




Case Report - (2026) Volume 5, Issue 1
Geniculate Nerve Cryoanalgesia for Chronic Knee Pain: A Retrospective Study
2Azienda Ospedaliera Universitaria Università degli Studi della Campania, Luigi Vanvitelli, Naples, Italy, Dipartimento di medicina di precision, Italy
3Saint Camillus International University of Health and Medical Sciences, Rome, Italy
4University of Salerno, Italy
Received Date: Oct 31, 2025 / Accepted Date: Dec 11, 2025 / Published Date: Jan 30, 2026
Copyright: ©2026 Francesco Saturno, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Saturno, F., Monaco, G., Salerno, A., Cianciola, A., Secondulfo, C., et al. (2026). Geniculate Nerve Cryoanalgesia for Chronic Knee Pain: A Retrospective Study. J Surg Care, 5(1), 01-04.
Abstract
Background: Knee osteoarthritis represents one of the leading causes of disability in older adults. Minimally invasive percutaneous treatments, including cryoanalgesia of the geniculate nerves, are emerging as valid alternatives for patients who are not candidates for surgery or who do not respond to infiltrative therapy.
Objectives: To evaluate the safety and medium-term efficacy of geniculate nerve cryoanalgesia in patients with refractory knee pain.
Methods: A retrospective review of all cryoanalgesia procedures performed on geniculate nerves between 2023 and 2024 was conducted. Pain outcomes (VAS) were collected at 6 months and 1 year. Complications and need for repeat procedures were recorded.
Results: Fifty patients were included. At 6 months, 86% (n=43) reported VAS <3. Seven patients experienced pain recurrence; four underwent repeat cryoanalgesia, with only one maintaining VAS >5. At 1 year, nine patients reported recurrence, and five of them underwent a repeat procedure, all reporting VAS <5. No major complications occurred. A transient increase in pain during the first 7–10 days was reported in a minority of cases.
Conclusion: Cryoanalgesia of the geniculate nerves is a safe and promising minimally invasive technique for managing refractory knee pain in high-risk or non-surgical candidates. Larger prospective studies are needed to assess long-term outcomes and potential opioid-sparing effects.
Introduction
Knee osteoarthritis is highly prevalent in adults older than 45 years and is a leading cause of functional limitation and disability. Despite the availability of pharmacological and infiltrative treatments, many patients continue to suffer from chronic pain due to the limited durability of these therapies. Cryoanalgesia has emerged as a minimally invasive option capable of disrupting pain transmission while maintaining a strong safety profile. The geniculate nerves, which supply sensory innervation to the knee joint, have become frequent targets for percutaneous ablative procedures, particularly in individuals not eligible for surgery.
Materials and Methods
A retrospective analysis was performed on all patients undergoing geniculate nerve cryoanalgesia from 2023 to 2024. Inclusion criteria consisted of chronic knee pain due to osteoarthritis refractory to conservative and infiltrative therapies. Cryoanalgesia was performed using combined ultrasound and fluoroscopic guidance. Pain outcomes (VAS) and complications were assessed at two time points: 6 months and 1 year.Results
A total of 50 patients were included. Pain decreased significantly in the majority of subjects, with 86% reporting VAS <3 at 6 months. Recurrence occurred in 7 patients at 6 months and 9 patients at 1 year; repeat cryoanalgesia restored satisfactory analgesia in nearly all. No major complications were observed.Discussion
Our retrospective analysis confirms that percutaneous cryoanalgesia of the geniculate nerves provides meaningful and durable pain relief for patients with knee osteoarthritis who are not candidates for surgical intervention. The efficacy observed at both 6-month and 1-year follow-ups aligns with existing literature supporting the use of cryoneurolysis in chronic pain syndromes. One of the major strengths of cryoanalgesia is its mechanism of action: unlike thermal neurolysis (radiofrequency or microwave ablation), cryoablation induces Wallerian degeneration without damaging the perineurium or epineurium. This selective preservation of the nerve sheath allows for predictable regeneration of axons while limiting the risk of neuroma formation or neuropathic flare. This regenerative potential is particularly relevant for elderly patients or those with multiple comorbidities, in whom safety is a priority. In our series, transient pain flare during the first postoperative week was noted in several patients. This has been well described in the literature and likely reflects an inflammatory response to axonal freezing followed by thaw cycles.
Importantly, no major adverse events such as hematoma, infection, nerve injury, or persistent paresthesia were observed, confirming the safety profile of the technique. The recurrence of pain at 1 year in a minority of patients should be interpreted in the context of nerve regeneration. Given the reversible nature of cryoneurolysis, analgesia is expected to diminish over time as axons regrow. Our findings highlight that repeat cryoanalgesia is effective and safe, suggesting that the procedure can be integrated into long-term management strategies for chronic knee pain. When compared with genicular nerve radiofrequency ablation, cryoanalgesia may offer several advantages, including reduced risk of neuritis, more comfortable patient experience due to absence of burning sensations during lesioning, and the potential for larger ice-ball formation allowing broader coverage of sensory branches. However, direct comparative trials are lacking, and future research should explore differential efficacy, duration, and safety among these modalities.
Another important direction for future investigation concerns opioid consumption. As the burden of opioid overuse remains a major public health issue, minimally invasive pain interventions capable of providing sustained analgesia—such as cryoanalgesia—may meaningfully reduce the need for chronic opioid therapy. Our next studies will specifically evaluate opioid-sparing outcomes. Overall, the results from our series reinforce the role of cryoanalgesia as a viable, safe, and repeatable alternative for managing refractory knee osteoarthritis pain, especially in surgically high-risk or elderly populations. Larger prospective studies with control groups are needed to confirm these findings and guide clinical decision-making [1-13].

