



Research Article - (2018) Volume 3, Issue 1
External Counterpulsation (ECP) Therapy as an Effective Treatment among Patients with Heart Failure undergoing Cardiac Rehabilitation
Received Date: Nov 25, 2018 / Accepted Date: Dec 13, 2018 / Published Date: Dec 15, 2018
Copyright: ©JS Ho, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: External counterpulsation (ECP) is a noninvasive procedure using lower limbs pressure cuffs to improve coronary artery blood flow and offload the heart. There is currently no data on the effects of ECP among patients undergoing cardiac rehabilitation (CR). This pilot study aims to determine whether ECP improves exercise capacity among patients with heart failure or post acute myocardial infarction undergoing cardiac rehabilitation.
Methods: This is a prospective randomised-controlled pilot study of the effect of ECP in patients with mild to moderate heart failure or post-acute myocardial infarction undergoing CR. Eligible patients were randomised at ratio of 1:1 to either combination of CR and ECP or CR only. All subjects received up to 16 sessions of conventional CR. For the combination arm, subjects received up to 16 one-hour sessions of one-hour ECP therapy following each CR session. All underwent baseline cardiopulmonary testing (CPET) and NT-Pro BNP determination and after completion of study.
Results: A total of 4 patients were enrolled in the study from June 2016 to Jan 2017. Two were randomised to combination arm and two into CR arm. Post treatment VO2MAX improved 12 % in the combination arm (23.3±5.6 ml/min/kg from20.8±5.3 ml/min/kgat baseline) compare to 5% in the CR arm (23.0±6.2 ml/min/kg from21.9±2.3 ml/min/kg at baseline). There were no significant difference in the post treatment VO2MAX between groups, p=0.97. There was a 16% increased in post treatment maximum oxygen pulsein the combination group (14.4±1.0ml/beat from12.4±0.5ml/beat at baseline) compare to a 7.8% increased in the CR group (12.4±2.2ml/beat from11.5±1.4ml/beat at baseline). Interestingly, NT proBNP level worsened post treatment in the combination group (447.5±563.6 pre treatment to 472.7±560.5 post treatment), whereas improved in the CR only group (950.5±522.9 pre treatment to 327.5±202.6 post treatment).
Conclusion: Cardiac Rehabilitation is known to improve exercise capacity among heart failure patients. ECP can further enhanced maximum oxygen consumption and maximum oxygen pulse in patients with mild to moderate degree of heart failure or post myocardial infarction undergoing cardiac rehabilitation. More studies with larger numbers are needed to prove this benefit of ECP
Keywords
External counterpulsation, Cardiac rehabilitation, Maximum oxygen consumption, Maximum oxygen pulse, Heart failure, Cardiac rehabilitation
Background
External counterpulsation (ECP) is a noninvasive procedure using lower limbs pressure cuffs to improve coronary artery blood flow and offload the heart. Itimitates the hemodynamic outcome of an intra- aortic balloon pump which is an invasive method. ECP is inflated sequentially during diastolic phase of the cardiac cycle. This can effectively increase diastolic and coronary pressures and leads to improved coronary flow. Furthermore, rapid deflation of the cuffs can reduce systolic pressure in the aorta thus reducing the workload of the heart. ECP has been shown to reduce angina symptoms and prolong time to exercise induced ischemia [1]. Moreover, ECP enhanced exercise capacity, NYHA classification and quality of life, in patients with mild to moderate heart failure [2].
There is currently no data on the effects of ECP among patients undergoing cardiac rehabilitation (CR). This pilot study aims to determine whether ECP improves exercise capacity among patients with mild to moderate heart failure or post myocardial infarction undergoing cardiac rehabilitation
Methods
Study Design
This is a prospective randomised-controlled pilot study conducted at the CR department at the National Heart Centre of Singapore. After providing informed consent, eligible patients were randomised at ratio of 1:1 to either combination of CR and ECP or CR only. For the combination arm, subjects received up to 16 one-hour sessions of CR together with one-hour ECP therapy following each CR session. For the CR arm, subjects received up to 16 one-hour sessions of CR only. All eligible patients underwent baseline cardiopulmonary testing (CPET) and NT-Pro BNP determination within two-weeks prior to initiation of ECP and within one -week after completion of study.
