



Review Article - (2019) Volume 4, Issue 3
FMTVDM Quantitative Imaging Replaces Current Qualitative Imaging for Coronary Artery Disease and Cancer, Increasing Diagnostic Accuracy and Providing Patient Specific, Patient-Directed Treatment
2Eastern Virginia Medical School Norfolk virgina, USA
3Sebec Consulting & Media Rock Hill, South Carolina, USA
Received Date: Aug 13, 2019 / Accepted Date: Aug 23, 2019 / Published Date: Aug 27, 2019
Copyright: ©Richard M Fleming, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The time for practicing medicine by merely looking at a qualitative picture of someone’s heart, chest or mammogram, or by taking a patients blood sample to measure cholesterol or inflammation levels and then letting the Doctor decide if they think you have heart disease or cancer, has ended. So too has the period of time for treating someone merely based upon mammography (x-rays), CT, MRI, PET, SPECT/planar imaging or any other test that requires your physician to qualitatively interpret what they think they see, and then decide you do or don’t have a medical problem.
Keywords
FMTVDM, Quantification, Nuclear Medicine, Nuclear Cardiology, Cancer, FDA, uBiome, Biomarkers
The time for practicing medicine by merely looking at a qualitative picture of someone’s heart, chest or mammogram, or by taking a patients blood sample to measure cholesterol or inflammation levels and then letting the Doctor decide if they think you have heart disease or cancer, has ended. So too has the period of time for treating someone merely based upon mammography (x-rays), CT, MRI, PET, SPECT/planar imaging or any other test that requires your physician to qualitatively interpret what they think they see, and then decide you do or don’t have a medical problem.
In 2018, CMS, ASNC and the SNMMI all called for improvements in diagnostic testing. These three groups emphasized the need to develop and implement quantitative imaging to replace the current qualitative imaging, with the primary endpoint being to reduce clinical mistakes and save time, money and lives. To address these clinical errors, the first author began working in 1989 on the intrinsic errors within our diagnostic tests, beginning with coronary arteriography [1].
Continued work lead to the discovery and development of both the “Inflammation and Heart Disease” and “Angina” theories, resulting in a shift in thinking that cholesterol was the sole cause of heart disease, to the understanding that coronary artery disease (CAD) is an inflammatory process which builds up in the walls of the arteries of the heart, making the arteries less able to relax (dilate), to delivery more blood to regions of the heart when needed, thereby producing angina [2-5].
By 1999, the first author had discovered that several companies were misrepresenting to the FDA how their drugs and nuclear cameras worked. As information continued to accumulate, the first author not only discovered that people were receiving more radiation than required, but that the sale of this increased amount of radioactive material, derived from enriched uranium, was resulting in a 2-3 fold increase in profits for the companies making and selling them; all the while concurrently missing critical heart disease, in some 20-30% of cases.
In 2018, the FDA asked the primary author to report these misrepresentations, along with misinformation being supplied by uBiome and other companies regarding biomarkers (FDA- 2018-P-3102; FDA-2018-D-4267-0002). In addition to what was discussed above, these reports detailed the discovery that the nuclear cameras being used to diagnose heart disease were not actually measuring what physicians thought the cameras were measuring. As a result and without knowing critical decision-making information was being lost, doctors were being asked to diagnose the presence or absence of heart disease and cancer, critical to the care and treatment of patients.
The Fleming Method for Tissue and Vascular Differentiation and Metabolism (FMTVDM) using same state single or sequential quantification comparisons [6].
Following 18-years of research and investigation, The Fleming Method for Tissue and Vascular Differentiation and Metabolism (FMTVDM) was patented (#9566037). By quantitatively measuring changes in regional blood flow and metabolism, FMTVDM had not only achieved what CMS, ASNC and SNMMI had called for, but then some. FMTVDM does more than merely ask if heart disease or cancer is present; it actually measures the changes, which occur as healthy tissue transitions through the disease process over time. This ability changes the question from does someone have disease, to where do they reside on the Health-Spectrum?
Given the ability to now measure this spectrum of health (Figure 1) for each individual, patients no longer will simply be told yes, you have disease, no, you don’t; but rather to what extent is there or isn’t there a problem; thus allowing patients and their health care providers to make patient-specific, patient-directed treatment decisions based upon objective, measureable outcomes.
