
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2020) Volume 5, Issue 1
Factors Associated With Severe Maternal Outcomes at a Regional Referral Hospital in South-Western Uganda: A Case-Control Study
2Department of Obstetrics and Gynecology, Massachusetts General Hospital, Boston, MA, USA
Received Date: Jan 30, 2020 / Accepted Date: Feb 05, 2020 / Published Date: Feb 13, 2020
Copyright: ©Joseph Ngonzi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The Sustainable Development Goal target is to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030. Maternal morbidity and mortality in sub-Saharan Africa remains high despite global efforts to reduce it. Severe maternal outcome studies offer a panoramic assessment of obstetric care.
Objective: The study aimed at determining the factors associated with severe maternal outcomes among women admitted at the obstetrics and gynecology ward of Mbarara Regional Referral Hospital.
Methods: In an unmatched case control (1:2) study conducted between February and May 2018, 162 pregnant women admitted on the obstetrics and gynecology ward of Mbarara Regional Referral Hospital, or who had delivered within the past 42 days were recruited. Near miss cases were defined based on the WHO criteria. Near-miss cases and events, maternal deaths and their causes were retrospectively reviewed. Three categories of risk factors (socio-demographic, obstetric and health system) were examined. P-values <0.05 were considered statistically significant. A multivariable logistic regression model was used to identify factors associated with severe maternal outcomes. All analyses were performed using Stata software (Version 12.0, StataCorp, and College Station, TX).
Results: In the four-month period there were 2301 live births, there were 45 near miss cases and 9 maternal deaths resulting in a severe maternal outcome ratio of 23.5/1000 live births, maternal near miss ratio of 19.6/1,000 live births, maternal near-miss mortality ratio of 5 and mortality index of 16.7%. Severe obstetric hemorrhage (33%), ruptured uterus (27.8%), sepsis or severe systemic infection (16.7%) and hypertensive disorders in pregnancy (16.7%) were the direct causes of severe maternal outcomes. About seventy-seven percent (77.8%) of the mothers with severe maternal outcomes were referred in from the peripheral health facilities, with a 4-time risk increased risk of a severe maternal outcome (aOR, 4.00; 95 % CI, 1.84-6.66, p-<0.001).
Conclusion: Of the severe maternal outcomes, direct causes were the most prevalent and most of which are preventable. Being referred in was significantly associated with severe maternal outcomes. The maternal near miss indicators indicate need for improved quality.
Keywords
Maternal Mortality, Mbarara University, Severe Maternal Outcomes
Background
The Sustainable Development Goal target is to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030 with no country having MMR of more than twice the global average. Of all maternal deaths, 99% occur in developing countries and majority of the maternal deaths occurring in low-resource settings can be prevented [1,2]. Sub-Saharan Africa is the riskiest region in the world with unacceptably high levels of maternal mortality; 1 in 38 unlike in the developed world where it is 1 in 3700 [3]. The current maternal mortality ratio according to the Uganda Demographic and Health Surveys of 2016 is 336 per 100,000 live births while in Mbarara Regional Referral Hospital the maternal death risk is 531 deaths/100,000 live births (Annual Health Sector Performance Report, 2017/2018) which is unacceptably high.
A maternal death is defined as the death of a woman during pregnancy or within forty-two days of termination of pregnancy irrespective of the duration or site of pregnancy, from any causes related to pregnancy, delivery or its management and not from accidental or incidental causes (10th International Classification of Diseases). A maternal near miss refers to a woman who, being close to death, survives a complication that occurred during pregnancy, delivery or up to 42 days after the end of her pregnancy [4]. Both a maternal death and maternal near miss are considered a severe maternal outcome. Since poor quality obstetric services continue to be an important associated factor of maternal mortality, and because maternal near-misses are a useful complement to the investigation of maternal mortality, severe maternal outcome studies offer a panoramic assessment of obstetric care [5].
