
Journal of Clinical Pediatrics and Child Care Research(JCPCCR)
ISSN: 2832-2584 | DOI: 10.33140/JCPCCR
Impact Factor: 1.10



Research Article - (2024) Volume 5, Issue 1
Fetal Macrosomia at Gabriel Toure Hospital: Prevalence and Perinatal Prognosis
2Secondary Hospital, Pediatric unit, CSREF kalabancoro Bamako, Mali
3Secondary Hospital, Pediatric unit, CSREF Mopti, Mali
Received Date: Oct 23, 2023 / Accepted Date: Dec 23, 2023 / Published Date: Jan 24, 2024
Copyright: ©Fousseyni Traore, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Traore, F., Konate, D., Maiga, B., Sacko, K., Idriss, L., et al. (2024). Fetal Macrosomia at Gabriel Toure Hospital: Prevalence and Perinatal Prognosis. J Cli Ped Chi Res, 5(1), 01-05.
Abstract
Macrosomia is a concern in the daily practice of the neonatologist. The aim of this work was to investigate the sociodemographic, clinical and survival aspects of macrosomic neonates. It was a retrospective and descriptive study ran from 01/01/2017 to 31/12/2019. Were included, all macrosomic neonates hospitalized in neonatology service during the study period. Forty- six macrosomic newborns were included, accounting for a hospital frequency of 0.71%. The predominant maternal age group was 20-29 years. Pregnancy was monitored in 73.9% of cases. Gestational diabetes represented 30.4% of cases. Pregnancy term was not specified in 43.5% of cases, and was exceeded in 6.5%. The main complications recorded were a serosanguineous bump observed in 41.3% of cases, clavicle fracture in 10.9%, cephalohaematoma in 6.5%, humerus fracture and obstetric brachial plexus palsy in 2.2% each (Figure 1). Hypoglycemia was observed in 39.1% of patients, 13% of whom died. Newborns were hospitalized for perinatal anoxia in 52.2% of cases, followed by neonatal infection in 47.8% and respiratory distress in 41.3% (Figure 2). At least a quarter of newborns (26.1%) were resuscitated at birth. The average hospital stay was 5.39 ± 2.902 days, with extremes ranging from one to twelve days.
Keywords
Fetal Macrosomia, Complications, Neonate, Mali
Introduction
Macrosomia is a birth weight at term greater ≥ 4000 grams or > 90 percentile of the intrauterine growth curves [1]. Macrosomia is a concern in the daily practice of the neonatologist [2]. Numerous studies have shown that overweight newborns have a higher risk of birth complications and long-term negative health problems, such as diabetes and obesity [3,4]. Excessive birth weight may be an important component in the developmental design of noninfectious diseases and may result in a more difficult start to life compared to appropriately weighted newborns [5,6]. The delivery of a macrosomic baby involves maternal and neonatal complications that are well known: shoulder dystocia with, brachial plexus palsy, asphyxia during expulsion, fractures (clavicles, humerus) during maneuvers. Hypoglycemia and hypocalcemia are among the most frequent complications in overweight newborns. On the maternal side, there is an increase in caesarean sections (before and during labour), immediate or remote genital tract injuries (tears) or fistulas during vaginal deliveries, postpartum haemorrhage and infections [7,8]. The etiological factors of fetal macrosomia are numerous and often interrelated and their relative influence remains poorly understood [9].
In America, the rate of macrosomic babies varies from 1.7% to 7% in the USA [10]. In Europe, on the other hand, the frequency of macrosomia is almost homogeneous around 5% despite small variations in some countries: 4.5% in France and 4.7% in Italy [11]. In Africa, although this prevalence varies with the socio-economic level and other definition criteria according to each country [12-14]. In Mali, we have not recent data on this subject. In this study, we will study the sociodemographic, clinical and evolutionary aspects of macrosomic newborns in the neonatology department of the CHU-Gabriel Toure.