Figure 1: Intraoperative Image Illustrating Needle Placement for Geniculate Nerve Targeting

Figure 2: Fluoroscopic Confirmation of Geniculate Nerve Anatomical Targets
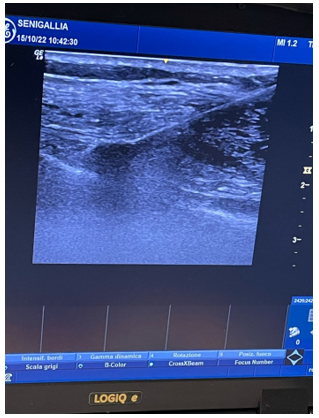
Figure 3: Ultrasound-Guided Approach to the Superior Medial Geniculate Nerve
References
- Litwic, A., Edwards, M. H., Dennison, E. M., & Cooper, C. (2013). Epidemiology and burden of osteoarthritis. British Medical Bulletin, 105(1), 185–199.
- Kolasinski, S. L., et al. (2020). 2019 ACR/AF guideline for the management of knee osteoarthritis. Arthritis & Rheumatology, 72(2), 220–233.
- Trescot, A. M. (2003). Cryoanalgesia in interventional pain management. Pain Physician, 6, 345–360.
- Gabriel, R. A., & Ilfeld, B. M. (2019). Cryoneurolysis for acute and chronic pain. Anesthesiology, 131, 1191–1204.
- Lloyd, J. W., et al. (1976). Cryoanalgesia: A new approach. Anesthesia & Analgesia, 55, 550–556.
- Prologo, J. D., et al. (2021). Cryoanalgesia for chronic non-cancer pain: Systematic review. Skeletal Radiology, 50, 207–218.
- Callström, M. R., et al. (2020). Image-guided percutaneous cryoablation. Radiology, 294, 378–388.
- Manchikanti, L., et al. (2002). Interventional techniques for chronic pain. Pain Physician, 5, 46–62.
- Tran, J., & Peng, P. W. H. (2014). Genicular nerve branches: Anatomical study. Regional Anesthesia & Pain Medicine, 39, 170–175.
- McCormick, Z., et al. (2017). Genicular nerve RFA for chronic knee pain. Pain Medicine, 18, 736–746.
- Bellini, M., & Barbieri, M. (2021). Percutaneous cryoablation for chronic knee pain. Pain Physician, 24, E257–E266.
- Samuelson, S., et al. (2020). Ultrasound-guided genicular nerve interventions. AJR American Journal of Roentgenology, 214, 175–182.
- Ilfeld, B. M., et al. (2021). Cryoneurolysis: Expected postprocedural course. Regional Anesthesia & Pain Medicine, 46, 965–972.