Results
A total of 4 patients were enrolled in the study from June 2016 to Jan 2017. The study was only able to recruit 4 patients out of the intended 16. Two patients were randomised to the combination arm and two into the CR arm. Mean age was 54.5±6.4 years and 47.0±5.7 years respectively between the combination and CR arm. All participants were male, mainly of Chinese race. Baseline characteristic BMI, NYHA class and baseline LVEF were comparable. All of them had history of ischemic heart disease and hyperlipidemia. (Table 1)
Table 1: Results
|
|
ECP and CR |
CR only |
p value |
|
Mean Age ( years )±SD |
54.5±6.4 |
47.0±5.7 |
0.34 |
|
Male ( No.) |
2 |
2 |
0.5 |
|
Race, Chinese (No.) Race, Malay (No.) |
1 1 |
2 0 |
0.5 |
|
Mean BMI (kg/m2) ±SD |
24.8±2.0 |
27.7±3.7 |
0.46 |
|
NYHA Class |
1 and II |
1 and II |
1.0 |
|
Baseline LVEF ( %) |
40.5± 6.4 |
34.5± 9.2 |
0.54 |
|
Hypertension (No.) |
2 |
1 |
0.5 |
|
Diabetes mellitus ( %) |
2 |
1 |
0.5 |
|
Dyslipidemia (%) |
2 |
2 |
1.0 |
|
Ischemic Heart Disease (No.) |
2 |
2 |
1.0 |
|
Chronic Kidney disease (No.) |
0 |
0 |
1.0 |
|
Smoking history (No.) |
1 |
2 |
0.5 |
|
Coronary artery Stenting (No.) |
1 |
1 |
1.0 |
|
Coronary artery bypass surgery (No.) |
1 |
1 |
1.0 |
|
|
|
|
|
|
Mean Pre treatment NTproBNP |
447.5±563.6 |
950.5±522.9 |
0.42 |
|
Mean Post treatment NTpro BNP |
472.7±560.5 |
327.5±202.6 |
0.78 |
|
Mean Pre treatment VO2Max (ml/min/kg) |
20.8±5.3 |
21.9±2.3 |
0.82 |
|
Mean Post treatment VO2Max (ml/min/kg) |
23.3±5.6 |
23.0±6.2 |
0.97 |
|
Mean Pre treatment METS |
5.9±1.5 |
8.0±1.3 |
0.33 |
|
Mean Post treatment METS |
6.7±1.6 |
6.5±1.7 |
0.95 |
|
Mean Pre treatment MaxO2pulse (ml/beat) |
12.4±0.5 |
11.5±1.4 |
0.60 |
|
Mean Post treatment MaxO2pulse (ml/beat) |
14.4±1.0 |
12.4±2.2 |
0.37 |
Note: VO2Max indicates maximum oxygen consumption; MaxO2pulse indicates maximum oxygen pulse.
Improvement in post treatment maximum oxygen consumption (VO2MAX) was observed in both the combination arm (23.3±5.6 ml/min/kg from 20.8±5.3 ml/min/kgat baseline) and CR arm (23.0±6.2 ml/min/kg from 21.9±2.3 ml/min/kg at baseline). The combination arm VO2MAX improved 12% from baseline, whereas the CR arm improved 5%.
Similarly, post treatment maximum oxygen pulsewere much increased compare to baseline in both the combination arm (14.4±1.0ml/beat from 12.4±0.5ml/beat at baseline) and CR arm(12.4±2.2ml/beat from 11.5±1.4ml/beat at baseline). There was a 16% increased from baseline in the combination group compare to 7.8% increased in the CR group.
NT proBNP increased 5.6% from 447.5±563.6 pre treatment to 472.7±560.5 post treatment in the combination group. In contrary to this, the CR group demonstrated a marked decrease, around 65% in NT-proBNP levelfrom 950.5±522.9 to 327.5±202.6.
Aims
This study primarily aims to assess the benefits of ECP in the treatment of patients with mild to moderate heart failureor post myocardial infarction undergoing CR in terms of improvement in exercise capacity measured as peak VO2 max and maximum oxygen pulse.
Apart from the primary aim, the study also intends to assess response of heart failure biomarker, NTproBNP in subjects undergoing ECP and CR as compare to the routine CR only.
ECP
A standard ECP treatment course comprises 35 one-hour sessions over a seven-week period [1]. In our study, a shorter treatment course of ECP was chosen to enhance patient compliance and minimize drop outs. The ECP sessions also take placed during the subject’s scheduled CR session.
Study population
The study intend to enrol a total of 16 patients, with symptoms of mild to moderate heart failure and LVEF <40%, or patients with post-acute myocardial infarction in last 3 month, undergoing phase II cardiac rehab at the National Heart Centre of Singapore. These patients were randomised in the ratio of 1:1 to either combination of CR and ECP therapy or the routine CR only. As pregnancy is a contraindication to ECP.
