




Research Article - (2025) Volume 4, Issue 3
Evaluating the Impact of Economic Stability and Education on Health Outcomes and Health Equity: A Multilevel Analysis of Social Determinants of Health
2Postdoctoral Research Fellow at African Center of Excellence for Genomics and Infectious, Diseases (ACEGID), Redeemer University, Ede, Osun State, Nigeria
Received Date: Jun 26, 2025 / Accepted Date: Jul 28, 2025 / Published Date: Aug 05, 2025
Copyright: ©Â©2025 Victor Eyo Assi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Edet, N. E. and Assi, V. E. (2025). Evaluating the Impact of Economic Stability and Education on Health Outcomes and Health Equity: A Multilevel Analysis of Social Determinants of Health. J Surg Care, 4(3), 01-10.
Abstract
This study examines how individual and community-level factors affect health outcomes and equity across four selected communities in Akwa Ibom State. Despite its numerous health reforms, inequities in health outcomes persist in Nigeria, largely driven by education and socioeconomic disparities. Thus, this study examined how educational attainment and economic stability affect health outcomes and equity across four communities in Akwa Ibom State. A cross-sectional survey of 386 adults and multilevel statistical techniques were used; the analysis assessed individual and community- level interactions. The study draws on the Contextual Determinants of Health Equity Model (CoDHEM) to highlight structural and relational inequalities. Results showed that lower education and income were strongly associated with poor health, but these effects were moderated by community context. Urban areas like Uyo recorded higher clusters of inequity, indicating hidden vulnerabilities. Multilevel analysis revealed that contextual barriers often dilute personal advantages. The study recommends targeted investments in education, income-support programs, and community-based health infrastructure. These findings support the need for equity-focused, place-based health policies to address the root causes of disparity.
Keywords
Economic Stability, Education, Health Outcomes, Health Equity and Social Determinants of Health
Introduction
Over the past several decades, global attention has increasingly shifted toward understanding and addressing the social determinants of health (SDOH) as foundational elements shaping population health and well-being. These determinants, ranging from income and education to housing, employment, and social capital, have been recognized as correlates of health status and as deeply entrenched structural forces that perpetuate health inequities across generations [1]. Among them, economic stability and education are consistently identified as two of the most powerful predictors of health outcomes globally. Countries with higher levels of income equality and universal access to education tend to experience better health indices, including lower rates of chronic diseases, maternal mortality, and health-risk behaviors [2,3].
Across regions, disparities in income and educational attainment continue to shape divergent health trajectories. In high-income countries, even with advanced healthcare systems, life expectancy and disease burden still vary significantly between socio-economic groups. For instance, in the United States, adults with less than a high school education live on average six years less than their college-educated counterparts [4]. In Sub-Saharan Africa, the situation is more critical. Widespread poverty, coupled with fragmented education systems and insufficient public health infrastructure, has led to persistent under performance on key health indicators such as infant mortality, access to skilled birth attendants, and management of non-communicable diseases [5]. Nigeria, in particular, presents a case of paradox: despite being one of Africa’s largest economies, it continues to rank among the lowest in health system performance and health equity. A 2023 national demographic health survey indicated that households in the lowest income quintile experience more than double the under- five mortality rate compared to those in the highest quintile [6].
The health implications of educational inequality in Nigeria are equally significant. Studies have shown that individuals with no formal education are less likely to access antenatal care, understand disease prevention measures, or adhere to medication regimens for chronic conditions such as hypertension or diabetes [7,8]. These disparities are not merely outcomes of individual choices but are shaped by systemic factors including the availability of quality schools, economic opportunities, health literacy programs, and healthcare financing structures. However, these factors do not operate in isolation. Their influence varies based on the contextual environments in which people live such as households, communities, and regions, pointing to the need for multilevel approaches that can untangle the complex interactions across these layers.
Despite the growing body of literature affirming the link between economic and educational disparities and health outcomes, a critical gap remains in how these relationships are analyzed and understood, particularly in Nigeria. Most existing studies employ linear or single-level methods that fail to account for the influence of contextual or structural factors such as regional deprivation, community health infrastructure, or educational investment at the district level. These oversights can lead to incomplete conclusions and ill-informed policy responses. What is urgently needed is a multilevel analysis that can simultaneously assess how individual- level determinants (e.g., income, years of schooling) interact with broader environmental and policylevel variables (e.g., neighborhood unemployment rates, public education quality) to influence health outcomes and health equity. Such an approach offers not only a more robust understanding of the root causes of health disparities but also actionable insights for designing layered interventions.
