Yaakoubi, et al This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Wael Yaakoubi, Manel Ben Hlima, Sana Ouali, Fathia Mghaith, Med Sami Mourali (2022) Heart Involvement in Hemoglobinopathies: Two Case Reports and Brief Review of Literature. Cardio Open, 7(1): 192-194.
Abstract
Hereditary haemoglobin disorders, also termed haemoglobinopathies, include mainly beta-thalassemia and sickle cell disease and represent the most common monogenic disorders in human. Cardiac complications are still a leading cause of mortality and morbidity in patients with haemoglobinopathy, have dramatically reduced in patient populations receiving modern regular therapy and follow-up.
Keywords
Heart Failure, Hemoglobinopathies, Mortality
Introduction
Τhe two main determinants of cardiovascular phenotype in haemoglobinopathy patients are the underlying molecular defect responsible for the main disease and the therapy applied for its management. The spectrum of cardiovascular manifestations in haemoglobinopathies is wide and includes ventricular dysfunction, pulmonary hypertension, thromboembolic events. We report a case of thalassemia and one of sickle cell disease having different clinic phenotype with brief literature review.
Case1
A patient 32-year-old male who was receiving periodic trans- fusions with intermittent chelation therapy for Cooley's Anae- mia came to our clinic with complaint of dyspnoea on exertion (DOE) in the past two years. The patient was followed up at the haematology department. He had a splenectomy at three years old. On the physical examination the patient had a global heart failure chart, high abundance ascites and hepatomegaly. He was in rapid atrial fibrillation. After treatment of congestion and slowing atrial fibrillation, the patient was explored by an echocardiography. Severe LV systolic dysfunction with a LVEF of about 20%; mitral regurgitation up to moderate degree was observed in Figure 1. The right ventricle is very dilated with massive and laminar tricuspid insufficiency due to lack of coap- tation of the cusps thus creating a tricuspid hiatus. A restrictive filling pattern in both ventricles with both ventricular systol- ic dysfunctions were evident in this patient, also a lower right ventricular function: free wall TDI peak systolic velocity was 7 cm/sec. The patient was probed by MRI revealing advanced he- patic and cardiac hemochromatosis. Endocrine pancreas is also reached in view of high glycaemic dosage relating to secondary diabetes. Our patient died while in hospital because he had an electrical storm.
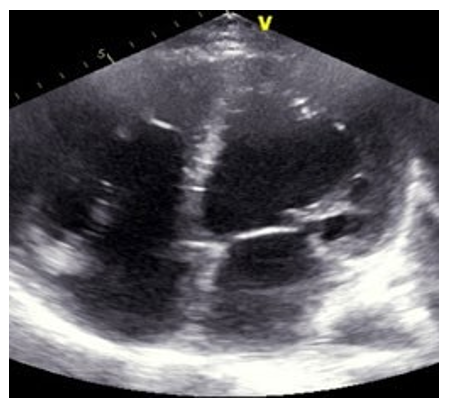
Figure 1: Echocardiography, Four Chamber 2D Apical View, Biventricular Dilated Cardiomyopath
Case 2
A patient 28-year-old male who was receiving periodic trans- fusions with intermittent chelation therapy for Sickle Cell Dis- ease (SCD) came to our clinic with complaint of dyspnoea on exertion (DOE) in the past two years. The patient was followed up at the haematology department. On the physical examination the patient had distended jugular veins, high abundance ascites and hepatomegaly. At the electrocardiogram revealed a regular rhythm and a completely right bundle brunch block. At echo- cardiography, LVEF was about 60%. The right ventricle is very dilated in Figure 2 with massive tricuspid insufficiency due to a diastasis in tricuspid valve.

