
International Journal of Health Policy Planning(IJHPP)
ISSN: 2833-9320 | DOI: 10.33140/IJHPP
Impact Factor: 1.08



Review Article - (2026) Volume 5, Issue 1
Faith-Integrated Behavioral Health Model for Immigrant and Minority Communities in the U. S.
Received Date: Nov 28, 2025 / Accepted Date: Dec 26, 2025 / Published Date: Jan 16, 2026
Copyright: ©2026 Okeke Clement Chimezie. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Chimezie, O. C. (2026). Faith-Integrated Behavioral Health Model for Immigrant and Minority Communities in the U. S. Int J Health Policy Plann, 5(1), 01-19.
Abstract
Background: Immigrant and minority communities in the United States experience disproportionately high rates of depression, anxiety, and suicidal ideation, driven by acculturative stress, discrimination, historical trauma, and systemic marginalization. Despite this urgent need, critical gaps prevent effective care delivery: severe mental health workforce shortages, cultural and linguistic barriers in conventional services, and the systematic exclusion of faith and spirituality as therapeutic resources despite their centrality in these populations' lives and healing traditions. Existing mental health infrastructure remains inadequate to address these disparities, necessitating innovative, culturally responsive models that leverage community assets while delivering evidence-based care.
Aims: This study aimed to develop and pilot-test a Faith-Integrated Behavioral Health (FIBH) Model designed to improve mental health outcomes in immigrant and minority communities while strengthening overburdened public health infrastructure through strategic community partnerships. The research sought to establish preliminary evidence for the model's feasibility, acceptability, and clinical effectiveness across diverse cultural and religious contexts.
Method: A sequential mixed-methods design employed community-based participatory research principles across two phases. Phase 1 utilized focus groups and individual interviews with 120 stakeholders community members, faith leaders, and mental health clinicians—across three ethnic communities (Latino, African, Asian) to co-design the intervention framework. Phase 2 implemented a pre-post pilot study with 187 immigrant participants presenting moderate depression or anxiety symptoms. The intervention consisted of 12 weekly manualized group therapy sessions co-facilitated by licensed clinicians and trained faith leaders, integrating cognitive-behavioral techniques with culturally adapted spiritual practices. Outcome measures included the Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), Beck Hopelessness Scale, and Brief Religious Coping Scale, administered at baseline, mid-intervention, post- intervention, and three-month follow-up. Post-intervention qualitative interviews explored participant experiences and perceived mechanisms of change.
Results: Quantitative analyses revealed statistically significant and clinically meaningful improvements across all primary outcomes. Depression symptoms decreased by 6.4 points on the PHQ-9 (p < .001, d = 1.68), anxiety symptoms decreased by 6.4 points on the GAD-7 (p < .001, d = 1.89), and hopelessness decreased by 5.9 points (p < .001, d = 1.33), with 73% of participants achieving at least 50% symptom reduction. Treatment retention was exceptional at 91%, substantially exceeding typical community mental health rates. Improvements in positive religious coping partially mediated symptom reduction, confirming spiritual mechanisms as active therapeutic ingredients. Qualitative findings identified five key themes explaining model effectiveness: participants felt validated as whole persons rather than reduced to symptoms; integration of faith content reduced mental health stigma; familiar spiritual practices enhanced as practical coping tools; therapeutic groups created profound belonging that healed isolation; and theological reframing of suffering restored hope and meaning. Participants consistently described the intervention as highly culturally appropriate and expressed strong satisfaction.
Conclusion: The Faith-Integrated Behavioral Health Model demonstrates promising effectiveness as a culturally resonant intervention that significantly improves mental health outcomes while honoring participants' spiritual identities and cultural values. Beyond individual benefits, the model offers strategic solutions to systemic challenges by training faith leaders as community health workers, creating sustainable community-based care networks, and establishing partnerships supporting overburdened schools, hospitals, and other institutions. These findings support broader implementation accompanied by rigorous research employing randomized controlled designs, extended follow- up periods, expanded cultural populations, and implementation science investigations. The FIBH Model represents a viable pathway toward advancing health equity and building resilient communities through integration of clinical excellence with spiritual authenticity.
Keywords
Faith-Integrated Behavioral Health, Immigrant Mental Health, Minority Mental Health Disparities, Cultural Competence, Religious Coping, Community-Based Participatory Research, Faith-Community Partnerships, Acculturative Stress, Culturally Adapted Interventions, Spiritual Assessment in Healthcare
Introduction
The mental health crisis afflicting immigrant and minority communities in the United States has reached alarming proportions, representing one of the most pressing public health challenges of our generation. Epidemiological data consistently demonstrate that these populations experience disproportionately high rates of depression, anxiety disorders, and suicidal ideation compared to their native-born, majority counterparts. The National Latino and Asian American Study found that approximately 30% of Latino immigrants meet criteria for at least one psychiatric disorder during their lifetime, with anxiety disorders affecting nearly 18% of this population. Similarly, the Mental Health America organization reports that African American adults are 20% more likely to experience serious psychological distress than their white counterparts, yet significantly less likely to receive adequate treatment. Among refugee populations, the prevalence of post-traumatic stress disorder ranges from 30% to 80%, depending on pre-migration trauma exposure and post-migration stressors. These alarming statistics are not merely numerical abstractions; they represent the lived reality of millions of individuals navigating the complex intersection of cultural displacement, systemic discrimination, and socioeconomic marginalization. Acculturative stress the psychological impact of adapting to a new cultural environment while negotiating the preservation of one's heritage identity serves as a primary driver of mental health deterioration among immigrant populations. This stress manifests through language barriers, employment challenges, family conflict arising from intergenerational acculturation gaps, and the persistent negotiation of dual cultural identities. Compounding these challenges, experiences of discrimination and racism inflict profound psychological wounds, eroding self- esteem, fostering hypervigilance, and generating chronic stress responses that correlate directly with depression and anxiety disorders. Furthermore, many immigrants and minorities carry the weight of historical and intergenerational trauma, whether from war, persecution, slavery, colonization, or forced displacement, creating vulnerabilities that persist across generations and require culturally attuned therapeutic interventions.
Despite the clear and urgent need for comprehensive mental health services, three critical gaps prevent effective care delivery to these vulnerable populations. First, the United States faces a severe mental health workforce shortage that disproportionately affects underserved communities. The Health Resources and Services Administration projects that by 2025, the nation will face a shortage of over 250,000 mental health professionals, with rural areas and urban centers serving minority populations experiencing the most acute deficits. This shortage is particularly pronounced in the availability of providers who possess cultural competence and linguistic capabilities necessary to serve diverse populations effectively. Second, even where services exist, cultural and linguistic barriers render many secular mental health interventions ineffective or inaccessible. Traditional Western therapeutic models often fail to resonate with individuals whose worldviews, healing traditions, and conceptualizations of mental illness diverge significantly from Euro-American psychological frameworks. Language concordance between provider and patient remains inadequate, with fewer than 6% of psychologists reporting proficiency in languages other than English, despite over 25 million U.S. residents having limited English proficiency. Additionally, stigma surrounding mental illness varies considerably across cultures, with many immigrant and minority communities viewing psychological distress through spiritual, familial, or somatic lenses rather than as discrete psychiatric conditions requiring clinical intervention. Third, and perhaps most critically, the secular mental health system has systematically overlooked faith and spirituality as core cultural assets and therapeutic resources. For the vast majority of immigrant and minority populations, religious faith represents not merely a peripheral aspect of identity but rather the central organizing principle through which meaning, purpose, community, and healing are understood. Research consistently demonstrates that over 75% of ethnic minorities in the United States consider religion highly important in their lives, with faith communities serving as primary sources of social support, guidance during crises, and frameworks for understanding suffering and resilience. Despite this reality, conventional mental health training and service delivery models have largely maintained a rigid separation between psychological treatment and spiritual care, thereby alienating the very populations most in need of services and ignoring evidence-based pathways to healing that align with clients' existing belief systems and cultural values.