The major risk factors influencing severe maternal outcomes include age (extremes of age that is under 16 years or over 30 years of age), parity (primiparity or grand parity i.e. five or more previous births) , low socio-economic status, the timing of care in women who develop obstetric complications (three delays), mode of delivery (most ‘near-miss’ studies showed that up to 50% or more of deliveries were by caesarean section, availability of medical supplies and the availability of a skilled attendant at delivery [6-8]. Factors contributing to obstetric near misses vary from one geographical area to another and from one country to another. In the developing world the causes of near miss were similar to those of maternal deaths prevailing in the area. According to Current Approach to Reduction of Maternal Mortality, the global causes of maternal mortality were hemorrhage (24.8%), Sepsis (14.9%), eclampsia (12.9%), obstructed labor (6.9%) and unsafe abortions (12.9%). For Uganda it was found that the leading causes were hemorrhage (26%), sepsis (22%), eclampsia (6%), obstructed labor (13%) and unsafe abortions (8%). While study done in MRRH found that in general direct causes contributed 77.7 % while the indirect the remaining 22.3 %. Puerperal sepsis (30.9 %) was the leading cause followed by post- partum hemorrhage (21.6 %), complications of abortions (10.8 %) then hypertensive disorders (14.4 %) [9].
Despite MRRH being a tertiary hospital in the south-western Uganda with a large catchment area, 7721 deliveries per year (AHSPR 2017/2018), there is was not yet a study done to review maternal near misses. Yet maternal mortality remains one of the major public health problems of our time, and poor quality obstetric services continue to be an important associated factor. The pathway of maternal morbidity is a continuum sharing pathological and circumstantial factors from non-severe maternal outcome, maternal near miss through to maternal death. By evaluating these cases with severe maternal outcomes (both “near-miss” cases and maternal deaths), much was learnt about the processes in place (or lack of them) for the care of pregnant women in MRRH. This study generated complementary information to that obtained from mortality studies done in MRRH. This study aimed at determining the maternal near miss indicators and factors (socio-demographic, obstetric, medical and health system) associated with severe maternal outcomes at Mbarara Regional Referral Hospital.
Methods
Study Site, Population and Design
An unmatched case control study was conducted between February 6, 2018 to May 18, 2018 to determine the magnitude and factors associated with severe maternal outcomes among women who were pregnant or had delivered within 42 days admitted at the obstetrics and gynecology ward of Mbarara Regional Referral Hospital (MRRH); a teaching hospital located in south-western Uganda with 24 districts within its catchment area, an estimate of 8.8 million people. Approximately 9,000 deliveries occur per year in this facility with a MMR of 531 per 100,000 live births and a caesarean delivery rate of 40% (Annual Health Sector Performance Report, 2017/2018). The physician to patient ratio ranges from 1:8 during the day to 1:14 during the night. The nursing/midwife to patient ratios are approximately 1:25 during the day and 1:50 at night. The hospital is equipped with surgical theatres, a blood bank and a general intensive care unit. Teams of pediatricians (who manage most of the neonatology cases), obstetricians, anesthesiologists and intensive care specialists are available round the clock. Also specialists in other surgical and clinical fields working in other units of the university hospital complex are readily available for consultation.
Selection and Definition of Cases and Controls
A mother was considered eligible for enrolment if they had an obstetric complication. And they were considered for inclusion as a case if they met the WHO maternal near miss criteria for identifying life threatening conditions at the point of hospital discharge or if it were a maternal death [10]. Controls were women on the MRRH obstetrics and gynecology ward who were pregnant or in puerperium that did not have any obstetric complication by the time of discharge. For every case recruited into the study, two controls were randomly selected from the same section (i.e. post-natal, ante natal or gynecology) of the ward within the same study period.
Women that were excluded included those that chose not to participate in the study, those who met the WHO definition of a maternal death but were dead on arrival and women who had been recruited before as a control, discharged then later developed a complication and were re-admitted.