Figure 2: Cardiac CT Scan: Very Dilated Right Ventricle in a SCD Patient
A lower right ventricular function: free wall TDI peak systol- ic velocity was 4 cm/sec. Estimation of systolic pulmonary ar- tery pressure from tricuspid insufficiency was about 120 mmHg which was very high and supra-systemic. The patient was ex- plored by cardiac CT-scan revealing advanced pulmonary hemo- chromatosis in Figure 3, no pulmonary emboli and very enlarged right cardiac cavities. Our patient died of acute chest syndrome during hospitalization [1].
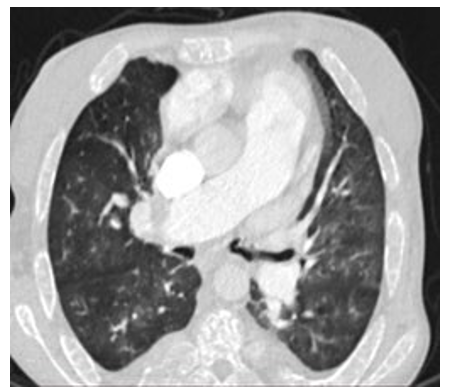
Figure 3: Pulmonary CT scan, Pulmonary Hemochromatosis in a SCD Patient
Discussion
Thalassemia heart disease involves mainly left ventricular dys- function caused by transfusion-induced iron overload. In addition to the left ventricular abnormalities right ventricular dysfunction represents a common, yet less well explored complication in the cardiopulmonary spectrum of the disease. Biventricular dilated cardiomyopathy is still considered as the leading cause of mor- tality in patients with beta thalassemia major [2]. In B-Thalas- semia, the defect in haemoglobin is quantitative, characterized by a reduction or total depletion of ð?½ chain synthesis, and the severity of ð?½ chain deficiency determines the clinical pheno- type, which extends from the severe and transfusion-dependent thalassaemia major to the milder and often transfusion-indepen- dent thalassaemia intermedia [3]. The heart takes up physiologic amounts of iron through transferrin receptors, but this process is tightly regulated and does not lead to iron overload. When transferrin-binding capacity is exceeded, circulating low molec- ular weight non-transferrin-bound iron (NTBI) species appear. NTBI is oxidatively active and can enter through nonspecific, poor-regulated cation channels in the heart, leading to cardiac iron overload [4]. Pulmonary hypertension (PH) in thalassemia is associated with vasoconstriction, vascular smooth muscle proliferation, and irregular endothelium in pulmonary arteries with associated thrombosis. These conditions all contribute to luminal narrowing, and eventual right ventricular failure. It in- cludes plexiform and concentric medial hyperplastic pulmonary vascular lesions, and in situ pulmonary artery thrombosis [5,6].
These pulmonary vascular abnormalities may have resulted from chronic embolic disease in other patients [5]. Advanc- ing age and a history of splenectomy are major risk factors for PH in this population [7,8]. Another phenomenon can explain this phenomenon as the process of haemolysis disables the ar- ginine-nitric oxide pathway through the simultaneous release of erythrocyte arginase and cell-free haemoglobin. Both nitric oxide and its obligate substrate arginine are rapidly consumed [9]. Outcome of heart failure, in advanced cardiac iron overload states, is dismal [10-12]. Compared to reported 3-month mor- tality rate of 58% in the pre-chelation era, recent findings indi- cate an improved prognosis over older series. Five-year survival was 48% and positively associated with left ventricular systolic function. All deaths occurred among patients with biventricular cardiomyopathy, shortly after involvement. Such improved sur- vival is explained by the widespread use of chelation treatment and possibly also by better management of anaemia and use of angiotensin-converting enzyme inhibitors. Although LV Iron overload cardiomyopathy is a leading cause of death in patients with thalassaemia major this complication appears to be uncom- mon in SCD patients. Left ventricular dysfunction due to sickle cell disease is rare [13].