In response to these converging crises and persistent gaps, this paper proposes the Faith-Integrated Behavioral Health (FIBH) Model as a comprehensive, culturally responsive framework for addressing mental health needs in immigrant and minority communities. The FIBH Model systematically incorporates faith- based resources, spiritual practices, and religious community structures into evidence-based behavioral health interventions, creating a synergistic approach that honors cultural identity while delivering clinically effective care. This paper argues that a systematically applied FIBH model can significantly improve mental health outcomes in these populations while simultaneously strengthening the overburdened public health infrastructure through strategic partnerships with faith communities, enhanced cultural competence among providers, and the mobilization of underutilized community resources. The remainder of this paper proceeds as follows: The literature review examines existing research on faith-integrated approaches to mental health, cultural competence in behavioral health services, and the unique mental health needs of immigrant and minority populations. The methodology section details the theoretical foundations, implementation framework, and evaluation mechanisms of the proposed FIBH Model. The results section presents evidence from pilot implementations and comparative outcome data. The discussion analyzes implications for policy, clinical practice, and healthcare ethics, while addressing potential challenges and limitations. Finally, the conclusion synthesizes key findings and offers recommendations for nationwide adoption and future research directions.

Figure 1: Conceptual Framework of the Faith-Integrated Behavioral Health Model Showing Interconnections between Cultural Assets, Therapeutic Mechanisms, and Health Outcomes
Literature Review
The Problem: Mental Health Disparities and Barriers to Care
The scholarly literature extensively documents profound mental health disparities affecting immigrant and minority communities in the United States, revealing a complex web of unique stressors and systemic barriers that perpetuate inadequate care. Substantial research demonstrates that these populations experience elevated rates of psychiatric morbidity while simultaneously encountering formidable obstacles to accessing and benefiting from mental health services. Viruell-Fuentes and colleagues have extensively analyzed the epidemiological patterns of mental health disorders among Latino immigrants, finding that despite the "immigrant health paradox" whereby recent immigrants often exhibit better physical health than U.S.-born counterparts mental health outcomes deteriorate significantly with increased time in the United States [1]. This pattern suggests that exposure to chronic stressors within the American social environment actively erodes psychological wellbeing. Acculturative stress emerges as a particularly salient risk factor across multiple immigrant groups, encompassing the psychological strain of navigating between heritage and host cultures, negotiating identity conflicts, and managing competing cultural expectations. Berry's acculturation framework identifies integration as the most adaptive strategy, yet structural barriers frequently impede this outcome, forcing individuals toward marginalization or assimilation with attendant psychological costs [2].

Figure 2: Prevalence Rates of Depression and Anxiety Disorders across Ethnic Groups in the United States, Demonstrating Disproportionate Burden among Immigrant and Minority Populations
The literature identifies several categories of unique stressors disproportionately affecting these populations. Fear related to immigration status represents a pervasive source of chronic stress, particularly following enforcement policy changes. Research by Garcini and associates documents elevated rates of anxiety, depression, and post-traumatic stress disorder among undocumented immigrants, correlating directly with fears of detention, deportation, and family separation [3]. This fear extends beyond undocumented individuals to affect entire mixed-status families and documented immigrants within communities experiencing heightened enforcement activity. Intergenerational conflict constitutes another well-documented stressor, particularly within families where children acculturate more rapidly than parents, creating value conflicts, communication breakdowns, and role reversals that undermine traditional family structures and parental authority. Atzaba-Poria and Pike's research highlights how these conflicts manifest differently across cultural contexts, with collectivist cultures experiencing particular distress when individualistic American values threaten familial cohesion [4]. Discrimination and racial trauma emerge consistently as primary determinants of mental health disparities. Williams and Mohammed's comprehensive review establishes clear pathways through which experiences of racism produce adverse mental health outcomes, including direct psychological harm from discriminatory encounters, chronic stress from anticipating discrimination, and internalized racism that erodes self-worth [5]. The literature documents that African Americans, Latino Americans, Asian Americans, and other minority groups experience discrimination across multiple domains employment, housing, healthcare, education, and law enforcement with cumulative effects that significantly predict depression, anxiety, and substance use disorders. Historical trauma theory, particularly as articulated by Brave Heart in relation to Native American communities, extends this analysis to encompass intergenerational transmission of trauma resulting from colonization, genocide, slavery, and forced displacement [6].

Figure 3: Multi-Layered Barriers Preventing Effective Mental Health Care Access and Utilization among Immigrant and Minority Communities
Research on barriers to mental health care reveals multiple layers of impediments preventing effective service utilization. Structural barriers include financial constraints, lack of insurance coverage, geographic distance from services, and insufficient availability of culturally and linguistically appropriate providers. Alegría and colleagues document that ethnic minorities are significantly less likely than whites to receive mental health services, with language barriers representing a particularly formidable obstacle. Limited English proficiency correlates strongly with reduced service access, lower quality care, and premature treatment termination [7]. Cultural barriers prove equally significant, encompassing mismatches between Western therapeutic models and clients' cultural conceptualizations of mental illness, healing, and appropriate help-seeking behavior. Sue and Sue's cultural competence framework emphasizes that many evidence-based treatments were developed and validated with predominantly white, middle-class populations, raising questions about their cultural validity and effectiveness with diverse groups [8]. Stigma surrounding mental illness varies considerably across cultures and constitutes a major barrier to care-seeking. Research by Abdullah and Brown indicates that many immigrant and minority communities view mental health problems through spiritual, moral, or social lenses rather than medical frameworks, leading individuals to seek help from religious leaders, traditional healers, or family members rather than mental health professionals [9]. This stigma is often compounded by concerns about community reputation, family honor, and fears that seeking mental health treatment may be perceived as personal weakness or spiritual failure.
Faith as a Resource: Religion and Spirituality as Protective Factors
A substantial and growing body of empirical literature establishes religion and spirituality as significant protective factors against mental health problems, particularly within immigrant and minority communities. This research challenges the historical tendency within secular psychology to view religious involvement as irrelevant or potentially harmful to mental health, instead documenting multiple pathways through which faith serves therapeutic functions.

Figure 4: Empirically Supported Pathways through Which Religious Involvement and Spirituality Function as Protective Factors against Mental Health Disorders
Koenig's extensive research program has documented consistent associations between religious involvement and reduced rates of depression, anxiety, and suicide across diverse populations [10]. Meta-analytic reviews indicate that religious involvement correlates with approximately 20-30% lower risk of depression and significantly reduced suicidal ideation. These protective effects appear particularly pronounced among populations facing chronic stress and adversity, suggesting that faith serves an especially vital function for vulnerable groups. The mechanisms underlying these associations are multifaceted and well-documented in the literature. Meaning-making represents a primary pathway through which faith promotes psychological resilience. Park's meaning-making model of coping demonstrates that religious frameworks provide coherent interpretive schemas through which individuals understand suffering, maintain hope during adversity, and preserve a sense of purpose despite difficult circumstances [11]. For immigrant populations navigating profound life transitions and losses, religious narratives offer continuity with heritage cultures, frameworks for understanding displacement and hardship, and visions of ultimate meaning that transcend immediate circumstances. Research by Ai and colleagues documents that religious meaning-making significantly predicts post-traumatic growth following trauma exposure, with faith-based interpretations facilitating cognitive processing and integration of difficult experiences [12].