Since 2018, FMTVDM has been discussed in more than 40 peer reviewed papers and presented at multiple medical conferences.
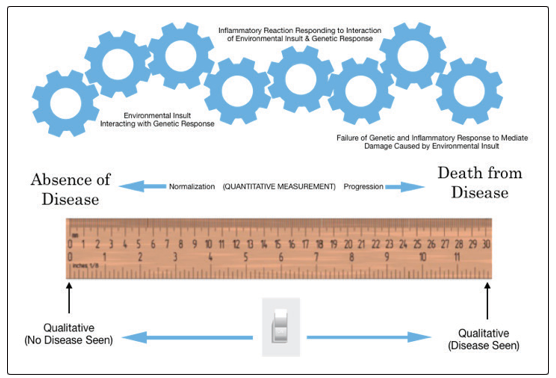
Figure 1: FMTVDM Quantification of the Health-Spectrum for Cancer.
Conclusion
Errors intrinsic to qualitative imaging, the over utilization of biomarkers, excessive sales and dosing of radioisotopes, and incorrectly calibrated nuclear cameras, have all resulted in errors in (a) the ability to correctly identify the presence or absence of a disease process; including coronary artery disease (Figure 2) and cancer – including breast cancer, and (b) the inability to quantitatively define transitional changes in health [7].
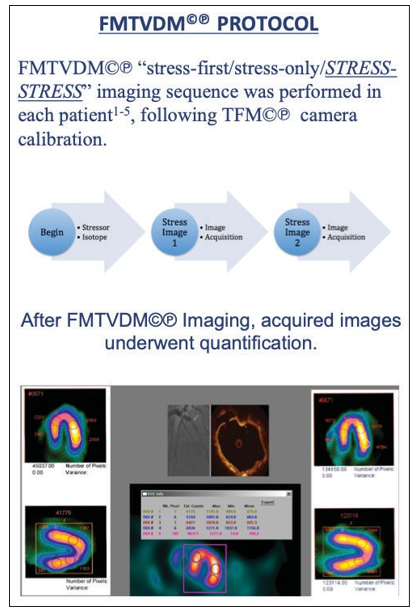
Figure 2: FMTVDM measures critical coronary artery disease missed by qualitative human interpretation
FMTVDM provides a patented method for quantitatively correcting these problems. Not only does it provide enhanced diagnostic capabilities called for by CMS, ASNC and the SNMMI, but by quantifying tissue specific differences in metabolism and regional blood flow, it provides measurement of (a) earlier transitional changes and (b) assessment of treatment responses; allowing physicians to provide patient-specific, patient-directed treatment.
COI: FMTVDM was issued to the primary author. All figures reproduced with expressed consent of the first author.
References
- Fleming RM, Kirkeeide RL, Smalling RW, Gould KL (1991) Patterns in Visual Interpretation of Coronary Arteriograms as Detected by Quantitative Coronary Arteriography. J Am Coll Cardiol 18: 945- 951.
- Fleming RM (2001) Coronary Artery Disease is More than Just Coronary Lumen Disease. Amer J Card 88: 599-600.
- Fleming RM (1999) Chapter 29. Atherosclerosis: Understanding the relationship between coronary artery disease and stenosis flow reserve. Textbook of Angiology. John C Chang Editor Springer-Verlag, New York, 381-387.
- Fleming RM (1999) Chapter 64. The Pathogenesis of Vascular Disease. Textbook of Angiology. John C Chang Editor, Springer- Verlag New York, 787-798.
- Fleming RM (2003) Angina and coronary Ischemia are the result of coronary regional Blood Flow Differences. J Amer Coll Angiol 1: 127-142.
- The Fleming Method for Tissue and Vascular Differentiation and Metabolism (FMTVDM) using same state single or sequential quantification comparisons. Patent Number 9566037. Issued 02/14/2017.
- Fleming RM, Fleming MR, Chaudhuri TK (2019) Quantitative stress-redistribution sequential imaging optimises MPI with the lowest dose of radiation per patient. BMJ Open Quality, 8: e000774