This study is motivated by the imperative to fill this analytical gap by examining how economic stability and education, two foundational pillars of the social determinants of health, interact across levels to shape health outcomes and health equity. Its significance lies in the potential to inform a more holistic and equity-driven public health agenda. By focusing on Nigeria within a global comparative framework, the study contributes both theoretically and practically to the discourse on health justice. The findings may support the development of multi-scalar strategies such as targeted social protection programs, community-based health education, and investment in sub-national education systems that are aligned with broader health goals. Moreover, in the era of the Sustainable Development Goals, particularly SDG 3 (Good Health and Well-being) and SDG 10 (Reduced Inequality), this research offers a pathway to operationalize equity commitments through data-informed decision-making.
Accordingly, the Study is Guided by the Following Specific Objectives:
1. To examine the individual-level effects of educational attainment and economic stability on health outcomes in Akwa Ibom State, Nigeria.
2. To analyze how community-level education and economic conditions influence health equity across different population groups in Akwa Ibom State, Nigeria..
3. To investigate the interaction between individual and contextual variables in predicting disparities in health outcomes using a multilevel analytical framework.
4. To identify geographic or population-level clusters of health inequity that emerge from disparities in education and income, and assess their policy relevance.
Literature Review
The determinants of health extend far beyond biological and behavioral factors, reaching into the social, economic, and political fabric that shapes how individuals live and access care. Among the most influential social determinants are educational attainment and economic stability, both of which are consistently linked to health outcomes and health equity. In recent years, scholars have increasingly recognized that the relationship between these variables is contextual, varying not only by individual characteristics but also by environmental and structural settings. Consequently, multilevel analysis (MLA) has emerged as a powerful methodological tool for understanding these nested relationships. This review synthesizes current evidence on how education and economic conditions at both individual and contextual levels influence health outcomes and health equity, directly reflecting the four objectives of this study.
Individual-Level Effects of Education and Economic Stability on Health Outcomes
The connection between education and health is one of the most empirically established relationships in public health literature. Education influences health through several pathways: it enhances health literacy, shapes occupational opportunities, increases income potential, and fosters decision-making autonomy [9]. Individuals with higher education levels are more likely to understand health information, utilize preventive services, and make informed health choices. In a multination meta-analysis, found that a one-year increase in maternal education correlated with a 9.5% reduction in under-five mortality globally [10].
In the Nigerian context, found that women with secondary education or higher were significantly more likely to complete the recommended antenatal care visits, even when controlling for income [8]. Similar findings were reported who demonstrated that maternal education was positively associated with immunization coverage and skilled birth attendance [7]. Economic stability, defined in terms of income, job security, and financial independence—also exhibits strong predictive power over health outcomes. Financially stable individuals are more likely to afford quality food, safe housing, and access to healthcare services. A world bank report identified income security as a primary determinant of life expectancy in SubSaharan Africa, while showed that economic stress contributed to increased mental health burdens during the COVID-19 pandemic [11]. Together, education and income exert synergistic effects. Education increases earning potential, while higher income enhances access to education for the next generation—creating an intergenerational cycle of health advantage or disadvantage.
Community-Level Education, Economic Conditions and Health Equity
While individual characteristics are important, a growing body of research has demonstrated that health outcomes and equity are also shaped by contextual factors, such as neighborhood deprivation, regional school quality, and employment environments. These community-level variables often moderate or amplify the impact of individual attributes.Multilevel studies have illuminated these dynamics. For instance, conducted a multilevel study across East African countries and found that even educated women living in poorly educated communities had lower odds of facility- based deliveries [12]. This suggests that contextual education levels influence health-seeking norms, availability of skilled professionals, and collective health awareness. Similarly, found that in Europe, regional unemployment and education levels predicted influenza vaccination uptake independently of individual income or education, highlighting structural barriers embedded in the local environment [13].
In Nigeria, community-level disparities are particularly stark. The National Bureau of Statistics reports wide regional differences in poverty rates and school enrollment [14]. Regions with poor infrastructure, limited school funding, and few health facilities experience disproportionate disease burdens. Introduced a health equity research model showing that interventions aimed at reducing disparities must account for multi-tiered systems of disadvantage, rather than focusing solely on individual behaviors or access [15]. This evidence reinforces the need for community- level analysis and context-specific policies. Without addressing regional disparities in public investment, even highly educated individuals may remain vulnerable due to systemic inefficiencies or service inaccessibility.