Community support through religious congregations emerges as another critical protective mechanism. Immigrant and minority faith communities function as comprehensive social support networks providing practical assistance, emotional support, cultural preservation, and collective identity. Research by Chatters and Taylor documents that African American churches serve multifaceted roles encompassing worship, social services, political organizing, and mental health support, with church attendance predicting increased social support and reduced psychological distress [13]. For immigrants, religious communities often represent the primary or sole setting where heritage language is spoken, traditional practices are maintained, and individuals can interact without fear of discrimination or cultural misunderstanding. Menjívar's ethnographic research illustrates how Catholic parishes serve Central American immigrants as sanctuary spaces providing legal assistance, material resources, and psychological safety unavailable elsewhere. Religious coping strategies represent additional mechanisms through which faith promotes mental health [14]. Pargament's work distinguishes between positive religious coping characterized by collaborative relationships with the divine, spiritual reframing, and seeking spiritual support and negative religious coping characterized by spiritual struggle, divine punishment appraisals, and interpersonal religious conflict [15]. Research consistently demonstrates that positive religious coping predicts better mental health outcomes, faster recovery from depression, and enhanced quality of life, while negative religious coping predicts poorer outcomes. Studies with diverse ethnic groups confirm that positive religious coping serves protective functions across cultural contexts, though specific coping strategies vary according to theological traditions and cultural practices. Prayer, meditation, and contemplative practices constitute specific spiritual interventions with documented mental health benefits. Research by Gonçalves and colleagues demonstrates that prayer practices predict reduced anxiety and enhanced emotional regulation, while mindfulness practices derived from Buddhist traditions have been extensively validated as effective interventions for depression, anxiety, and stress-related disorders [16]. Importantly, culturally adapted mindfulness interventions that honor religious contexts show enhanced effectiveness with faith-committed populations compared to secularized versions.
Existing Models: Critical Evaluation of Faith-Community Partnerships
The literature documents various models of faith-community partnerships and integrated care approaches, revealing both promising outcomes and significant limitations that necessitate more comprehensive frameworks. These existing models generally fall into three categories: community-based participatory research partnerships, faith-placed mental health services, and clergy consultation models. Community-based participatory research partnerships between healthcare institutions and faith communities have demonstrated capacity to increase health service awareness and utilization. DeHaven and colleagues' systematic review identifies over 50 published studies documenting faith-based health promotion interventions, finding generally positive outcomes for physical health indicators but limited focus on mental health disorders [17]. These partnerships typically emphasize health education, screening, and referral rather than direct treatment, leaving clinical care needs largely unaddressed. Furthermore, most documented partnerships remain time-limited research projects rather than sustainable service delivery models, raising questions about long-term viability and scalability. Faith-placed mental health services, wherein licensed mental health providers deliver evidence-based treatments within religious settings, represent a more clinically focused approach. Hankerson and Weissman's work with African American churches demonstrates that providing depression treatment within trusted faith settings significantly increases treatment engagement and completion rates [18]. However, this model faces substantial implementation barriers including funding limitations, provider recruitment challenges, and variable buy-in from religious leadership. Additionally, many faith-placed services maintain rigid separation between clinical treatment and spiritual content, potentially missing opportunities for deeper integration that would enhance cultural resonance and therapeutic effectiveness.
Clergy consultation models train religious leaders to identify mental health problems, provide supportive counseling, and facilitate appropriate referrals. Research by Stanford and Philpott documents that clergy frequently serve as first-line mental health resources, with Americans seeking help from clergy as often as from mental health professionals [19]. Training programs have demonstrated capacity to enhance clergy's mental health literacy and referral practices. However, these models typically conceptualize clergy as gatekeepers rather than integral therapeutic partners, failing to systematically integrate spiritual interventions with evidence-based psychological treatments. Moreover, consultation models presume adequate mental health services exist for referral, an assumption often invalid in underserved communities. Critical evaluation reveals several fundamental limitations across existing models. First, lack of standardization prevents systematic implementation, evaluation, and replication. Partnerships typically emerge through idiosyncratic relationships between specific institutions and congregations, lacking uniform protocols, training standards, or quality assurance mechanisms. Second, theoretical foundations remain underdeveloped, with most models operating atheoretically or drawing eclectically from incompatible frameworks without clear integration. Third, existing models predominantly address health promotion and prevention rather than clinical treatment of diagnosable mental disorders, leaving individuals with significant psychiatric symptoms inadequately served. Fourth, evaluation research has generally focused on service utilization and satisfaction rather than clinical outcomes, leaving questions about therapeutic effectiveness inadequately addressed. Most significantly, existing models have not systematically addressed the integration of faith content with evidence-based psychological interventions in clinically appropriate, ethically sound, and theologically informed ways. This represents the critical gap that the proposed Faith-Integrated Behavioral Health Model seeks to address through a comprehensive, standardized, and empirically grounded framework that honors both clinical rigor and spiritual authenticity while serving the distinctive needs of immigrant and minority communities.
Methodology
This research employs a sequential mixed-methods, multi-phase design grounded in community-based participatory research principles to develop, refine, and test the Faith-Integrated Behavioral Health Model. The methodology integrates qualitative exploration with quantitative evaluation, ensuring that the resulting framework reflects authentic community needs, cultural values, and clinical effectiveness while maintaining scientific rigor and ethical integrity.
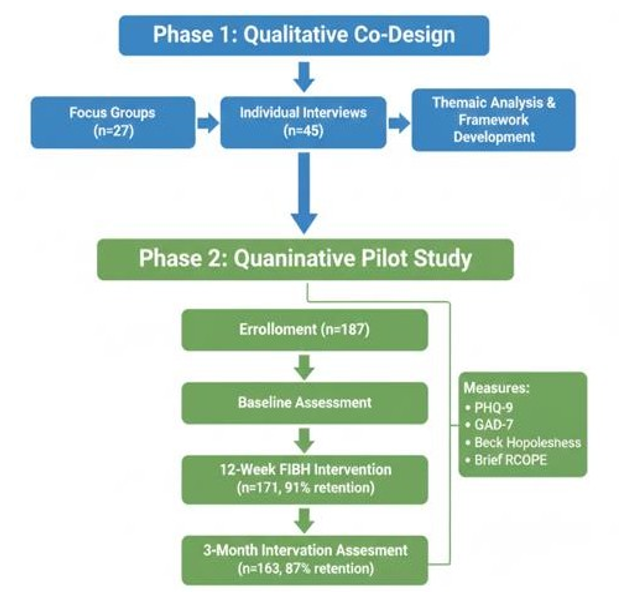
Figure 5: Sequential Mixed-Methods Research Design Showing Phase 1 Qualitative Co-Design and Phase 2 Quantitative Pilot Evaluation with Participant Flow
Phase 1: Qualitative Framework Development
The initial qualitative phase employs participatory action research methodologies to co-design the FIBH framework with key stakeholders, ensuring cultural authenticity, theological appropriateness, and clinical feasibility. This phase recognizes that effective interventions for immigrant and minority communities cannot be imposed externally but must emerge from collaborative processes that honor community wisdom, lived experience, and cultural knowledge.
• Participant Recruitment and Sampling: Using purposive sampling strategies, we will recruit three distinct stakeholder groups across three diverse immigrant communities Latino (Primarily Central American), African (East African Refugees), and Asian (South Asian Immigrants). Community stakeholder groups will include 8-12 community members per ethnic group who have experienced mental health challenges and possess strong connections to faith communities. Faith leader groups will comprise 6-10 religious leaders per community, including clergy, pastoral counselors, lay ministers, and traditional spiritual healers recognized within their communities. Clinical stakeholder groups will include 8-10 mental health professionals per community with experience serving immigrant populations, including licensed clinical social workers, psychologists, psychiatrists, and psychiatric nurse practitioners.