Definition of a Severe Maternal Outcome
A maternal death or a maternal near-miss was considered a severe maternal outcome. A maternal death was any woman who died during pregnancy or within forty-two days of termination of her pregnancy irrespective of the duration or site of pregnancy, from any causes related to pregnancy, delivery or its management and not from accidental or incidental causes.
A maternal near miss was a woman who at the point of discharge from the hospital had been close to death however survived a complication that occurred during pregnancy or delivery up to 42 days after the end of her pregnancy. The World Health Organization (WHO) near miss criteria tool was utilized to identify those with life threatening conditions [10].
Data Collection
At the point of discharge from hospital or if a mother died, with the aid of an interviewer-administered questionnaire, mother’s clinical examination, investigations and duteous review of patient chart records, data was collected on socio-demographic characteristics, obstetric history, current pregnancy history and both pregnancy and delivery outcomes. Data analysis wasn’t done for mothers enrolled but were classified as having non- life threatening obstetric complications by the WHO maternal near miss tool criteria [10]. For every case recruited into the study, two controls were randomly selected from the same section of the ward (post-natal, ante natal or gynecology), within the same study period. For the mothers who died information was picked from the care takers and kinsmen as well as retrospectively from the medical charts.
Sample Size and Statistical Analysis
Using the Kelsey et al formula and a ratio of controls to cases of 2, an assumed power of 80%, a 5% accepted probability of making an error, a 38% hypothetical proportion of women with severe maternal outcomes that had had a caesarean delivery was 38% was used to estimate my sample size to 54 cases and 108 controls after factor in the possibility of incomplete charts or data collected of up to 04% of the participants on both the control and case arms [11].
Data Analysis
Questionnaires and patient chart information was entered into a Research Electronic Data Capture (REDCap) database then exported to Excel where it was cleaned and then analyzed using computer software Stata software (Version 12.0, StataCorp, College Station, TX). Computation of descriptive characteristics of mothers with severe maternal outcomes (cases) and controls near miss was done, whereby categorical variables were presented as frequencies and percentages while numerical variables are presented as means and medians (with standard deviations and inter-quartile ranges respectively).
Socio-demographic, obstetric and health system characteristics and outcomes were compared between cases and controls using Chi-squared analysis for categorical variables and student’s t-test for continuous variables. We did a bivariate analysis analysis of socio-demographic, obstetric and health system factors associated with severe maternal outcomes among the study participants and adjusted relative risks computed. We considered P-values of < 0.1 to be statistically significant and also included those that were of clinical significance. The final model was created using backwards stepwise elimination and all variables with P-values< 0.05 in the final model were considered significant independent predictors of the outcome.
In addition, the following maternal near miss indicators were computed, the maternal near miss (MNM) incidence ratios (MNM/ 1000 live births), the severe maternal outcome ratio ((MD + MNM)/1000 live births), the severe maternal mortality index (MD / (MD+MNM) expressed as a percentage).
Ethics
Prior to data collection all enrolled women provided written informed consent. Participants below 18 years of age were enrolled as emancipated minors on basis of pregnancy. Ethical clearance to carry out the study was obtained from; the Mbarara University of Science and Technology department of Obstetrics and Gynecology, the Faculty of Medicine Ethical Research Committee, Research Ethics Committee, of Mbarara University of Science and Technology [11-13]. Permission was also obtained from Mbarara Regional Referral Hospital. At all stages of this research, privacy and confidentiality were observed.