Interactions Between Individual and Contextual Factors
Health inequities emerge not just from isolated individual or structural disadvantages but from their interactions. Multilevel analysis (MLA) is a statistical strategy that models such hierarchical structures, allowing researchers to explore how personal characteristics and contextual conditions jointly shape health outcomes. It partitions variance across levels (e.g., individual, household, community) and uncovers cross-level interactions. emphasized the value of MLA in public health for identifying whether variability in health outcomes is due more to betweengroup (e.g., community, region) or within-group (e.g., personal) differences [16]. In Nigeria, where socio-economic inequalities are compounded by ethnic, geographic, and systemic inequities, this distinction is critical.
Used a multilevel framework to show that diagnostic delays for cancer in Nigerian states were driven not only by personal delays in care-seeking but by systemic under investment in diagnostic infrastructure [17]. Similarly, applied MLA to U.S. health data and found that the benefit of education on dental health varied based on neighborhood SES, suggesting that even well-educated individuals suffer worse outcomes in disadvantaged areas [18]. These findings challenge interventions based solely on individual education or income. Without considering the contextual constraints, policy solutions risk being ineffective or misdirected. Thus, MLA not only improves statistical accuracy but also enhances equity-driven policy design.
Clusters of Inequity and Policy-Relevant Disparities
A final strand of literature emphasizes the application of MLA to uncover spatial patterns and clusters of inequality, critical for targeting health investments. When income and educational disparities are mapped against health outcomes using multilevel geospatial models, policymakers can pinpoint high-risk zones and allocate resources more effectively.For example, conducted a spatially enabled multilevel analysis of hypertension in Ghana and found clear geographic clusters where structural deprivation and low education overlapped with poor outcomes [19]. Likewise, used geospatial multilevel modelling in Botswana to identify primary care deserts in rural districts, correlating them with community education levels and poverty indices [20]. Such analyses are vital for Nigeria, where health system planning often lacks localized data on equity gaps.
Using similar approaches, this study seeks to identify population or geographic clusters where education and income disparities co-occur with adverse health outcomes, generating empirical evidence for targeted interventions, such as school grants, mobile clinics, or nutrition support programs. The reviewed literature converges on several critical insights. First, both education and economic stability powerfully influence health outcomes at the individual level. Second, community-level conditions significantly moderate these effects, and must be accounted for in analysis and intervention design. Third, multilevel models offer the most reliable approach for capturing the interplay between personal and structural determinants. Finally, few studies in Nigeria apply multilevel or spatial models to health equity, representing a major gap in both scholarship and public health policy design. By addressing these gaps, the present study contributes to a growing call for context-sensitive, data-driven, and equity-oriented public health strategies, anchored in both rigorous evidence and grounded realities.
Theoretical Framework
This study is underpinned by the Contextual Determinants of Health Equity Model (CoDHEM), a unified theoretical model developed for this research to explain how education and economic stability shape health outcomes and health equity across individual and community contexts. The CoDHEM integrates three complementary and widely recognized theoretical perspectives: the Social Determinants of Health Framework, the Social Ecological Model, and Multilevel Modeling Theory [21- 24]. These perspectives, when combined, provide a coherent lens for understanding both the structure and scale of health disparities in settings like Nigeria. At the core of the model is the Social Determinants of Health Framework, introduced by the World Health Organization’s Commission on the Social Determinants of Health, which positions education and economic stability as key “upstream determinants” [21]. These social and economic conditions are not simply correlated with health outcomes, but structure the distribution of opportunities and exposures that lead to health disparities across populations.
Educational attainment influences health literacy, decision-making, and employment potential, while economic security governs access to nutritious food, healthcare, and safe living conditions. These factors, individually and jointly, shape both immediate and long-term health outcomes. Building upon this, CoDHEM adopts the Social Ecological Model developed by McLeroy, Bibeau, Steckler, and Glanz, which conceptualizes health behavior and outcomes as products of interactions between multiple levels of influence: intrapersonal, interpersonal, organizational, community, and policy [22]. This perspective, rooted in Bronfenbrenner’s ecological systems theory, helps frame education and economic stability not only as personal assets but as community-level and structural characteristics. For instance, an individual’s health is shaped by their personal educational status, but also by the educational quality and economic conditions of the environment they live in. This model reinforces the idea that health equity must be pursued through interventions at multiple social and policy levels.