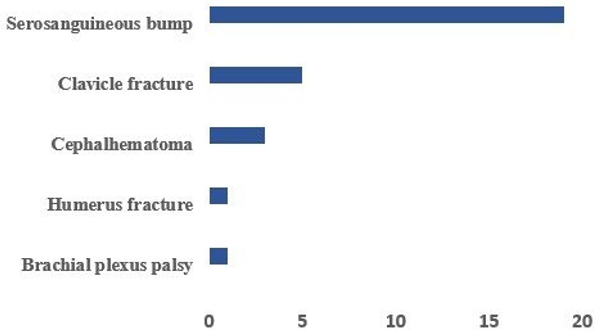
Figure 1: Distribution According to Perinatal Complications

Figure 2: Main Reasons of Hospitalization
Patients and Methods
This retrospective, descriptive study ran from 01/01/2017 to 31/12/2019. The aim of this work was to investigate the sociodemographic, clinical and survival aspects of macrosomic neonates in our neonatology service. Were included, all macrosomic neonates hospitalized in neonatology during the study period. Newborns who did not comply with the criteria for inclusion or whose records could not be used were not included. Data were collected from the neonatal medical record, the pregnancy follow-up booklet, the transfer form, and from the mother and/or accompanying persons. Data entry and analysis were performed using SPSS version 20 SPSS software.
Results
Forty-six macrosomic newborns were included, accounting for a hospital frequency of 0.71%. The predominant maternal age group was 20-29 years. Two percent of the mothers were under 20 years old. Pregnancy was monitored in 73.9% of cases. Gestational diabetes was found in 30.4% of cases. Regarding parity: 45.7% were pauciparous, 17.4% primiparous, 21.7% multiparous and 15.2% highly multiparous. A history of macrosomic neonates was found in 13% of mothers. Pregnancy term was not specified in 43.5% of cases, and was exceeded in 6.5%. The characteristics of the newborns were as follows: The sex ratio was 1.8; 34.8% had a weight ≥4500 grams and 65.2% weighed less than 4500 grams, 6.5% had a height <50 cm and 93.6% had a height ≥ 50 cm, as for the head circumference, it was ≤35 cm in 95.7% of cases and >35cm in 4.3% of cases (Table). Delivery occurred in a referral health center in 47.8% of cases.
|
Parameters |
Number |
Percentage |
|
Weight (g) |
|
|
|
< 4 500 |
30 |
65,2 |
|
≥ 4 500 |
16 |
34,8 |
|
Size (cm) |
|
|
|
< 50 |
3 |
6,5 |
|
≥ 50 |
43 |
93,5 |
|
Head Circumference (cm) |
|
|
|
30 – 39 |
44 |
95,7 |
|
> 39 |
2 |
4,3 |
Table: Patients Distribution According to Weight, Head Circumference and Height
Delivery in a university hospital accounted for 34.8% of cases. Caesarean section (39.1%) and vaginal delivery in 60.9% of cases. The use of instruments (vacuum aspiration or forceps) was reported in 17.4% of cases. The treatments received by the newborns were as follows: infusion of 10% glucose serum and calcium in 97.8% of cases, antibiotics in 70% of cases and oxygen therapy in 21.4% of cases. The main complications recorded were a serosanguineous bump observed in 41.3% of cases, clavicle fracture in 10.9%, cephalohaematoma in 6.5%, humerus fracture and obstetric brachial plexus palsy in 2.2% each (Figure 1). Hypoglycemia was observed in 39.1% of patients, 13% of whom died. Newborns were hospitalized for perinatal anoxia in 52.2% of cases, followed by neonatal infection in 47.8% and respiratory distress in 41.3% (Figure 2). At least a quarter of newborns (26.1%) were resuscitated at birth. The average hospital stay was 5.39 ± 2.902 days, with extremes ranging from 1 to 12 days. The large majority of children (80.4%) had a normal clinical examination, but 4.3% were discharged against medical advice and 13% died.