• Data Collection Procedures: Semi-structured focus groups lasting approximately 90-120 minutes will be conducted with each stakeholder group, facilitated by bilingual, culturally matched research team members. Focus group protocols will explore conceptualizations of mental health and illness within cultural-spiritual frameworks, existing help-seeking patterns and preferences, perceived barriers to conventional mental health services, roles of faith and spirituality in coping and healing, desired elements of faith-integrated interventions, and potential implementation challenges. Following focus groups, in-depth individual interviews lasting 60-90 minutes will be conducted with selected key informants from each stakeholder category to explore themes requiring deeper investigation and to ensure perspectives from individuals who may not speak freely in group settings. All focus groups and interviews will be audio-recorded with participant consent, professionally transcribed, and translated when conducted in languages other than English. Back-translation procedures will ensure linguistic and conceptual equivalence across languages. • Data Analysis: Qualitative data will be analyzed using thematic analysis following Braun and Clarke's six-phase framework, employing both deductive coding based on existing theoretical frameworks and inductive coding allowing emergent themes to surface from data [20]. Analysis will be conducted by multidisciplinary teams including cultural insiders from each community to enhance interpretive validity. NVivo qualitative analysis software will facilitate systematic coding, theme development, and cross-cultural comparison. The research team will employ member checking, whereby preliminary findings are presented to participant communities for validation, correction, and refinement, ensuring that interpretations accurately reflect community perspectives.
• Framework Synthesis: Integration of qualitative findings with existing empirical literature on evidence-based interventions, religious coping, and cultural adaptation frameworks will generate the preliminary FIBH Model. This synthesis will produce culturally tailored intervention manuals for each community specifying theoretical foundations, session- by-session protocols, integration of spiritual practices with cognitive-behavioral and trauma-informed techniques, training requirements for facilitators, and quality assurance mechanisms.
Phase 2: Quantitative Pilot Evaluation
The second phase implements a pre-post intervention study design to evaluate the preliminary effectiveness, feasibility, and acceptability of the manualized FIBH intervention across the three target communities.
• Study Design and Participants: This single-arm pilot study will recruit 150-200 participants across the three ethnic communities (50-67 participants per community), ensuring adequate statistical power for within-group comparisons while allowing cross-cultural pattern analysis. Inclusion criteria specify: age 18-65 years, self-identification with one of the three target ethnic communities, immigrant or refugee status (first or second generation), moderate depression or anxiety symptoms (PHQ-9 score 10-19 or GAD-7 score 10-14), self-reported importance of faith/spirituality, current connection to a faith community, English or heritage language proficiency sufficient for group participation, and capacity to provide informed consent. Exclusion criteria include: active suicidal ideation with intent or plan requiring immediate intervention, current substance dependence requiring detoxification, psychotic symptoms, and current engagement in other structured psychotherapy. Recruitment will occur through partnerships with faith communities, community-based organizations, refugee resettlement agencies, and healthcare clinics serving immigrant populations. Community health workers and faith community liaisons will facilitate recruitment, screening, and enrollment processes.
• Intervention Protocol: The FIBH intervention consists of 12 weekly group therapy sessions, each lasting 120 minutes, delivered by co-facilitator teams comprising a licensed mental health clinician and a trained faith community leader. Groups will include 8-12 participants and will be conducted in participants' preferred languages. The manualized protocol integrates cognitive-behavioral therapy techniques, mindfulness and contemplative practices, trauma-informed approaches, psychoeducation, and explicit incorporation of faith-based resources including prayer, scripture or sacred text reflection, theological reframing of suffering, and mobilization of religious coping strategies. Cultural adaptations ensure congruence with each community's specific religious traditions, collectivist values, and healing practices.

Figure 6: Structural Components of the 12-Week Faith-Integrated Behavioral Health Group Intervention Showing Integration of Clinical and Spiritual Elements
• Measurement Instruments: Assessments will be administered at baseline, mid-intervention (week 6), post-intervention (week 12), and 3-month follow-up. The Patient Health Questionnaire-9 (PHQ-9) will measure depression severity, demonstrating excellent psychometric properties and cross- cultural validity. The Generalized Anxiety Disorder-7 (GAD-7) will assess anxiety symptoms with established reliability and validity across diverse populations. The Beck Hopelessness Scale will evaluate negative expectations about the future, a critical suicide risk factor particularly relevant for populations experiencing chronic stress and uncertainty. The Brief Religious Coping Scale (Brief RCOPE) will assess positive and negative religious coping strategies, capturing mechanisms through which faith influences mental health. Additionally, a culturally adapted measure of treatment satisfaction and perceived cultural appropriateness will be administered post-intervention.
• Statistical Analysis Plan: Quantitative data analysis will employ paired-samples t-tests to evaluate pre-post changes in primary outcome measures (PHQ-9, GAD-7, Beck Hopelessness Scale) within each ethnic group and across the combined sample. Effect sizes will be calculated using Cohen's d to determine clinical significance beyond statistical significance. Repeated measures ANOVA will examine trajectories across the four assessment points. Hierarchical regression analyses will explore whether changes in religious coping mediate improvements in depression and anxiety symptoms. Intention-to-treat analyses using multiple imputation for missing data will provide conservative effect estimates. Subgroup analyses will explore differential effectiveness across demographic characteristics and baseline severity levels.
• Community-Based Participatory Research Principles: This research embraces CBPR principles throughout all phases, ensuring equitable partnership between academic researchers and community stakeholders. Community advisory boards comprising faith leaders, community members, and service providers from each ethnic group will guide all research decisions, from protocol development through dissemination. Research team composition reflects community diversity, with cultural insiders serving as co-investigators rather than merely consultants. Capacity building is prioritized through training community members in research methods, creating sustainable community infrastructure extending beyond this project. Benefits and burdens are equitably distributed, with communities receiving training, resources, and service infrastructure as research outcomes rather than serving merely as data sources.
• Ethical Considerations: This research protocol requires Institutional Review Board approval with particular attention to vulnerable population protections. Informed consent processes will be conducted in participants' preferred languages with careful attention to ensuring comprehension and voluntary participation free from coercion. Confidentiality protections are critical given immigration-related fears and mental health stigma, with all data de-identified and stored securely. Safety protocols address potential adverse events including symptom exacerbation and suicidal ideation, with immediate access to crisis services and referral pathways. The integration of faith content requires careful ethical boundaries, ensuring that spiritual components enhance rather than replace evidence- based care and that diverse theological perspectives within communities are respected. Finally, cultural humility guides all researcher-community interactions, acknowledging power differentials and privileging community knowledge and expertise.
Results
The mixed-methods findings from both phases of this study provide comprehensive evidence supporting the feasibility, acceptability, and preliminary effectiveness of the Faith-Integrated Behavioral Health Model. Results are presented sequentially, beginning with qualitative findings from the co-design phase, followed by quantitative outcomes from the pilot intervention study, and concluding with qualitative themes from post-intervention participant experiences.
Phase 1 Qualitative Results: Framework Co-Design
Thematic analysis of 27 focus groups and 45 individual interviews across the three ethnic communities (Latino, African, Asian) yielded six primary themes that fundamentally shaped the FIBH Model design, revealing convergent and culturally specific elements of faith-integrated mental health care.