In SCD, the defect in haemoglobin is qualitative, as a substi- tution at the sixth amino acid residue in the ð?½ chain results in synthesis of an abnormal haemoglobin, termed haemoglobin S, instead of the normal haemoglobin A [14]. Left ventricular systolic dysfunction is uncommon in patients with SCD: A me- ta-analysis of 19 controlled case studies has shown similar LV ejection fraction (LVEF) in homozygous S patients compared to healthy controls [15]. Accordingly, the prevalence of an LVEF < 50% is low, ranging from 0% to 2.5% in ultrasound cohorts’ studies and 0% to 4% in smaller CMR studies [16,17]. SCD-re- lated PH involves several mechanisms. First, as pulmonary pressure is the product of flow and pulmonary vascular resis- tances, high cardiac output in SCD induces elevated pulmonary pressure whether pulmonary vascular resistances are altered or not [18,19]. Second, chronic volume overload might lead to LV failure and subsequent pulmonary venous hypertension [20,21]. Third, intravascular haemolysis could induce pulmonary arteri- al vasculopathy mainly driven by nitric oxide scavenging due to free plasma haemoglobin [22]. Finally, several other mecha- nisms may participate including, chronic hypoxaemia, post-em- bolic PH, SCD-related lung injury, chronic liver disease, and asplenia.
In SCD, the pulmonary vascular bed is commonly affected [23]. Pneumonia may be difficult to distinguish from pulmonary in- farction and both may coexist. Intravascular sickling may cause pulmonary vascular occlusion in the absence of radiologic changes, and in some patient’s bone marrow and fat released from infarcted bone may embolize to the lungs [24]. In the au- topsy series of Gerry et al, 30% of adults and 22% of children had right ventricular hypertrophy. Three of these patients had had right ventricular failure, considered to be due to cor pulmo- nale [25].
Abbreviations
DOE: Dyspnoea on Exertion
MRI: Magnetic Resonance Imaging
SCD: Sickle Cell Disease
LVEF: Left Ventricle Ejection Fraction
MBT: Major Beta-thalassemia
Conclusion
The main cardiac involvement during major beta thalassemia is left ventricular dysfunction or in extreme cases biventricular di- lated cardiomyopathy on the other hand sickle cell disease main- ly causes right ventricular dilatation and dysfunction secondary to sickle cell lung pathology. A major near-term issue to address is the establishment of criteria for early disease-specific treat- ment of patients with MBT and SCD to avoid cardiovascular complications
References
- Grisaru, D., Rachmilewitz, E. A., Mosseri, M., Gotsman, M., Lafair, J. S., & et al. (1990). Cardiopulmonary assess- ment in beta-thalassemia major. Chest, 98(5), 1138-1142.
- Levy, R. I., & Moskowitz, J. (1982). Cardiovascular re- search: decades of progress, a decade of promise. Science, 217(4555), 121-129.
- Rund, D., & Rachmilewitz, E. (2005). β-Thalassemia. New England Journal of Medicine, 353(11), 1135-1146.
- Wood, J. C. (2009). Cardiac complications in thalassemia major. Hemoglobin, 33(sup1), S81-S86.
- Sonakul, D., Pacharee, P., & Thakerngpol, K. (1988). Patho- logic findings in 76 autopsy cases of thalassemia. Birth De- fects Original Article Series, 23(5B), 157-176.
- Morris, C. R., Gladwin, M. T., & Kato, G. J. (2008). Nitric oxide and arginine dysregulation: a novel pathway to pul- monary hypertension in hemolytic disorders. Current mo- lecular medicine, 8(7), 620-632.
- Atichartakarn, V., Likittanasombat, K., Chuncharunee, S., Chandanamattha, P., Worapongpaiboon, S., & et al. (2003). Pulmonary arterial hypertension in previously splenecto- mized patients with β-thalassemic disorders. International journal of hematology, 78(2), 139-145.