All patients undergoing phase II cardiac rehab were screened for possible enrolment in the study. Patients were approached by the study coordinator, investigators or staff to discuss trial participation. A copy of patient information sheet was provided to the patient to read and understand the study. Patients signed an informed consent if he/she keen to participate in the study. Patient case sheets were reviewed during the screening for verification of ejection fraction. Once a subject meets inclusion and exclusion criteria, he would be enrolled into the study.
Inclusion criteria:
The subject must meet all of the inclusion criteria to participate in this study:
a) Age between 21- 80 years old
b) Enrolment in phase II cardiac rehab
c) Left ventricular systolic dysfunction (LVEF<40% by 2 Decho or Myocardial perfusion Imaging), or post-acute myocardial infarction within the last 3 months.
d) Symptoms of heart failure NYHA Class I – II from ischemic and non-ischemic causes
e) Able to provide informed consent
Exclusion criteria:
Subjects meeting any of the exclusion criteria were excluded from participation:
a) Acute decompensate heart failure, unstable angina pectoris, ST segment elevation. And non-ST elevation MI at the time of enrolment.
b) Heart Failure NYHA Class III - IV
c) Active plan on revascularization or open heart surgery at the time of enrolment.
d) Patients who have undergone any surgical procedure within 6 weeks from start of treatment
e) Cardiac catheterization procedure within 6 weeks from start of treatment
f) Patients in atrial fibrillation or any arrhythmia that could interfere with ECP inflation and deflation triggering
g) Deep vein thrombosis
h) Bleeding disorders
i) Uncorrected symptomatic moderate to severe mitral and aortic stenosis
j) Moderate to severe AR
k) Patients on dual chamber pacemaker/AICD
l) Severe hypertension
m) Presence of local infection or vasculitis of the extremities
n) Women of childbearing potential
For subject who randomised to combination arm (Cardiac Rehab follows by ECP therapy)
Patients received up to 16 one-hour sessions of ECP, following their routine rehab session. This was at least twice a week. Make up session was arranged for the subject in the event that he/she has missed the session but minimum required session of at least once a week in order to be continued in the study.
ECP Therapy
The ECP therapies were conducted using Renew TM NCP-4 Device. Three pressure cuffs similar to blood pressure cuffs were placed at the calves, thighs and hips. The cuffs inflate sequentially upward at the onset of diastole, and deflate rapidly and concurrently before the start of systole (Figure 1). The permissible level of pressure applied to the cuffs for each subject range between 150 mm Hg/ 3 PSI and 300/6 PSI mm Hg
At the start, the skilled operator set a pressure level of 50mmHg/1 PSI on the participant. After 2 minutes, the operator raised the pressure level by 50mmHg/1 PSI to 100/2 PSI mmHg. The participant was asked if the pressure level is comfortable. In a similar manner, 2 minutes later, the operator checked on the participant before increasing the pressure level by an additional 50mmHg/1 PSI. This was continuing up to the level which the participant feels uncomfortable, after which the operator lowered the pressure level by 50mmHg/1 PSI. The pressure level is then recorded and used for subsequent ECP sessions
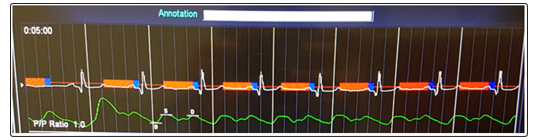
Figure 1: Electrocardiogram gated inflation and deflation of cuffs of the ECP
Note:
Red bar: Inflation of cuffs
Blue bar: Deflation of cuffs
Green waveform: Systolic(S) & diastolic(D)peaks.
For subject randomised to CR arm only
Subjects attended the CR sessions. All underwent baseline cardiopulmonary testing (CPET) and NT-Pro BNP determination within two-weeks prior to initiation of ECP and within one -week after completion of study.
Make up session was arranged for the subject in the event that he/ she has missed the session but minimum required session of at least once a week in order to be continued in the study.
Discontinuation Criteria:
Participants who experience an event (MI, stroke, decompensated heart failure, hospitalization from any cause) and those who cannot tolerate with the session or expresses a desire to discontinue participation were withdrawn from the study.
If duration between two sessions was more than 7 calendar days, patient was considered to have dropped out from the study.
Ethics
The study has obtained approval from the ethics board, the Centralised institutional review board.