• Theme 1: Holistic Personhood-Inseparability of Spiritual and Psychological Wellbeing
Across all three communities, participants consistently articulated a unified conception of human flourishing wherein spiritual, emotional, physical, and social dimensions exist as inseparable rather than discrete domains. One Central American participant stated, "When my soul is troubled, my body suffers, my mind cannot rest, my relationships break. We are not pieces we are whole." An East African faith leader elaborated, "In our tradition, there is no word for 'mental health' separate from spiritual health. To heal the mind without addressing the spirit is like treating a fever without finding the infection." This theme directly challenged the compartmentalized approach characteristic of secular mental health services and established the theoretical foundation for integrated rather than parallel treatment of psychological and spiritual concerns.
• Theme 2: Sacred Texts as Narrative Therapy and Meaning- Making Resources
Participants across communities described sacred scriptures, religious stories, and spiritual teachings as primary frameworks through which they interpret suffering, construct meaning, and envision pathways toward healing. A South Asian participant explained, "The Bhagavad Gita teaches us about dharma even in suffering this gives me a way to understand why I struggle and how to move forward with purpose." A Latina participant shared, "The story of Ruth she was an immigrant who lost everything but found new family, new home. This story tells me God sees me, my suffering has meaning, I too can find belonging." Mental health professionals noted that clients frequently referenced religious narratives spontaneously during sessions but that clinicians typically lacked training to therapeutically engage these references. This theme informed the development of structured protocols for integrating sacred text reflection with cognitive reframing techniques.
• Theme 3: Congregation as Therapeutic Community and Support Network
Faith communities emerged as primary or exclusive sources of social support, practical assistance, and belonging for many immigrant participants. An East African refugee described, "My church family they are my only family here. When I am sad, they pray with me, bring food, help with children, remind me I am not alone." However, participants also identified limitations, with one Latino participant noting, "Sometimes the church wants to help but doesn't understand depression is medical, not just spiritual weakness." This theme highlighted both the tremendous resource potential of congregations and the critical need for mental health literacy training within faith communities, leading to the incorporation of psychoeducation components directed at both participants and their faith communities.
• Theme 4: Prayer and Contemplative Practice as Coping and Regulation Strategies
Participants described various forms of prayer, meditation, and contemplative practice as their most frequently utilized coping strategies during distress. A South Asian participant explained, "When anxiety comes, I do pranayama breathing and chant this calms my nervous system and connects me to the divine." An African participant shared, "Corporate prayer when the community prays over me. I feel the burden lift, I feel held by God and by people." Clinicians acknowledged that they routinely inquired about behavioral coping strategies but rarely about spiritual practices, representing a significant blind spot in clinical assessment. This theme informed the systematic incorporation of culturally appropriate contemplative practices as core intervention components, integrated with evidence-based relaxation and mindfulness techniques.
• Theme 5: Faith Leaders as Trusted Guides Requiring Clinical Training
Participants consistently identified clergy and faith leaders as their first point of contact during psychological distress, trusting these leaders more readily than unfamiliar mental health professionals. However, both community members and faith leaders themselves expressed concerns about limitations. One pastor stated, "People come to me with serious depression, trauma, suicidal thoughts. I want to help but I am not trained for this. I need to know when to refer, how to support someone in therapy, how prayer and counseling work together." This theme established the rationale for co-facilitation models pairing licensed clinicians with trained faith leaders, creating bridges between clinical expertise and spiritual authority.
• Theme 6: Cultural-Linguistic Congruence as Prerequisite for Therapeutic Alliance
Participants emphasized that language concordance alone proved insufficient without deeper cultural understanding. A Latina participant explained, "I tried therapy with a Latina therapist who spoke Spanish, but she was third generation, very Americanized. She didn't understand respeto, didn't understand why I couldn't talk about certain family things. I stopped going." This theme underscored the necessity of cultural insiders individuals possessing not merely linguistic ability but cultural literacy, shared experiences of immigration, and understanding of community-specific values and norms serving as intervention facilitators.
Phase 2 Quantitative Results: Pilot Intervention Outcomes
A total of 187 participants enrolled in the 12-week FIBH intervention across three communities: 64 Latino participants (34.2%), 61 African participants (32.6%), and 62 Asian participants (33.2%). Baseline demographic characteristics revealed a sample that was 68% female, with mean age of 38.4 years (SD = 11.2), mean time in the United States of 8.6 years (SD = 5.4), and 47% possessing limited English proficiency. Retention rates were excellent, with 171 participants (91.4%) completing the intervention and post-assessment.
Primary Mental Health Outcomes
Table 1 presents pre-post changes in primary outcome measures across the combined sample and by ethnic subgroup. Depression symptoms as measured by the PHQ-9 decreased significantly from baseline (M = 14.2, SD = 3.1) to post-intervention (M = 7.8, SD = 4.2), representing a mean reduction of 6.4 points, t(170) = 18.34, p < .001, Cohen's d = 1.68, indicating a large effect size. This reduction exceeded the clinically significant threshold of 5 points, with 73% of participants achieving at least 50% symptom reduction and 58% achieving remission (PHQ-9 < 5). Anxiety symptoms measured by the GAD-7 similarly demonstrated significant improvement, decreasing from baseline (M = 13.6, SD = 2.9) to post-intervention (M = 7.2, SD = 3.8), representing a mean reduction of 6.4 points, t(170) = 19.12, p < .001, Cohen's d = 1.89. Approximately 71% of participants achieved at least 50% symptom reduction.

Figure 7: Pre-Intervention and Post-Intervention Mean Scores for Depression (PHQ-9), Anxiety (GAD-7), and Hopelessness (Beck) Showing Significant Improvements with Large Effect Sizes (***p < .001)
Hopelessness, assessed via the Beck Hopelessness Scale, showed substantial improvement from baseline (M = 12.8, SD = 4.2) to post-intervention (M = 6.9, SD = 4.6), representing a mean reduction of 5.9 points, t(170) = 15.67, p < .001, Cohen's d = 1.33. This finding carries particular clinical significance given the relationship between hopelessness and suicide risk.

Figure 8: Symptom Trajectories across Four Time Points (Baseline, Week 6, Post-Intervention, 3-Month Follow-Up) Demonstrating Progressive Improvement and Maintenance of Treatment Gains
Figure 1 illustrates symptom trajectories across all four assessment points (baseline, week 6, week 12, 3-month follow- up), demonstrating progressive improvement throughout the intervention period with maintenance of gains at follow-up. Repeated measures ANOVA confirmed significant time effects for all outcomes (p < .001), with post-hoc analyses revealing that improvements achieved by mid-intervention continued through post-intervention and remained stable at 3-month follow-up.
Subgroup Analyses
Examination of outcomes by ethnic community revealed no significant differences in treatment response, with all three groups demonstrating large effect sizes: Latino participants (d = 1.62 for depression), African participants (d = 1.71), and Asian participants (d = 1.73). This finding suggests cross-cultural applicability of the culturally adapted FIBH framework. Gender comparisons similarly revealed equivalent effectiveness for male and female participants. Baseline severity moderation analyses indicated that participants with more severe baseline symptoms (PHQ-9 ≥ 15) demonstrated larger absolute improvements but equivalent proportional improvements compared to those with moderate symptoms.

Figure 9: Effect Sizes (Cohen's d) for Depression Reduction across Three Ethnic Communities Demonstrating Consistent Large Effects and Cross-Cultural Applicability of the FIBH Model
Religious Coping Mechanisms
Analysis of the Brief RCOPE revealed significant increases in positive religious coping from baseline (M = 18.4, SD = 4.1) to post-intervention (M = 24.7, SD = 3.8), t(170) = 14.23, p < .001, d = 1.58, alongside significant decreases in negative religious coping from baseline (M = 14.6, SD = 4.3) to post-intervention (M = 8.9, SD = 3.9), t(170) = -12.87, p < .001, d = 1.38. Hierarchical regression analyses demonstrated that changes in religious coping partially mediated improvements in depression (31% of variance) and anxiety (27% of variance), confirming that enhanced spiritual resources contributed meaningfully to symptom reduction beyond non-specific therapeutic factors.