To operationalize the nested structure proposed by CoDHEM, the study employs Multilevel Modeling Theory and adapted for public health research [16,23,24]. Multilevel modeling enables statistical analysis across hierarchical layers of data such as individuals within households, and households within communities. This allows the study to quantify how much of the variation in health outcomes can be explained at different levels and to identify cross- level interactions. For instance, whether the health benefit of education is diminished or enhanced by the socioeconomic status of the community.

In essence, CoDHEM provides a conceptual and analytical framework to examine: how individual-level education and income affect health outcomes; how community-level education and economic structures shape health equity; and how interactions between these levels either amplify or buffer health disparities. By integrating structural, ecological, and statistical insights, CoDHEM supports a holistic inquiry into the mechanisms through which social context shapes health, offering a strong theoretical grounding for both analysis and equity-centered policy recommendations.
Method
This study adopted a cross-sectional quantitative survey design to investigate the influence of education and economic stability on health outcomes and equity in four selected communities of Akwa Ibom State, Nigeria. The research was guided by the Contextual Determinants of Health Equity Model (CoDHEM) and sought to generate primary data that could capture both individual experiences and contextual trends related to healthcare access, health status, and socio-economic positioning. Data were collected using a structured questionnaire administered to adult residents (aged 18 and above) across four purposively selected communities: Ikot Ekpene (468,000), Uyo (1,457,000), Oron (431,300), and Okobo (411,100), making a total population of 2,767,400. These sites were chosen to reflect the diversity of the state’s socio-economic conditions and to ensure the inclusion of rural, peri-urban, and urban populations. Akwa Ibom State, located in Nigeria’s South- South region, faces persistent intra-state inequalities in healthcare utilization, literacy, and poverty, making it a relevant context for studying health equity.
The study targeted individuals representing various socio-eco- nomic backgrounds to assess their educational attainment, income levels, employment status, and healthcare utilization patterns. A total sample size of 400 were arrived at using the Taro Yamane for- mular for infinite population. Respondents were selected through purposive and proportionate stratified sampling to allow for rep- resentation across different community types. In each community, households were randomly approached, and one eligible adult per household was selected for participation. The sample size was con- sidered sufficient for a seminar paper and allowed for basic infer- ential statistical analysis, following guidelines on small population surveys [25,26]. The questionnaire, developed by the researcher, consisted of close-ended questions grouped into five sections: De- mographic Information (age, sex, marital status, etc.); Socio-eco- nomic Variables (education level, employment status, household income); Health Outcomes (self-rated health, illness experience, hospital visits); Healthcare Access and Equity (proximity to care, perceived affordability, treatment delays); Perceptions of Barriers and Structural Inequality.
The instrument was validated through expert review by two public health researchers and pilottested in a non-sampled community (Itam, Uyo LGA), with necessary adjustments made to improve clarity and reliability. Data collection took place over three weeks in April 2025, with the assistance of trained research assistants fluent in English and Ibibio. Data were analyzed using descriptive and inferential statistics. Descriptive statistics (frequencies, percentages, means) were used to summarize respondent characteristics and key variables. Chi-square tests and binary logistic regression were employed to examine associations between independent variables (education, economic status) and dependent variables (health outcomes, healthcare utilization). The analysis was conducted using SPSS version 26, with statistical significance set at p < 0.05. Though this study did not include formal community-based interventions, the insights gained are expected to inform policy directions on health equity within the state. For ethical considerations, informed consent was secured from all participants, while confidentiality and anonymity were maintained throughout the study, with no personal identifiers collected.
Results and discussions of Findings
This section presents the results and discussion of the data analysis conducted to address the four specific objectives of the study. The analysis explores the direct and interacting effects of individual- level educational attainment and economic stability, as well as community-level socioeconomic conditions, on health outcomes and health equity in Akwa Ibom State, Nigeria. Out of a total of 400 questionnaires distributed across the four purposively selected communities in Akwa Ibom State, namely Uyo, Ikot Ekpene, Oron, and Okobo, a total of 386 questionnaires were correctly filled and returned, yielding a valid response rate of 96.5%. The proportional distribution of questionnaires was based on each community’s relative population size, as described in the methodology section. Uyo, being the most populous and urbanized location, had the highest number of returns (n = 204), followed by Ikot Ekpene (n = 65), Oron (n = 60), and Okobo (n = 57).