Results
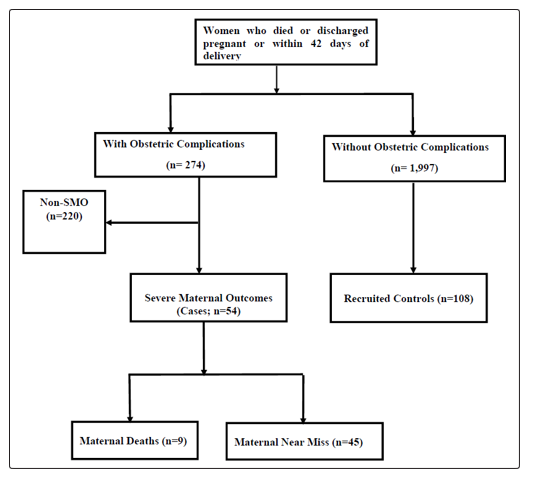
Over the four-month study period there were 2301 live births. During the same study period the total number of mothers who were discharged pregnant or within 42 days of delivery and those who had died were 2,271. Of these, 274 mothers had obstetric complications while 1,997 had none. 220 of the mothers with obstetric complications didn’t have life threatening complications i.e. they were not a severe maternal outcome. The remaining 54 were severe maternal outcomes; 5 of which were maternal deaths and the rest maternal near misses (Figure 1).
The median age among the controls was 25 years with IQR and among the cases was 28 years with IQR [14,15]. Of the mothers with severe maternal outcomes, 3.7% were between 16-19 years, 55.6% between 20-29 years and 40.7% above 30 years. While for the controls 12.96% were between 16 and 19 years of age, 62% between 20 and 29, and 25% above 30 years of age (Table 1).
Participants Baseline Characteristics
Table 1. Socio-Demographics, Obstetric and Health System Factors of Study Participants, Comparing those with Severe Maternal Outcomes (Cases) and those without any Obstetric Complication (Control Group)
|
Characteristics (n=162) |
Controls n(%), (n=108) |
Cases n(%), (n=54) |
P-value* |
|
Age |
|||
|
16-19 yrs |
14 (12.96) |
2 (3.7) |
0.042 |
|
20-29 yrs |
67 (62.04) |
30 (55.56) |
|
|
>30 yrs |
27 (25.00) |
22 (40.74) |
|
|
Parity |
|||
|
P1 |
42 (38.89) |
10 (18.52) |
0.031 |
|
P2-P4 |
45 (41.67) |
29 (53.70) |
|
|
≥P5 |
21 (19.44) |
15(27.78) |
|
|
Marital status |
|||
|
Married |
82 (75.93) |
38 (70.37) |
0.749 |
|
Single |
15 (13.89) |
11 (20.37) |
|
|
Cohabiting |
8 (7.41) |
4 (7.41) |
|
|
Divorced |
3 (2.78) |
1 (1.85) |
|
|
Occupation |
|||
|
Peasant |
71 (65.74) |
35 (64.81) |
0.884 |
|
Housewife |
22 (20.37) |
11 (20.37) |
|
|
Student |
4 (3.70) |
1 (1.85) |
|
|
Professional |
11 (10.19) |
7 (12.96) |
|
|
Religion |
|||
|
Moslem |
11 (10.19) |
4 (7.41) |
0.161 |
|
Protestant |
37 (34.26) |
27 (50.00) |
|
|
Catholic |
49 (45.37) |
16 (29.63) |
|
|
Pentecostal |
9 (8.33) |
7 (12.96) |
|
|
SDA |
2 (1.85) |
0 (0.00) |
|
|
Education (Mother) |
|||
|
Low Education |
63 (58.33%) |
28 (51.85%) |
0.433 |
|
High Education |
45 (41.67%) |
26 (48.15%) |
|
|
Residence |
|||
|
Urban |
31 (28.70) |
14 (25.93) |
0.710 |
|
Rural |
77 (71.30) |
40 (74.07) |
|
|
Distance |
|
|
|
|
≤5km |
77 (71.30) |
33 (61.11) |
0.191 |
|
>5km |
31 (28.70) |
21 (38.89) |
|
|
Health System Factors |
|||
|
Referral Status |
|||
|
Not referred |
58 (53.70) |
12 (22.22) |
<0.001 |
|
Referred |
50 (46.30) |
42 (77.78) |
|
|
Obstetric Factors |
|||
|
Number of ANC Visits |
|||
|
None |
7 (6.48) |
2 (3.70) |
0.078 |
|
1 |
5 (4.63) |
2 (3.70) |
|
|
2 |
7 (6.48) |
10 (18.52) |
|
|
3 |
22 (20.37) |
15 (27.78) |
|
|
4 |
46 (42.59) |
21 (38.89) |
|
|
>4 |
21 (19.44) |
4 (7.41) |
|
|
HIV Sero-status |
|||
|
Negative |
104 (96.30) |
48 (88.89) |
0.065 |
|
Positive |
4 (3.70) |
6 (11.11) |
|
legend: Km-Kilometre; HIV-Human Immuno-deficiency Virus; ANC-Antenatal Care; SDA-Seventh Day Adventist
Majority of the mothers for both the cases and controls were married peasant farmers, with only a primary level of formal education, living in the rural area and most lived less than 5Km from the nearest government owned health facility. Transport charges were used as a proxy to assess distance. As opposed to mothers without obstetric complications, majority of the mothers with severe maternal outcomes were in-referrals (77.8%) while majority of the controls were mothers who were not in-referrals (53.7%). The distribution of the baseline characteristics among the cases and controls is shown in (Table 1).