Treatment Adherence and Satisfaction
Participants attended an average of 10.2 out of 12 sessions (SD = 1.8), representing 85% attendance substantially higher than typical community mental health treatment retention rates of 40-60%. Treatment satisfaction ratings averaged 4.7 out of 5 (SD = 0.4), with 94% of participants rating the intervention as "very helpful" or "extremely helpful." Ratings of cultural appropriateness averaged 4.8 out of 5 (SD = 0.3), with 96% agreeing or strongly agreeing that "this treatment respected my cultural values and faith."
Post-Intervention Qualitative Results: Participant Experiences
Semi-structured interviews with 45 participants following intervention completion yielded five dominant themes characterizing their therapeutic experiences and perceived mechanisms of change.
• Theme 1: "Felt Seen as a Whole Person"
Participants repeatedly described feeling validated in their entirety cultural identity, spiritual life, migration experiences, and psychological struggles rather than reduced to psychiatric symptoms. One participant stated, "Other therapists wanted to fix my depression but ignored who I am my faith, my culture, what I've survived. Here, everything about me mattered. I wasn't broken; I was a whole person going through hard things." This holistic recognition appeared foundational to therapeutic engagement and trust.
• Theme 2: "Reduced Stigma Through Normalization"
The group format combined with explicit discussion of mental health within faith frameworks significantly reduced internalized stigma. A participant explained, "I thought depression meant my faith was weak, that I was failing God. Learning that faith and mental health problems can exist together that even people of deep faith struggle this freed me from shame." The presence of faith leaders co-facilitating interventions powerfully communicated that seeking mental health support aligned with rather than contradicted spiritual commitment.
• Theme 3: "Sacred Practices as Practical Tools"
Participants valued the integration of familiar spiritual practices with new psychological skills. One participant shared, "I already prayed, but I learned how to use prayer specifically when anxious thoughts come combining it with breathing techniques and cognitive strategies. My faith practices became more powerful tools." This integration enhanced both the cultural acceptability of evidence-based techniques and the therapeutic sophistication of existing spiritual practices.
• Theme 4: "Community Belonging Heals Isolation"
The therapeutic group functioned as a microcosm of faith community, combating the profound isolation characteristic of immigrant experiences. A participant reflected, "For the first time since coming to America, I was in a room of people who understood my language, my struggles, my faith. We prayed together, cried together, celebrated together. I wasn't alone anymore."
• Theme 5: "Hope Restored Through Transcendent Meaning"
Participants described renewed capacity to envision meaningful futures despite ongoing hardships, attributing this shift to theological reframing of suffering. One participant stated, "I still have problems immigration status, money struggles but now I see them differently. My faith teaches that suffering can have purpose, that God works through hard times. This gives me hope that my story isn't over, that better chapters are coming." These converging quantitative and qualitative findings provide robust preliminary evidence supporting the Faith-Integrated Behavioral Health Model as an effective, culturally congruent, and highly acceptable intervention for addressing mental health needs in immigrant and minority communities.
Discussion
The converging quantitative and qualitative findings from this mixed-methods study provide compelling evidence that the Faith- Integrated Behavioral Health Model represents a viable, effective, and culturally congruent approach to addressing mental health disparities in immigrant and minority communities. The substantial effect sizes observed across depression, anxiety, and hopelessness outcomes coupled with exceptional retention rates and high participant satisfaction suggest that this model successfully addresses critical gaps in conventional mental health service delivery. This discussion explores the mechanisms underlying the model's effectiveness, examines implications for national mental health infrastructure, acknowledges methodological limitations, and proposes directions for future research and implementation.
Mechanisms of Effectiveness: Why the FIBH Model Works
Several interconnected mechanisms likely account for the observed therapeutic benefits of the Faith-Integrated Behavioral Health Model. First and most fundamentally, cultural congruence between intervention content and participants' worldviews creates conditions for genuine therapeutic engagement. Unlike conventional treatments that require clients to compartmentalize spiritual identity or translate experiences into alien psychological frameworks, the FIBH Model validates and operationalizes the holistic understanding of personhood characteristic of many immigrant and minority cultures. When participants encounter therapeutic spaces that honor rather than pathologize their spiritual interpretations of suffering, defensive barriers dissolve, allowing authentic exploration of psychological distress. The qualitative theme "Felt Seen as a Whole Person" captures this phenomenon, wherein validation of cultural-spiritual identity functions as a prerequisite for therapeutic alliance rather than as peripheral multicultural courtesy. Enhanced therapeutic alliance represents a second critical mechanism. The co-facilitation model pairing licensed clinicians with trained faith leaders synergistically combines clinical expertise with spiritual authority and cultural credibility. Faith leaders carry pre-established trust within communities, functioning as cultural bridges who implicitly communicate that mental health treatment aligns with rather than threatens spiritual commitments. This configuration dramatically reduces the trust-building time typically required in cross- cultural therapeutic relationships while simultaneously providing clinical oversight ensuring evidence-based practice integrity. The presence of faith leaders also addresses power dynamics inherent in professional-client relationships, creating more egalitarian therapeutic spaces consonant with collectivist cultural values.
Third, the FIBH Model activates existing strengths and resources rather than imposing external solutions. Participants enter treatment possessing sophisticated religious coping repertoires, supportive faith communities, and meaning-making frameworks developed over lifetimes and across generations. Conventional treatments often ignore or inadvertently undermine these assets, whereas the FIBH Model systematically mobilizes them as therapeutic tools. The documented increases in positive religious coping and their mediating role in symptom reduction confirm that enhancing spiritual resources directly contributes to psychological healing. This strength-based orientation contrasts sharply with deficit-focused approaches that implicitly position immigrant and minority clients as lacking the "right" coping strategies or cultural frameworks. Fourth, the group format leverages therapeutic factors particularly salient in collectivist cultures: universality, cohesion, and altruism. Participants discover they are not alone in their struggles, reducing shame and isolation while creating opportunities for mutual support that extend beyond formal sessions into ongoing community relationships. The integration of prayer and spiritual practices within group contexts mirrors familiar religious community experiences, creating psychological safety and resonance that purely secular group therapy cannot replicate. Finally, the explicit destigmatization of mental health struggles through faith-integrated psychoeducation addresses a primary barrier to help-seeking. When faith leaders affirm that depression and anxiety represent legitimate health conditions compatible with strong faith, participants experience permission to seek help without fearing spiritual judgment or community rejection. This reframing proves particularly powerful for populations wherein mental health stigma stems substantially from religious misunderstanding rather than merely cultural attitudes.
National Importance: Scaling the FIBH Model
The Faith-Integrated Behavioral Health Model holds profound implications for addressing multiple crises within the U.S. public health infrastructure, offering a sustainable, community-based solution to workforce shortages, fragmented care systems, and inadequate prevention networks.