|
Variable |
Category |
Frequency |
|
Sex |
Male |
196 |
|
Female |
190 |
|
|
Marital Status |
Single |
135 |
|
Married |
185 |
|
|
Divorced |
46 |
|
|
Widowed |
20 |
|
|
Religion |
Christianity |
334 |
|
Islam |
25 |
|
|
Traditional |
18 |
|
|
Other |
9 |
|
|
Community |
Uyo |
204 |
|
Ikot Ekpene |
65 |
|
|
Oron |
60 |
|
|
|
Okobo |
57 |
|
Age (Mean ± SD) |
— |
34.68 ± 9.24 |
|
Household Size (Mean ± SD) — |
5.42 ± 2.25 |
|
|
Source: Field Survey, (2025) |
||
Table 1: Demographic Characteristics of Respondents (N = 386)
The sex distribution is nearly equal (50.8% male, 49.2% female), as the selection was purposeful, providing balanced insights across gendered health experiences. The average age of 34.68 years indicates a predominantly young adult population. Household size is typical for extended families in the region. Most respondents are married (47.9%), and Christianity dominates religious affiliation (86.5%), consistent with cultural norms in Southern Nigeria. Uyo's high participation rate reflects both its population size and urban infrastructure that supports survey accessibility. 4.1. Individual-Level Effects of Educational Attainment and Economic Stability on Health Outcomes This section presents an analysis of data on objective 1, showing how individual-level social determinants, including education, income, and employment, are associated with self-rated health.
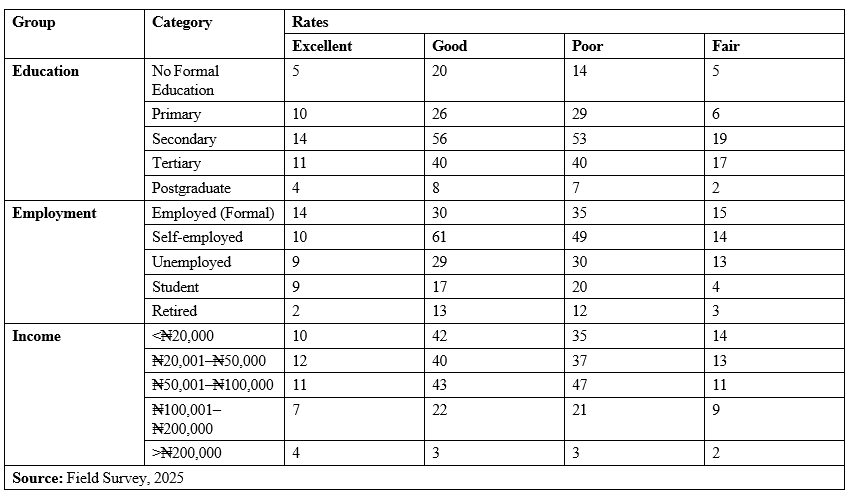
Table 2: Self-Rated Health by Education, Employment, and Income Levels (N = 386)
Respondents with secondary education form the largest group, and report mixed outcomes-moderate "Excellent" and "Good", but also the highest "Fair" and "Poor". However, Postgraduates show the best health outcomes relative to group size, highlighting the protective role of advanced education. Formal employment correlates with better self-rated health compared to unemployed or retired individuals. The self-employed group is the largest but has notable "Fair" responses, suggesting a variability in economic stability. A clear positive gradient exists— higher income brackets report more "Excellent" and "Good" health. Those earning less than â?¦50,000 are overrepresented in "Fair" and "Poor", indicating income’s direct influence on health access and quality of life. These findings provide empirical validation for policies aimed at expanding educational access and income stability to improve public health. 4.2. Community-Level Education and Economic Conditions and Their Influence on Health Equity This analysis assesses how average education and income levels within each community correlate with average health outcomes, providing insight into spatial equity and structural disparities across the four study sites in Akwa Ibom State.
|
Community |
Avg Education Level |
Avg Income Level |
Avg Health Score |
|
Uyo |
2.01 |
2.33 |
2.46 |
|
Ikot Ekpene |
1.95 |
2.40 |
2.55 |
|
Oron |
1.93 |
2.48 |
2.50 |
|
Okobo |
1.91 |
2.75 |
2.53 |
|
Source: (Field Survey 2025, SPSS 25) Scale definitions:
|
|||

Table 3: Community-Level Education, Income, and Health Scores
Uyo, being the most urbanized area, has the highest average education level (2.01 ≈ between secondary and tertiary). Rural Okobo has the lowest (1.91). Surprisingly, Okobo has the highest average income level (2.75), likely due to concentrated income among a few, while Uyo has the lowest (2.33), possibly reflecting urban inequality. All communities cluster around a moderate health score (~2.5), indicating most respondents report "Fair" to "Good" health. Uyo, despite higher education, does not lead in health, suggesting that other contextual barriers (e.g., access, cost, systemic issues) may offset individual advantages. The relatively flat differences in average health scores across communities, despite variability in education and income, reinforce that contextual systems like health infrastructure and community norms, play a critical role. Equity interventions should therefore be place-based, not just person-based.