Using backward stepwise elimination into the multivariate logistic regression, this study observed that the only significant factor associated with severe maternal outcomes after adjusting for confounders was referral status. There was an increased risk of a severe maternal outcome if referred from the peripheral health facilities (aOR, 4.00; 95 % CI, 1.84-6.66, p-<0.001) (Table 2). Factors Associated with Severe Maternal Outcomes
Table 2: Bivariable Logistic regression table showing factors associated with severe maternal outcomes
|
Characteristic |
cOR [95% CCI] |
P-value |
|
Age |
Ref |
|
|
20-29 yrs |
3.13 [0.67 - 14.66] |
0.147 |
|
>30 yrs |
5.70 [1.16 - 27.82] |
0.031 |
|
Parity |
||
|
P1 |
Ref |
|
|
P2-P4 |
2.71 [1.17 - 6.22] |
0.019 |
|
≥P5 |
3 [1.15 - 7.81] |
0.024 |
|
Referral Status |
|
|
|
Not referred |
Ref |
|
|
Referred |
4.06 [1.93- 8.55] |
<0.001 |
|
HIV Sero-status |
|
|
|
Negative |
Ref |
|
|
Positive |
3.25 [0.88 - 12.05] |
0.078 |
Severe obstetric hemorrhage (33.3%), ruptured uterus (27.8), hypertensive disorders (16.7%) and severe systemic infections (16.7%) were the leading morbidity among women with potentially life-threatening conditions (severe maternal outcomes) (Table 3).
Maternal Near Miss Indicators
Table 3: Morbidity conditions among women with potentially life-threatening conditions
|
Morbidity conditions |
Number |
Percentage of SMO |
|
Number of women with severe complications |
||
|
Severe obstetric hemorrhage |
18 |
33.3 |
|
Severe pre-eclampsia |
4 |
7.4 |
|
Eclampsia |
5 |
9.3 |
|
Sepsis or severe systemic infection |
9 |
16.7 |
|
Ruptured uterus |
15 |
27.8 |
|
Other complications associated with severe maternal |
3 |
5.5 |
Legend: SMO-severe maternal outcome
The study observed a severe maternal outcome ratio of 23.5 per 1000 live /births, a maternal near-miss ratio of 19.6 per 1000 live births, maternal near-miss mortality ratio of 5 and a mortality index of 16.7%.
Discussion
Factors Associated With Severe Maternal Outcomes
The factor that was found significant at multivariate analysis was referral status. About 77.8% of the mothers with severe maternal outcomes were referred in from the peripheral health facilities. This study found that there was a 4-time risk (aOR 4.00, 95% CI 1.84-6.66, p-<0.001), of a severe maternal outcome for a mother who was referred in from the peripheral health facilities as opposed to one who wasn’t referred in. In a study done here in MRRH it was found that having been referred from another health facility was associated with maternal mortality (OR 5.0; 95 % CI, 2.9–10.0) (9). Related studies have showed that patients who are referred from lower health facilities are usually in critical states and their outcomes are poorer as compared to those not referred [12]. Being referred from a peripheral health facility in critical condition is associated with poor obstetric outcomes, including mortality [16]. It is possibly due to challenges in the referral system for example, late referrals or delay in securing transport especially due to costs that the mothers cannot afford, resulting in the high proportion of women that present at the hospital already in a severe health condition.