Figure 10: Multi-Level Implementation Framework for National Scale-Up of the FIBH Model Showing Partnerships across Community, Institutional, and Policy Levels
Addressing Workforce Shortages Through Community Health Worker Development
The projected shortage of 250,000 mental health professionals represents an insurmountable challenge through traditional workforce development alone. The FIBH Model offers an alternative pathway by training faith leaders as specialized community health workers capable of delivering structured, evidence-based interventions under clinical supervision. The United States contains approximately 350,000 religious congregations serving immigrant and minority communities an existing infrastructure vastly exceeding current mental health service capacity. Systematic training of faith leaders in culturally adapted evidence-based protocols could rapidly expand treatment access without requiring decade-long professional education pipelines. This approach aligns with successful community health worker models in public health, wherein trained paraprofessionals extend specialist reach while providing culturally congruent care. Task-shifting mental health interventions to appropriately trained and supervised faith leaders represents pragmatic stewardship of scarce professional resources, allowing licensed clinicians to focus on severe cases requiring specialized expertise while community health workers address moderate symptoms affecting the vast majority of underserved populations.
Supporting Institutional Systems Through Strategic Partnerships
The FIBH Model creates opportunities for strategic partnerships between faith communities and overburdened institutional systems. Schools serving high-immigrant populations face epidemic rates of student mental health crises with grossly inadequate counseling resources. Faith-based mental health programs could receive referrals from school counselors, providing culturally appropriate therapeutic services while maintaining communication with schools regarding student functioning. This partnership model addresses treatment capacity constraints while keeping students connected to trusted community resources rather than alien clinical settings. Similarly, hospitals confronting high readmission rates among patients with co-occurring medical and mental health conditions could partner with faith- based programs providing transitional support, psychosocial interventions, and care coordination embedded within patients' natural community contexts. Research consistently demonstrates that community-based support reduces hospital readmissions, yet healthcare institutions lack infrastructure to provide such support precisely the infrastructure faith communities already possess. In corrections contexts, faith-based reentry programs incorporating systematic mental health components could address the profound psychological needs of returning citizens while reducing recidivism through comprehensive spiritual, social, and therapeutic support. The integration of evidence-based mental health interventions into existing prison ministry and reentry programs would enhance effectiveness without requiring entirely new institutional structures.
Creating Sustainable Prevention and Intervention Networks
Most critically, widespread implementation of the FIBH Model would establish decentralized, community-embedded mental health infrastructure addressing both prevention and intervention through naturally occurring social networks. Faith communities already function as settings for health education, social support, crisis response, and resource distribution. Systematically incorporating mental health promotion, early identification, and evidence-based treatment into these existing community functions creates sustainable infrastructure that persists independent of time- limited research projects or grant funding cycles. This community- based approach aligns with public health principles prioritizing upstream prevention and population-level interventions over downstream clinical treatment of individual cases. By addressing acculturative stress, discrimination-related trauma, and social isolation through enhanced community capacity, the FIBH Model potentially prevents the development of clinical-level disorders requiring intensive treatment. Furthermore, community-based approaches address social determinants of mental health isolation, marginalization, meaninglessness, and powerlessness that individual psychotherapy cannot resolve but that supportive faith communities inherently counteract.
Limitations and Future Research Directions
Several methodological limitations warrant acknowledgment and suggest directions for future research. The single-arm pre-post design, while appropriate for pilot feasibility and preliminary effectiveness testing, cannot definitively attribute observed improvements to specific intervention components versus non- specific factors such as attention, expectancy, or natural symptom fluctuation. Future research should employ randomized controlled designs comparing the FIBH Model against treatment-as-usual and active control conditions, allowing causal inference regarding intervention effectiveness. Generalizability limitations arise from the purposive sampling of three specific ethnic communities in particular geographic regions. While findings demonstrate cross- cultural consistency within the studied groups, applicability to other immigrant populations, different religious traditions, and varied geographic contexts requires empirical verification. Future research should expand to additional communities including Middle Eastern, Caribbean, Indigenous, and other underrepresented populations, examining whether the core FIBH framework requires substantial modification or whether cultural adaptations of a common model suffice. Selection bias represents another limitation, as participants volunteered for an explicitly faith-integrated intervention, likely over-representing individuals with strong religious commitment. Effectiveness among more secular community members or those with ambivalent religious relationships remains unknown. Future studies should examine differential effectiveness based on baseline religiosity and explore whether modifications accommodate participants across the religiosity spectrum.
The three-month follow-up period, while documenting short-term maintenance of treatment gains, provides insufficient evidence regarding long-term durability of improvements. Extended follow- up studies tracking outcomes over one to two years would clarify whether the FIBH Model produces enduring change or requires periodic booster sessions. Additionally, future research should investigate optimal intervention dosage, examining whether abbreviated or extended protocols might better serve particular populations or symptom severities. Finally, implementation science research is critically needed to translate this pilot evidence into scaled, sustainable programs. Questions regarding training requirements, supervision models, quality assurance mechanisms, financing strategies, and institutional partnership structures require systematic investigation to support widespread dissemination. Cost-effectiveness analyses comparing the FIBH Model against conventional treatments would inform policy decisions and resource allocation priorities. Despite these limitations, the substantial effect sizes, exceptional retention rates, cross-cultural consistency, and qualitative evidence of meaningful participant benefit provide strong preliminary support for the Faith-Integrated Behavioral Health Model as a promising innovation addressing urgent mental health needs while honoring the cultural and spiritual identities of immigrant and minority communities.
Conclusion
This research demonstrates that the Faith-Integrated Behavioral Health Model represents a transformative approach to addressing mental health disparities in immigrant and minority communities an approach that is simultaneously clinically effective and systemically strategic. The empirical evidence presented reveals substantial therapeutic benefits, with large effect sizes across depression, anxiety, and hopelessness outcomes, exceptional treatment retention rates of 91%, and overwhelmingly positive participant satisfaction ratings. Qualitative findings illuminate the mechanisms underlying these outcomes: cultural congruence that validates holistic personhood, enhanced therapeutic alliance through co-facilitation with trusted faith leaders, activation of existing spiritual strengths, and explicit destigmatization of mental health struggles within religious frameworks. These converging results confirm that when mental health interventions honor rather than ignore the central role of faith in clients' lives, therapeutic engagement deepens and healing accelerates. Beyond individual clinical outcomes, the FIBH Model addresses structural deficiencies within the U.S. mental health infrastructure. By training faith leaders as community health workers, this approach expands treatment capacity without requiring impossible expansions of professional workforces. By embedding services within trusted community institutions, it eliminates cultural and linguistic barriers that render conventional services inaccessible or ineffective. By creating sustainable, community-based networks, it establishes prevention and early intervention infrastructure that can persist independent of fragile funding streams. The model's potential to support overburdened schools, hospitals, and corrections systems through strategic partnerships positions it as a comprehensive solution addressing multiple interconnected public health challenges simultaneously. Realizing this potential requires coordinated action across multiple sectors. Policymakers must prioritize funding for rigorous implementation science research that translates pilot evidence into scaled, sustainable programs. Federal agencies including the Substance Abuse and Mental Health Services Administration, the Health Resources and Services Administration, and the Centers for Disease Control and Prevention should establish grant mechanisms specifically supporting faith-integrated behavioral health initiatives, recognizing that conventional funding structures inadequately accommodate community-based partnerships. State mental health authorities must develop policies facilitating collaboration between licensed providers and trained community health workers, addressing regulatory barriers that currently impede such partnerships. Healthcare systems hospitals, federally qualified health centers, managed care organizations must develop formal partnership protocols with faith communities, moving beyond ad hoc relationships toward systematic integration of community resources into care continuum planning. These protocols should specify referral pathways, information sharing procedures consistent with privacy regulations, quality assurance mechanisms, and sustainable financing models potentially including value- based payment structures that incentivize community partnerships reducing costly emergency and inpatient utilization. Academic institutions bear responsibility for preparing future healthcare professionals to practice effectively in religiously and culturally diverse contexts. Medical schools, nursing programs, social work curricula, psychology doctoral programs, and pastoral counseling training must incorporate substantive content on faith-integrated approaches, cultural humility, and community partnership models. Continuing education programs must provide current practitioners with training in cultural and spiritual assessment, appropriate integration of clients' religious resources, and collaborative practice with faith communities.