Discussion
Our study reveals a frequency of 0.71%, this frequency is lower than that found in various African studies: 6.87% in Morocco, 5.7% in DRC and 10.9% in Tunisia [15-17]. In a review of the American literature on macrosomia, Chauhan found that this frequency varied around 10% between 1996 and 2002 [18]. A Chinese study records a frequency of 3.4% [19]. The incidence of macrosomia is differently reported according to racial differences, ethnic differences and the presence of local factors in different regions [20]. According to Cheng, the difference in birth weight distribution is probably due to genetic differences and anthropometric abnormalities between populations [8]. The low rates in the African studies could be explained by their monocentric nature. But in addition, factors such as malnutrition, poor follow¬up, lack of hygiene during pregnancy, and low socioeconomic status may explain these low rates. Half of the parturient (50%) were aged 30 years or older: this rate is lower than that of Azzam Imane in Morocco where 57.63% of the mothers were aged 30 years or older [8] but higher than that of Laghzaoui where the majority of parturient were aged 30 years or younger [21]. This can be explained by the socio-cultural specificity of each country (age of marriage, lifestyle, family planning etc.). According to the American College of Obstetricians and Gynaecologists (ACOG), the history of macrosomia is the most incriminating factor in the occurrence of macrosomia, its positive predictive value is 95% and it is practically the same value found by the National Agency for the Development of Medical Evaluation (ANDEM) [22]. In our study 13% of the mothers had a history of fetal macrosomia. This rate is higher than that of Elouazzani in Morocco who found 4% in his study [14].
Most works have also reported the preponderance and multiparity, this is consistent with the data from our series where multiparous women represented 36.9% [23]. According to several authors, diabetes, whether gestational or pre-existing to pregnancy, is a known risk factor for fetal macrosomia: its frequency varies between 45% in a population of diabetic women, and 8% in a control population of non-diabetic women [24,25]. In our series, 30.4% of mothers had gestational diabetes. The ethiopathogenic mechanism of macrosomia is classically attributed to fetal hyperinsulinism in response to maternal hyperglycemia, due to the anabolic effect of insulin [26,27]. This is true in diabetic parturient in whom it has been shown that strict control of maternal blood glucose levels significantly reduces the risk of fetal macrosomia [26,28,29].
Our results showed a significantly high rate of caesarean section in parturient with 39.1%. Our rate is higher than that of Prosper et al with 9.8% but comparable to the data in the literature which show that macrosomia is associated with a high risk of caesarean section and higher rates than ours have been reported in the literature ranging from 21.4% to 51.4% [16,30-32]. Whereas several studies have shown that vaginal delivery is a more reasonable alternative to elective cesarean section. The American College of Obstetrics and Gynecology has suggested prophylactic cesarean delivery for any suspected macrosomia with fetal weight ≥ 5000g in non-diabetic women and at ≥ 4500g in case of diabetes [33]. Male gender was cited by several studies as a risk factor for macrosomia [34]. Thus, both univariate and multivariate studies have shown that male sex is a predictor of macrosomia. The sex ratio was 1.8 in our series. Our rate is comparable to that of Fatnassi et al [17]. Hypoglycemia is a dreaded complication because it could be responsible for neonatal death. We found 39.1% of cases of hypoglycemia.
This high rate can be explained by the fact that more than 50% of the deliveries took place outside the university hospital; these children at the time of referral are not necessarily fed and can therefore easily suffer from hypoglycemia. Neonatal morbidity related to the delivery of a macrosomia is not negligible. It is dominated by two complications, namely serosanguineous bumps, which are generally trivial, and lesions of the brachial plexus [27]. The latter are formidable and frequent in our series. They reflect the existence of a fetopelvic disproportion. A serosanguineous bump was found in 41.3% of newborns and a cephalohaematoma in 6.5% of cases. A fracture of the clavicle was found in 10.9% of the newborns in our series. Clavicle fracture was more frequent in the macrosomic group than in the control group in the series by Fatnassi et al [17]. The death rate was up to 13% in our study, it is higher than that of Fatnassi et al (4.8%) but can be explained by the high rate of hypoglycemia and also the excessive weights where we have 34.8% with a weight greater than 4500g. Data from the literature support that maternal and neonatal morbidity increases with birth weight and especially in newborns weighing more than 4500 g [35,36].
Conclusion
Macrosomia is often the cause of maternal and perinatal complications. The reduction of these complications requires a better knowledge of the risk factors and an early detection. More effective monitoring of pregnancy and the equipment of maternity wards will reduce morbidity and mortality.
Ethical Considerations
Upon admission, parents or legal guardians of patients approved their inclusion in a clinical research study. The national ethics committee validated the research protocol.
References
- Bouabida D, Belaoun F, Maarouf A, Bouchareb N, Saadalah F, Benbouabdelah M. Epidemiological profile of macrosomic newborns at Nouar FADELA EHS: preliminary results, Archives of Pediatrics 2015; 22 (HS2): 233-371.