Although in this study, age was not found statistically significant on the multivariate model, the bivariate analysis model demonstrated an increasing risk of developing a severe maternal outcome with advancing maternal age. These findings are consistent with a systematic analysis for the Global Burden of Disease Study in 2013 which found that MMR was highest in the oldest age groups [17]. The largest number of severe maternal outcomes occurred in the age groups between 20-29, and this is probably because these are the ages at which women are most likely to give birth. The more likely to give birth the more exposed to risks associated with giving birth.
Grand multi-parity is a major public health concern which has been associated with higher risk of adverse intrapartum complications compared with women of lesser parity especially among developing countries. The term “grand multipara” was introduced by Solomon in 1934, he called them the “the dangerous multiparas” [18]. Parity was not found to be significant in this study as a factor associated with severe maternal outcomes. Similarly a study done in rural Cameroon observed no significant difference in the delivery outcomes between grand multiparous women and those with lesser parity [19].
A secondary analysis of the WHO Multi-country Survey to assess the association of levels of education on access to health care and severe maternal outcomes among women delivering in health care facilities in 29 countries observed that in countries with poorer markers of social and economic development, women with lower levels of education were at greater risk for severe maternal outcomes [13]. In this study mothers with a primary, or no education at all, were considered to be a low education while secondary and tertiary education was considered high level education. Most of the mothers were of a low education level however was not found to have a significant association with severe maternal outcomes.
Maternal Near Miss Indicators
During the period of our study we had 2,301 live births with a severe maternal outcome ratio of 23.5 per 1000 live births which is way high compared to the findings observed in a similar study done within similar settings done in two referral hospitals; Mulago and Jinja located in the central and eastern regions respectively which found a severe maternal outcome ratio of 9.99 per 1000 live births [11]. In a World Health Organization multi-country survey conducted in 357 health facilities in 29 countries from the different continents in 2011, a severe maternal outcome ratio of 9.9 per 1000 live births was observed, which was way lower that the one observed in our study [19]. However, the findings of this study were relatively consistent with those of studies done in Tanzania at 26.1/ 1000 live births and Mozambique at 22.7/ 1000 live births [15,20]. In this study we report a maternal near miss incidence (ratio) of 19.6 per 1000 live births which is twice higher than that observed in the study that was done in Mulago and Jinja referral hospitals (8.42 per 1000 live births) and that observed in the World Health Organization multi-country survey at 8.3 per 1000 live births [19]. It still is however almost similar to that found in a study in similar settings in Mozambique at 20.2 per 1000 live births [20].
The difference between the findings in our study and the one done by Nakimuli in Mulago, Uganda could be attributed to the fact that, as opposed to our study, theirs was a prospective cohort study, conducted over a longer (one year), in two hospitals in different regions central and eastern Uganda. Noteworthy, since severe maternal outcome ratio and maternal near miss ratio as indicators give an estimate of the amount of care and resources that would be needed in an area or facility this gives an estimate of the how much more amount of care and resources the MRRH as a facility would need compared to these other facilities and regions.