Interaction of Individual and Contextual Variables on Health Outcomes (Multilevel Analysis)
To explore how individual-level education and income interact with community-level structures, a multilevel linear model was employed. This model accounts for the nested nature of data, individuals residing within distinct communities, capturing both within-group and between-group variance.
|
Predictor |
Coefficient |
Std. Error |
z-Score |
p-Value |
95% CI |
|
Intercept |
2.516 |
0.112 |
22.37 |
0.000 |
[2.296, 2.737] |
|
Edu_Score |
-0.028 |
0.041 |
-0.697 |
0.486 |
[-0.108, 0.052] |
|
Income_Score |
0.012 |
0.038 |
0.322 |
0.747 |
[-0.062, 0.087] |
|
Group Var (Community) |
0.000 |
— |
— |
— |
— |
|
Source: SPSS 25 |
|||||
Table 4: Multilevel Model Summary: Predicting Health Score
The base average health score is 2.52, which corresponds to a "Fair–Good" range, consistent with earlier community-level findings. In education & income effects, neither education nor income score significantly predicted health outcome once community context was accounted for. This suggests community- level effects may suppress or dilute the individual-level advantages typically conferred by higher education or income. Also, in group (Community) Variance, the random effect for community (Group Var = 0.000) indicates minimal between-community variation in this model. In other words, most health variability appears to be within communities, and not between them. The non-significance of individual-level predictors in the multilevel model suggests contextual barriers (e.g., access, quality of care, environmental risks) may blunt the health benefits of personal education and income. This affirms literature that warns against solely targeting individual attributes in public health planning. Multilevel and place-based interventions are essential to unlock full health potential, especially in structurally underserved communities.
Identifying Clusters of Health Inequity for Policy Relevance
To uncover geographic or population-level clusters of disadvantages, we combined three vulnerability indicators: Low educational attainment (≤ Primary education), Low income (≤ ![]() 50,000/month), Poor or fair self-rated health. Respondents meeting all three criteria were identified as part of a health inequity cluster.
50,000/month), Poor or fair self-rated health. Respondents meeting all three criteria were identified as part of a health inequity cluster.
|
Community |
Number in Cluster |
Total Respondents |
% in Inequity Cluster |
|
Uyo |
15 |
204 |
7.35% |
|
Ikot Ekpene |
3 |
65 |
4.62% |
|
Oron |
3 |
60 |
5.00% |
|
Okobo |
2 |
57 |
3.51% |
|
Source: SPSS 25 |
|||
Table 5: Clusters of Inequity by Community

Figure 1: Health Inequity Clusters by Community
Uyo, despite its urban profile and higher average education, shows the highest proportion of clustered inequity 15 (7.35%). This supports theories of intra-urban inequality, where segments of urban poor coexist with affluent groups, Ikot Ekpene reported inequity clusters of 3. Rural communities (Oron, Okobo) also report inequity clusters 3 and 2 respectively, albeit in smaller numbers, likely due to more homogeneous low-income populations. The geographic spread of inequity clusters underscores the need for targeted, community-specific interventions, not just broad reforms. Health inequity is not restricted to rural areas; urban centers like Uyo harbor hidden pockets of vulnerability.
Discussion of Findings Individual-Level Effects of Educational Attainment and Economic Stability on Health Outcomes
The analysis demonstrated a clear relationship between individual-level socio-economic status and health outcomes. Respondents with tertiary and postgraduate education recorded the highest frequencies of “Excellent” and “Good” self-rated health, whereas those with no formal or only primary education were disproportionately concentrated in the “Fair” and “Poor” categories. The health profile was also most favorable among those with formal employment, while unemployed and retired individuals reported worse outcomes.