- Chubb Cw, Alarge Child, Brmed J, 1879, 1,143.
- Cascella, M., Rajnik, M., Cuomo, A., Dulebohn, S. C., & Di Napoli, R. S. StatPearls Publishing; Treasure Island, FL, USA: 2020. Features, evaluation and treatment coronavirus (COVID-19) [Google Scholar].
- Beta, J., Khan, N., Khalil, A., Fiolna, M., Ramadan, G., & Akolekar, R. (2019). Maternal and neonatal complications of fetal macrosomia: systematic review and meta-analysis. Ultrasound in Obstetrics & Gynecology, 54(3), 308-318.
- Fang, F., Zhang, Q. Y., Zhang, J., Lei, X. P., Luo, Z. C., & Cheng, H. D. (2019). Risk factors for recurrent macrosomia and child outcomes. World Journal of Pediatrics, 15, 289-296.
- Hofstee, P., McKeating, D. R., Bartho, L. A., Anderson, S.T., Perkins, A. V., & Cuffe, J. S. (2020). Maternal selenium deficiency in mice alters offspring glucose metabolism and thyroid status in a sexually dimorphic manner. Nutrients, 12(1), 267.
- Goffinet, F. (2000). Difficulties in antenatal recognition of fetal macrosomia. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction, 29(1 Suppl), 13-19.
- Cheng, Y. K. Y., & Lao, T. T. (2014). Fetal and maternal complications in macrosomic pregnancies. Research and Reports in Neonatology, 65-70.
- Lepercq, J., Timsit, J., & Hauguel-de Mouzon, S. (2000). Etiopathogeny of fetal macrosomia. Journal de gynecologie, obstetrique et biologie de la reproduction, 29(1 Suppl), 6-12.
- Martin, J. A., Hamilton, B. E., Osterman, M. J., Driscoll, A. K., & Mathews, T. J. (2017). Births: final data for 2015.
- Mello, G., Parretti, E., Mecacci, F., Lucchetti, R., Lagazio, C., Pratesi, M., & Scarselli, G. (1997). Risk factors for fetal macrosomia: the importance of a positive oral glucose challenge test. European Journal of Endocrinology, 137(1), 27-33.
- Mai, A. H., & Abbassia, D. (2014). The prevalence of fetal macrosomia at the specialized hospital of gynecology and obstetrics of Sidi Bel Abbes (West of Algeria). Journal of Nutrition & Food Sciences, 4(3), 272.
- Denguezli, W., Faleh, R., Fessi, A., Yassine, A., Hajjaji, A., Laajili, H., & Sakouhi, M. (2009). Risk factors of fetal macrosomia: role of maternal nutrition. La Tunisie Médicale, 87(9), 564-568.
- Touhami Elouazzania, F., Kabiri, M., Karboubia, L., Keswatib, J., Mrabet, M., & Barkat, A. (2012. Macrosomia: About 255 Cases. Journal of Pediatrics and Childcare, 25, 97-101.
- Fetal macrosomia about 1270 cases in the Faculty of Medicine and Pharmacy of Rabat. Thesis of med. Rabat, 2015, n°266.
- Luhete, P. K., Mukuku, O., Kiopin, P. M., Tambwe, A. M., & Kayamb, P. K. M. (2016). Macrosomie fœtale à Lubumbashi: facteurs de risque et pronostic maternel et périnatal. Pan African Medical Journal, 23(1).
- Fatnassi, R., Ragmoun, H., Marzougui, L., Mkhinini, I., & Hammami, S. (2017). Facteurs de risque et pronostic materno-fœtal de la macrosomie fœtale: étude comparative a propos de 820 cas Risk factors and materno-fetal prognosis of foetal macrosomia: comparative study of 820 cases. The Pan African Medical Journal, 28.
- Chauhan, S. P., Grobman, W. A., Gherman, R. A., Chauhan,V. B., Chang, G., Magann, E. F., & Hendrix, N. W. (2005). Suspicion and treatment of the macrosomic fetus: a review. American journal of obstetrics and gynecology, 193(2), 332-346.