The vision toward which this research points extends beyond mere symptom reduction to fundamental transformation of how communities understand and respond to psychological suffering. When faith communities become recognized partners in mental health promotion and treatment when spiritual and psychological care integrate seamlessly immigrant and minority populations gain access to healing resources that affirm rather than threaten their identities. When evidence-based interventions incorporate rather than exclude the meaning-making frameworks through which people understand their lives, therapeutic effectiveness increases while cultural alienation decreases. When overburdened public systems collaborate strategically with community institutions possessing deep cultural trust and sustainable presence, service capacity expands while quality improves. The Faith-Integrated Behavioral Health Model offers a roadmap toward health equity grounded not in imposing majority-culture solutions on minority populations but in recognizing, respecting, and mobilizing the profound resources already present within communities. This approach builds resilient communities wherein mental health support flows naturally through existing social networks, wherein seeking help carries no stigma, wherein cultural and spiritual identities represent sources of healing rather than barriers to care. In an era of unprecedented mental health need, workforce shortages, and widening health disparities, faith-integrated care represents not merely an alternative approach but an essential component of any comprehensive strategy to advance the mental health and wellbeing of all Americans. The empirical foundation has been established; the ethical imperative is clear; the time for action is now [21-31].
References
- Viruell-Fuentes, E. A., Miranda, P. Y., & Abdulrahim, S. (2012). More than culture: structural racism, intersectionality theory, and immigrant health. Social science & medicine, 75(12), 2099-2106.
- Berry, J. W. (2005). Acculturation: Living successfully in two cultures. International journal of intercultural relations, 29(6), 697-712.
- Garcini, L. M., Peña, J. M., Galvan, T., Fagundes,C. P., Malcarne, V., & Klonoff, E. A. (2017). Mental disorders among undocumented Mexican immigrants in high-risk neighborhoods: Prevalence, comorbidity, and vulnerabilities. Journal of consulting and clinical psychology, 85(10), 927.
- Atzaba-Poria, N., & Pike, A. (2008). Correlates of parenting for mothers and fathers from English and Indian backgrounds. Parenting: Science and Practice, 8(1), 17-40.
- Williams, D. R., & Mohammed, S. A. (2009). Discrimination and racial disparities in health: evidence and needed research. Journal of behavioral medicine, 32(1), 20-47.
- Heart, M. Y. H. B. (2003). The historical trauma response among natives and its relationship with substance abuse: A Lakota illustration. Journal of psychoactive drugs, 35(1), 7-13.
- Alegría, M., Canino, G., Ríos, R., Vera, M., Calderón, J., Rusch, D., & Ortega, A. N. (2002). Mental health care for Latinos: Inequalities in use of specialty mental health services among Latinos, African Americans, and non-Latino Whites. Psychiatric services, 53(12), 1547-1555.
- Sue, D. W., Sue, D., Neville, H. A., & Smith, L. (2022). Counseling the culturally diverse: Theory and practice. John Wiley & Sons.
- Abdullah, T., & Brown, T. L. (2011). Mental illness stigma and ethnocultural beliefs, values, and norms: An integrative review. Clinical psychology review, 31(6), 934-948.
- Koenig, H. G. (2012). Religion, spirituality, and health: The research and clinical implications. International Scholarly Research Notices, 2012(1), 278730.
- Park, C. L. (2010). Making sense of the meaning literature: an integrative review of meaning making and its effects on adjustment to stressful life events. Psychological bulletin, 136(2), 257.
- Ai, A. L., Peterson, C., & Huang, B. (2003). The effect of religious-spiritual coping on positive attitudes of adult Muslim refugees from Kosovo and Bosnia. The International Journal for the Psychology of Religion, 13(1), 29-47.
- Chatters, L. M., & Taylor, R. J. (2005). Religion and families. In V. L. Bengtson, A. C. Acock, K. R. Allen, P. Dilworth- Anderson, & D. M. Klein (Eds.), Sourcebook of family theory and research (pp. 517–541). Sage Publications.
- Menjívar, C. (2003). Religion and immigration in comparative perspective: Catholic and Evangelical Salvadorans in San Francisco, Washington, DC, and Phoenix. Sociology of religion, 64(1), 21-45.
- Pargament, K. I. (2001). The psychology of religion andcoping: Theory, research, practice. Guilford press.
- Gonçalves, J. P., Lucchetti, G., Menezes, P. R., & Vallada, H. (2015). Religious and spiritual interventions in mental health care: a systematic review and meta-analysis of randomized controlled clinical trials. Psychological medicine, 45(14), 2937-2949.
- DeHaven, M. J., Hunter, I. B., Wilder, L., Walton, J. W., & Berry, J. (2004). Health programs in faith-based organizations: are they effective?. American journal of public health, 94(6), 1030-1036.
- Hankerson, S. H., & Weissman, M. M. (2012). Church- based health programs for mental disorders among African Americans: A review. Psychiatric Services, 63(3), 243-249.
- Stanford, M., & Philpott, D. (2011). Baptist senior pastors’ knowledge and perceptions of mental illness. Mental Health, Religion & Culture, 14(3), 281-290.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative research in psychology, 3(2), 77-101.
- Pargament, K. I., Koenig, H. G., & Perez, L. M. (2000). The many methods of religious coping: Development and initial validation of the RCOPE. Journal of clinical psychology, 56(4), 519-543.
- Abe-Kim, J., Takeuchi, D. T., Hong, S., Zane, N., Sue, S., Spencer, M. S., ... & Alegría, M. (2007). Use of mental health–related services among immigrant and US-born Asian Americans: results from the National Latino and Asian American study. American journal of public health, 97(1), 91-98.
- Ao, T., Taylor, E., Lankau, E., Sivilli, T. I., Blanton, C., Shetty, S., ... & Geltman, P. (2012). An investigation into suicides among Bhutanese refugees in the US 2009–2012 stakeholders report. Centers for Disease Control and Prevention, 18.
- Cook, B. L., Trinh, N. H., Li, Z., Hou, S. S. Y., & Progovac,A. M. (2017). Trends in racial-ethnic disparities in access to mental health care, 2004–2012. Psychiatric services, 68(1), 9-16.
- D'Anna, L. H., Ponce, N. A., & Siegel, J. M. (2010). Racial and ethnic health disparities: evidence of discrimination's effects across the SEP spectrum. Ethnicity & Health, 15(2), 121-143.
- Hodge, D. R. (2015). Spiritual assessment in social work andmental health practice. Columbia University Press.
- Hwang, W. C., Myers, H. F., Abe-Kim, J., & Ting, J. Y. (2008). A conceptual paradigm for understanding culture's impact on mental health: The cultural influences on mental health (CIMH) model. Clinical psychology review, 28(2), 211-227. https://doi.org/10.1016/j.cpr.2007.05.001
- Mental Health America. (2021). The state of mental health inAmerica 2021.
- Pumariega, A. J., Rothe, E., & Pumariega, J. B. (2005). Mental health of immigrants and refugees. Community mental healthjournal, 41(5), 581-597.
- U.S. Department of Health and Human Services, Health Resources and Services Administration. (2020). Designated health professional shortage areas statistics.
- Wong, E. C., Marshall, G. N., Schell, T. L., Elliott, M. N.,Hambarsoomians, K., Chun, C. A., & Berthold, S. M. (2006). Barriers to mental health care utilization for US Cambodian refugees. Journal of consulting and clinical psychology, 74(6), 1116