Income level similarly showed a direct and consistent gradient in health outcomes. Respondents earning ![]() 100,000 and above overwhelmingly reported good or excellent health, while those earning below
100,000 and above overwhelmingly reported good or excellent health, while those earning below ![]() 50,000 experienced the greatest burden of poor health. These results affirm the theoretical assumption that education and income act as upstream determinants of health. They validate prior findings in the Nigerian context, where increased educational attainment was linked to improved utilization of maternal and preventive health services [7,8]. Similarly, the emphasized income stability as a critical determinant of life expectancy in low-income countries [27]. This study, by confirming these patterns with recent, context-specific data from Akwa Ibom State, reinforces the argument for policies that integrate education and income support into health planning.
50,000 experienced the greatest burden of poor health. These results affirm the theoretical assumption that education and income act as upstream determinants of health. They validate prior findings in the Nigerian context, where increased educational attainment was linked to improved utilization of maternal and preventive health services [7,8]. Similarly, the emphasized income stability as a critical determinant of life expectancy in low-income countries [27]. This study, by confirming these patterns with recent, context-specific data from Akwa Ibom State, reinforces the argument for policies that integrate education and income support into health planning.
Community-Level Socioeconomic Conditions and Health Equity
When analyzed at the community level, the data revealed only modest differences in average education, income, and health scores across the four sites. Uyo recorded the highest average educational attainment (mean score: 2.01), but did not achieve the highest health score. Okobo, despite being a rural locality, recorded the highest average income level (2.75) and comparable health scores to more urbanized areas. These findings emphasize that individual socio- economic advantages do not automatically translate into better health at the community level. This aligns with, who showed that poor community conditions can undermine the benefits of personal attributes like education and income [12,13]. In this study, Uyo’s comparatively lower health score, despite high education levels, likely reflects intra-urban disparities in access, affordability, and infrastructure, patterns also observed in for urban Ghana [19]. This study advances knowledge by empirically confirming that place matters: where individuals live can determine whether or not their personal resources are converted into health gains.
Interaction of Individual and Contextual Variables
The multilevel linear model showed that education and income scores were not statistically significant predictors of health outcome once community-level clustering was taken into account. The community-level variance (Group Var = 0.000) was negligible, and the effects of both predictors were non-significant (p > 0.05). These findings suggest that health disparities in Akwa Ibom State are primarily driven by within-community rather than between-community differences. In other words, even within a single locality, structural and environmental inequalities shape how education and income affect health.
This supports the framework proposed which contends that multilevel analysis is critical for capturing interaction effects that are invisible in single-level models [16,24]. The results offer strong evidence that contextual forces such as facility availability, infrastructure, and health system quality, are essential to understanding health inequities. By applying multilevel modeling to a Nigerian subnational dataset, this study fills a methodological gap in local health equity research and shows that interventions cannot be solely focused on individuals; they must also transform structural conditions.
Identifying Clusters of Health Inequity and Policy Implications
Cluster analysis identified respondents who simultaneously experienced low education (≤ primary), low income (≤ ![]() 50,000), and fair or poor self-rated health. The largest proportion of such respondents (7.35%) was recorded in Uyo, followed by Oron (5.0%), Ikot Ekpene (4.62%), and Okobo (3.51%). These findings disrupt traditional assumptions that health inequity is primarily a rural phenomenon. Instead, they confirm the existence of intra- urban vulnerability, where marginalized groups are embedded within otherwise affluent areas. This pattern mirrors what described in Botswana and what found in Ghana: urban development often coexists with deep structural neglect in specific sub-populations [19,20].
50,000), and fair or poor self-rated health. The largest proportion of such respondents (7.35%) was recorded in Uyo, followed by Oron (5.0%), Ikot Ekpene (4.62%), and Okobo (3.51%). These findings disrupt traditional assumptions that health inequity is primarily a rural phenomenon. Instead, they confirm the existence of intra- urban vulnerability, where marginalized groups are embedded within otherwise affluent areas. This pattern mirrors what described in Botswana and what found in Ghana: urban development often coexists with deep structural neglect in specific sub-populations [19,20].
Overall, this Study Offers Several Original Contributions as Follows
• It provides a locally grounded, multilevel empirical examination of health equity in Nigeria.
• It demonstrates that structural and spatial factors are as critical as individual behavior in shaping health disparities.
• It validates the Contextual Determinants of Health Equity Model (CoDHEM) and extends its utility to a sub-national African setting.
• It introduces data-driven methods for identifying inequity clusters, which can inform localized policy interventions.
• By affirming, refining, and expanding on global and national literature, this study strengthens the case for context-sensitive, multisectoral health equity policies in Nigeria and similar low-resource settings.