In this study the maternal near-miss mortality ratio was 5, which was relatively similar to the one observed in the Mulago and Jinja study (5.3) and that observed in the World Health Organization multi-country survey (5.2) however it’s way lower than the maternal near-miss mortality ratio observed in the World Health Organization multi¬country survey among the countries (N=15) with moderate maternal mortality ratio at 16.8 [19]. Our observed maternal mortality index [16.7%] was relatively similar to the one observed in the World Health Organization multi-country (N=29) survey (16.1%) however compared to the survey among the countries (N=15) with moderate maternal mortality ratio at 5.6% it was way higher. The maternal mortality index findings in our study were also higher than the one in the Mulago and Jinja study [15.8%] and Ethiopia [14.5%] [6]. This implies that a bigger proportion of mothers with severe maternal outcomes die at MRRH. The mortality index is lower than the one observed in Mozambique [21.8%] and Rwanda [26%] [20,21]. The difference in the findings is probably because both these studies were cross-sectional, and they used a different maternal near miss criteria (Clinical diagnostic criteria) instead of the recommended WHO maternal near miss criteria of 2009. Higher maternal near-miss mortality ratios indicate better care while higher Mortality index imply that more women with life-threatening conditions die and thus low quality of care, whereas the lower the index the fewer women with life-threatening conditions die and therefore better quality of care [22].
All the severe maternal out comes were caused by direct causes. Among the severe maternal out comes obstetric hemorrhage (33%) contributed the most followed by ruptured uterus (27.8%), sepsis or severe systemic infection (16.7%), hypertensive disorders in pregnancy (16.7%), then other complications (Venous Thromboembolic events (VTEs) at 5.5%). Similarly in the World Health Organization multi-country survey conducted in 357 health facilities in 29 countries obstetric hemorrhage was the leading cause (26.7%) of severe maternal outcomes followed by hypertensive disorders of pregnancy (25.9%) [19]. Our study was in agreement with a systematic review to determine the causes of maternal deaths conducted by the WHO which observed that hemorrhage was the leading cause of maternal deaths in Africa at 33.9% [23]. Similarly, hemorrhage accounted for the most common event among near miss cases in other low income countries; in Maputo (hemorrhage 58.0%) and Nigeria (hemorrhage 41.3%) [20,24]. A study done in this very hospital and ward revealed that the most frequent cause of maternal mortality was puerperal sepsis (30.9 %), followed by obstetric hemorrhage (21.6 %), hypertensive disorders in pregnancy (14.4 %), abortion complications (10.8 %) [9].
This difference in the leading direct cause is probably because while the study done in MRRH in 2016 included all obstetric complications, in this study we only considered severe maternal outcomes (MNMs and MDs) with a strict criterion for the definition of maternal near misses. The other possible reason for the difference is probably due to the efforts that have been adopted by the team of clinicians on the ward to curb sepsis since the dissemination of the study findings and these included; audits of mothers with sepsis, the emphasis on hand washing and antiseptic hand gel use, allowing for a longer time of observation before discharge for cases believed to be prone to sepsis from 3 to 5 days and the improvement on antibiotic administration with encouragement to start oral antibiotics on the second day post-surgical operation. This was because the staffing levels did not allow for proficient IV antibiotic administration in the evening and at night.
The high rate of uterine rupture is probably due to a temporal health system management challenge at the peripheral units where the theatres were under renovation. All mothers that had ruptured uteri were in- referrals with an already diagnosed condition.
Conclusion
Of the severe maternal outcomes, direct causes were the most prevalent and most of which are preventable. Being referred in was significantly associated with severe maternal outcomes. The maternal near miss indicators indicate need for improved quality.
References
- Organization WH, UNICEF. Trends in maternal mortality: 1990-2015: estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division 2015.
- Regmi P, Van Teijlingen E, Hundley V, Simkhada P, Sharma S, et al. (2016) Sustainable Development Goals: relevance to maternal and child health in Nepal. Health Prospect: Journal of Public Health 15: 9-10.
- Organization WH, UNICEF. Trends in maternal mortality: 1990 to 2013: estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division: executive summary 2014.
- Organization WH, Evaluating the quality of care for severe pregnancy complications: the WHO near-miss approach for maternal health 2011.
- Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, et al. (2010) Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. The lancet 375: 1609-1623.
- Kwast BE, Liff JM (1988) Factors associated with maternal mortality in Addis Ababa, Ethiopia. International journal of epidemiology 17: 115-121.