- Phrommintikul, A., Sukonthasarn, A., Kanjanavanit, R., & Nawarawong, W. (2006). Splenectomy: a strong risk factor for pulmonary hypertension in patients with thalassaemia. Heart, 92(10), 1467-1472
- Rother, R. P., Bell, L., Hillmen, P., & Gladwin, M. T. (2005). The clinical sequelae of intravascular hemolysis and extra- cellular plasma hemoglobin: a novel mechanism of human disease. Jama, 293(13), 1653-1662
- ENGLE, M. A., ERLANDSON, M., & SMITH, C. H.(1964). Late cardiac complications of chronic, severe, refractory anemia with hemochromatosis. Circulation, 30(5), 698-705.
- Engle, M. A. (1964). Cardiac involvement in Cooley's ane- mia. Annals of the New York Academy of Sciences, 119(2), 694-702.
- Felker, G. M., Thompson, R. E., Hare, J. M., Hruban, R. H., Clemetson, D. E., & et al. (2000). Underlying causes and long-term survival in patients with initially unexplained car- diomyopathy. New England Journal of Medicine, 342(15), 1077-1084.
- Falk, R. H., & Hood, W. B. (1982). The heart in sickle cell anemia. Archives of internal medicine, 142(9), 1680-1684.
- Rees, D. C., Williams, T. N., & Gladwin, M. T. (2010). Sickle-cell disease. The Lancet, 376(9757), 2018-2031.
- Poludasu, S., Ramkissoon, K., Salciccioli, L., Kamran, H., & Lazar, J. M. (2013). Left ventricular systolic function in sickle cell anemia: a meta-analysis. Journal of Cardiac Fail- ure, 19(5), 333-341.
- Desai, A. A., Patel, A. R., Ahmad, H., Groth, J. V., Thiru- voipati, T., & et al. (2014). Mechanistic insights and charac- terization of sickle cell disease–associated cardiomyopathy. Circulation: Cardiovascular Imaging, 7(3), 430-437.
- Wood, J. C., Tyszka, J. M., Carson, S., Nelson, M. D., & Coates, T. D. (2004). Myocardial iron loading in transfu- sion-dependent thalassemia and sickle cell disease. Blood, 103(5), 1934-1936.
- Mushemi-Blake, S., Melikian, N., Drasar, E., Bhan, A., Lunt, A., & et al. (2015). Pulmonary haemodynamics in sickle cell disease are driven predominantly by a high-out- put state rather than elevated pulmonary vascular resistance: a prospective 3-dimensional echocardiography/Doppler study. PLoS One, 10(8), e0135472.
- Caughey, M. C., Hinderliter, A. L., Jones, S. K., Shah, S. P., & Ataga, K. I. (2012). Hemodynamic characteristics and predictors of pulmonary hypertension in patients with sickle cell disease. The American journal of cardiology, 109(9), 1353-1357.
- Junqueira, F. P., Fernandes, J. L., Cunha, G. M., TA Kubo, T., MAO Lima, C., & et al. (2013). Right and left ventricu- lar function and myocardial scarring in adult patients with sickle cell disease: a comprehensive magnetic resonance as- sessment of hepatic and myocardial iron overload. Journal of Cardiovascular Magnetic Resonance, 15(1), 1-7.
- Fonseca, G. H. H., Souza, R., Salemi, V. M. C., Jardim, C.V. P., & Gualandro, S. F. M. (2012). Pulmonary hyperten- sion diagnosed by right heart catheterisation in sickle cell disease. European Respiratory Journal, 39(1), 112-118.
- Farmakis, D., & Aessopos, A. (2011). Pulmonary hyper- tension associated with hemoglobinopathies: prevalent but overlooked. Circulation, 123(11), 1227-1232.
- Bromberg, P. A. (1974). Pulmonary aspects of sickle cell disease. Archives of Internal Medicine, 133(4), 652-657.
- Baroldi, G. (1969). High resistance of the human myocardi- um to shock and red blood cell aggregation (sludge). Cardi- ology, 54(5), 271-277.
- Gerry Jr, J. L., Bulkley, B. H., & Hutchins, G. M. (1978). Clinicopathologic analysis of cardiac dysfunction in 52 pa- tients with sickle cell anemia. The American journal of car- diology, 42(2), 211-216.