Statistical analysis
Statistical analysis was performed using SPSS version 21. The control and intervention arm were compared using independent T test and p value was reported.
Discussion
This pilot study demonstrated that ECP further improves exercise capacity among patients with heart failure or post acute myocardial infarction undergoing cardiac rehabilitation.
Post treatment maximum oxygen consumption (VO2MAX) showed much improvement in both the combination arm and CR arm with the combination arm improving 12% from baseline, and CR arm 5%.Maximal oxygen consumption reflects the cardiorespiratory fitness and is akey factor determining a person cardiovascularstamina during extended exercise.VO2MAX can be applied as a robust predictor of cardiac events, much better thanthe prediction by the usualrecognized risk factors [3]. CR alone is known to improve VO2MAX, the addition of ECP into CR combination confers a greater VO2max in our study. However, in another trial which randomized subjects with mild-to-moderate symptoms of HF to either ECP or without ECP, no disparity found between the intervention and control groups change in peak VO2 [2].
Post treatment maximum oxygen pulsewere also much increased compare to baseline in both the combination arm and CR arm. There was a 16% increased from baseline in the combination group compare to 7.8% increased in the CR group. Maximal oxygen pulse depicts the stroke volume response to exercise. Oxygen pulse risesnearly linearly till the point itreaches the greatestvalue in normal circumstances, conversely in those with impaired left ventricular ejection fraction, oxygen pulse only risesto a small degree with progressive workloads [4]. Studies demonstrated the possible utility of maximum oxygen pulse in forecasting prognosis for individuals with heart failure with reduced ejection fraction [5]. As far as we know, no studies have reported the increase in maximum oxygen pulse with the use of ECP in individuals undergoing CR.
NT proBNP increased 5.6% after treatment in the combination group. In contrary to this, the CR group demonstrated a marked decrease, around 65% in NT-proBNP level post treatment.A slight increased in NT-proBNP level could possibly be due to increase venous return as a result of ECP lower limb compressions in patients with reduced left ventricular ejection fraction. This had led to higher number of decompensated heart failure as a consequence ofrise in preload. This was previously reported in earlier studies [6]. However, in another prospective ECP study performed on ischemic heart disease and chronic Heart failure patients, remarkable improvement in post- intervention BNP levels, NYHA class, left ventricular ejection fraction have been noted [7].
Limitations
Small numbers of participants in this pilot study posed a limitation. With larger numbers, results are likely to reach significance in view of the large treatment effect.
Conclusion
Cardiac Rehabilitation is known to improve exercise capacity among mild to moderate degree heart failure and ischemic heart disease patients. ECP can further enhance maximum oxygen consumption and maximum oxygen pulse in these patients. More studies with larger numbers are needed to prove this benefit of ECP.
Acknowledgments
The support of Renew TM NCP-4 device company.
References
- Arora RR, Chou TM, Jain D, Fleishman B, Crawford L, et al. (1999) The Multicenter Study of Enhanced External Counterpulsation ( MUST-EECP ): Effect of EECP on Exercise- Induced Myocardial Ischemia and Anginal Episodes. J Am Coll Cardiol 33: 1833-1840.
- Feldman AM, Silver MA, Francis GS, Abbottsmith CW, Fleishman BL, et al. (2006) Enhanced External Counterpulsation Improves Exercise Tolerance in Patients With Chronic Heart Failure. J Am Coll Cardiol 48: 1198-1205.
- Laukkanen JA, Kurl S, Salonen R, Rauramaa R, Salonen JT (2004) The predictive value of cardio respiratory fitness for cardiovascular events in men with various risk profiles: a prospective population-based cohort study. Eur Heart J. 25:1428-1437.
- Stringer WW, Hansen JE, Wasserman K (1997) Cardiac output estimated noninvasively from oxygen uptake during exercise. Journal of Applied Physiology 82: 908-912.
- Lavie CJ, Milani R V, Mehra MR (2004) Peak exercise oxygen pulse and prognosis in chronic heart failure. Am J Cardiol. 93:588-593.
- Lawson WE, Kennard ED, Holubkov R, Kelsey SF, Strobeck JE, et al. (2001) Benefit and Safety of Enhanced External Counterpulsation in Treating Coronary Artery Disease Patients with a History of Congestive Heart Failure. Cardiology. 96: 78-84.
- Kozdag G1, Ertas G, Aygün F, Emre E, Kirban A, et al. (2012) Clinical effects of enhanced external counterpulsation treatment in patients with ischemic heart failure. Anatol J Cardiol. 12: 214-221.