- Murphy DJ, Charlett P (2002) Cohort study of near-miss maternal mortality and subsequent reproductive outcome. European Journal of Obstetrics & Gynecology and Reproductive Biology 102: 173-178.
- de Souza JPD, Duarte G, Basile-Filho A (2002) Near-miss maternal mortality in developing countries. European Journal of Obstetrics & Gynecology and Reproductive Biology 104: 80.
- Ngonzi J, Tornes YF, Mukasa PK, Salongo W, Kabakyenga J, et al. (2016) Puerperal sepsis, the leading cause of maternal deaths at a Tertiary University Teaching Hospital in Uganda. BMC pregnancy and childbirth 16: 207.
- Souza JP, Cecatti JG, Haddad SM, Parpinelli MA, Costa ML, et al. (2012) The WHO maternal near-miss approach and the maternal severity index model (MSI): tools for assessing the management of severe maternal morbidity. PloS one 7: e44129.
- Nakimuli A, Nakubulwa S, Kakaire O, Osinde MO, Mbalinda SN, et al. (2016) Maternal near misses from two referral hospitals in Uganda: a prospective cohort study on incidence, determinants and prognostic factors. BMC Pregnancy and Childbirth 16: 24.
- Kongnyuy EJ, Mlava G, Van Den Broek N (2009) Facility-based maternal death review in three districts in the central region of Malawi: an analysis of causes and characteristics of maternal deaths. Women’s Health Issues 19: 14-20.
- Tunçalp Ö, Souza J, Hindin M, Santos C, Oliveira T, et al. (2014) Education and severe maternal outcomes in developing countries: a multicountry cross-sectional survey. BJOG: An International Journal of Obstetrics & Gynecology 121: 57-65.
- Ajong AB, Agbor VN, Simo LP, Noubiap JJ, Njim T. (2019) Grand multiparity in rural Cameroon: prevalence and adverse maternal and fetal delivery outcomes. BMC pregnancy and childbirth 19: 233.
- Nelissen EJ, Mduma E, Ersdal HL, Evjen-Olsen B, van Roosmalen JJ, et al. (2013) Maternal near miss and mortality in a rural referral hospital in northern Tanzania: a cross-sectional study. BMC pregnancy and childbirth 13: 141.
- Ronsmans C, Graham WJ, group LMSSs. (2006) Maternal mortality: who, when, where, and why. The lancet 368: 1189-1200.
- Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, Shackelford KA, Steiner C, et al. (2014) Global, regional, and national levels and causes of maternal mortality during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. The lancet 384: 980-1004.
- Lyrenäs S (2002) Labor in the grand multipara. Gynecologic and obstetric investigation 53: 6-12.
- Souza JP, Gülmezoglu AM, Vogel J, Carroli G, Lumbiganon P, et al. (2013) Moving beyond essential interventions for reduction of maternal mortality (the WHO Multicountry Survey on Maternal and Newborn Health): a cross-sectional study. The lancet 381: 1747-1755.
- David E, Machungo F, Zanconato G, Cavaliere E, Fiosse S, et al. (2014) Maternal near miss and maternal deaths in Mozambique: a cross-sectional, region-wide study of 635 consecutive cases assisted in health facilities of Maputo province. BMC pregnancy and childbirth 14: 401.
- Rulisa S, Umuziranenge I, Small M, van Roosmalen J (2015) Maternal near miss and mortality in a tertiary care hospital in Rwanda. BMC pregnancy and childbirth 15: 203.
- Cecatti JG, Souza JP, Neto AFO, Parpinelli MA, Sousa MH, et al. (2011) Pre-validation of the WHO organ dysfunction based criteria for identification of maternal near miss. Reproductive Health 8: 22.
- Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF (2006) WHO analysis of causes of maternal death: a systematic review. The lancet 367: 1066-1074.
- Adeoye IA, Onayade AA, Fatusi AO (2013) Incidence, determinants and perinatal outcomes of near miss maternal morbidity in Ile-Ife Nigeria: a prospective case control study. BMC pregnancy and childbirth 13: 93