- Cheng, Y. K. Y., Lao, T. T., Sahota, D. S., Leung, V. K. T., & Leung, T. Y. (2013). Use of birth weight threshold for macrosomia to identify fetuses at risk of shoulder dystocia among Chinese populations. International Journal of Gynecology & Obstetrics, 120(3), 249-253.
- Henriksen, T. (2008). The macrosomic fetus: a challenge in current obstetrics. Acta obstetricia et gynecologica Scandinavica, 87(2), 134-145.
- M Laghzaoui, B. (2004). Epidemiolpgie de la macrosomie, 99-102.
- Gyurkovits, Z., Kálló, K., Bakki, J., Katona, M., Bitó, T., Pál, A., & Orvos, H. (2011). Neonatal outcome of macrosomic infants: an analysis of a two-year period. European Journal of Obstetrics & Gynecology and Reproductive Biology, 159(2), 289-292.
- Kamanu, C. I., Onwere, S., Chigbu, B., Aluka, C., Okoro, O., & Obasi, M. (2009). Fetal macrosomia in African women: a study of 249 cases. Archives of gynecology and obstetrics, 279, 857-861.
- Carlotti, N., Moquet, P. Y., Foucher, F., & Laurent, M. C. (2000). Le diabète gestationnel: prise en charge conjointe obstétricale et endocrinienne. J. Gynécol. Obstet. Biol Reprod, 29(4), 403-405.
- Ballard, J. L., Rosenn, B., Khoury, J. C., & Miodovnik,M. (1993). Diabetic fetal macrosomia: significance of disproportionate growth. The Journal of pediatrics, 122(1), 115-119.
- Das, S., Irigoyen, M., Salvador, A., Patterson, M. B., & Schutzman, D. L. (2009). Neonatal outcomes of macrosomic births in diabetic and non-diabetic women. Archives of Disease in Childhood-Fetal and Neonatal Edition. 94, 419-422.
- Saleh, A. M., Al-Sultan, S. M., Moria, A. M., Rakaf, F. I., Turkistani, Y. M., & Al-Onazi, S. H. (2008). Fetal macrosomia greater than or equal to 4000 grams. Saudi Med J, 29(10), 1463-1469.
- Ehrenberg, H. M., Mercer, B. M., & Catalano, P. M. (2004). The influence of obesity and diabetes on the prevalence of macrosomia. American journal of obstetrics and gynecology, 191(3), 964-968.
- Yogev, Y., & Catalano, P. M. (2009). Pregnancy and obesity.Obstetrics and Gynecology Clinics, 36(2), 285-300.
- Ezegwui, H. U., Ikeako, L. C., & Egbuji, C. (2011). Fetal macrosomia: obstetric outcome of 311 cases in UNTH, Enugu, Nigeria. Nigerian journal of clinical practice, 14(3), 322-326.
- Alberico, S., Montico, M., Barresi, V., Monasta, L., Businelli, C., Soini, V., ... & Multicentre Study Group on Mode of Delivery in Friuli Venezia Giulia. (2014). The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: results from a prospective multicentre study. BMC pregnancy and childbirth, 14, 1-8.
- Palumbo, M. A., Fauzia, M., Gulino, F. A., Di Grazia, F. M., Giunta, M. R., Giannone, T. T., ... & Zarbo, G. (2013). Macrosomia: effect, predictive maternal factor, neonatal complications. Our casuistry. Giornale italiano di ostetricia e ginecologia, 35(3), 453-456.
- Zelop, C. M., Shipp, T. D., Repke, J. T., Cohen, A., & Lieberman, E. (2001). Outcomes of trial of labor following previous cesarean delivery among women with fetuses weighing> 4000 g. American journal of obstetrics and gynecology, 185(4), 903-905.
- Depaillerets F. Delivery of the big baby. Thesis of medicine. Paris France 1992.
- Oral, E., Cagdas, A., Gezer, A., Kaleli, S., Aydinli, K., & Öçer, F. (2001). Perinatal and maternal outcomes of fetal macrosomia. European Journal of Obstetrics & Gynecology and Reproductive Biology, 99(2), 167-171.
- Kamanu, C. I., Onwere, S., Chigbu, B., Aluka, C., Okoro, O., & Obasi, M. (2009). Fetal macrosomia in African women: a study of 249 cases. Archives of gynecology and obstetrics, 279, 857-861.