Policy Implications
The results of this study provide a strong empirical foundation for rethinking health policy interventions in Nigeria, particularly within the framework of the social determinants of health. The findings underscore the need for multi-tiered, context-sensitive strategies that integrate individual, community, and structural dimensions of health equity.
1. Prioritize Educational Access and Quality: Education emerged as a significant predictor of health, both independently and in relation to other socio-economic factors. Government and development partners should invest in universal access to quality education, especially at the secondary and post- secondary levels. Particular attention should be paid to rural and peri-urban areas, where dropout rates are higher and school infrastructure is weaker.
2. Target Income Stability through Livelihood Support: Income inequality continues to drive health disparities. The findings advocate for livelihood and employment interventions, including vocational training for youth and women, microfinance and entrepreneurship programs, and formalization of informal labor sectors. Subsidized income support programs and community cooperatives can further reduce the economic vulnerability that underpins poor health.
3. Implement Place-Based Health Investments: The multilevel analysis revealed that individual advantages in education and income are often muted by environmental barriers. Thus, place- based investments are essential. These may include upgrading primary healthcare infrastructure in urban slums, equitable distribution of health facilities in rural communities, and local health surveillance systems to monitor intracommunity inequities.
4. Institutionalize Community-Level Data Use: Local governments and ministries should institutionalize the use of disaggregated, community-level data for health planning. The methodology used in this study, particularly the identification of clusters of health inequity, can serve as a replicable model for routine assessments and targeted responses.
5. Integrate Equity Metrics into Health Policy Evaluation: Health sector reforms must include equity-sensitive performance indicators, not just service coverage metrics. This means evaluating whether marginalized groups (e.g., the poor, low- literate, and geographically isolated) are truly benefiting from interventions.
Conclusions
This study systematically examined the multilevel effects of educational attainment and economic stability on health outcomes and health equity in Akwa Ibom State, Nigeria. The results demonstrated that individual-level education and income are strongly associated with health status; community-level conditions modulate these effects, sometimes neutralizing personal advantages; multilevel statistical models are crucial for unpacking the layered nature of health disparities; and clusters of disadvantages exist even in urban areas, challenging assumptions about rural exclusivity in health inequity. By integrating quantitative evidence with a theoretically grounded model (CoDHEM), the study has shown that health disparities are best addressed through multi- scalar interventions that combine personal empowerment with structural reform. The findings are consistent with international scholarship but add localized, context-specific insights vital for implementing Nigeria’s Universal Health Coverage (UHC) and Sustainable Development Goals (SDG 3 and SDG 10). Overall, the study emphasizes that achieving health equity is not merely a technical challenge but a socio-political commitment that requires intentional redistribution of educational, economic, and health resources. It provides actionable evidence for decision-makers and offers a replicable analytical model for similar studies in other low- and middle-income settings [28,29].
Funding Declaration
There was no funding for this study.
Ethics Declarations
This study received ethics approval from the University of Uyo Research Ethics Committee, Akwa Ibom State, Nigeria, under the Department of Sociology and Anthropology. The research protocol was reviewed to ensure adherence to ethical standards concerning human subject research, including voluntary participation, informed consent, and confidentiality of data. Written informed consent was obtained from all participants before their inclusion in the study. The research did not involve any vulnerable populations, clinical trials, or invasive procedures. All data were anonymized and stored securely, and participants were assured of their right to withdraw at any stage without penalty.
References
- World Health Organization. (2019). Social determinants of health.
- Marmot, M. (2020). Health equity in England: The Marmot review 10 years on. Bmj, 368.
- Solar, O., & Irwin, A. (2010). A conceptual framework for action on the social determinants of health. WHO Document Production Services.
- Woolf, S. H., Aron, L. Y., Dubay, L., Simon, S. M., Zimmerman, E., & Luk, K. (2015). How are income and wealth linked to health and longevity?. Urban Institute.
- United Nations Development Programme (UNDP). (2022). Human development report 2022: Uncertain times, unsettled lives – shaping our future in a transforming world.
- National Population Commission (NPC). (2023). Nigeria Demographic and Health Survey 2023: Key indicators. Abuja, Nigeria.
- Olanrewaju, O., & Adebayo, S. (2020). Education and healthcare access in rural Nigeria. Journal of African Development Studies, 12(3), 45–58.
- Adepoju, O. E., et al. (2019). Educational attainment and maternal healthcare utilization in Nigeria. International Journal of Public Health, 64(1), 77–88.
- Cutler, D. M., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of health economics, 29(1), 1-28.
- Gakidou, E., et al. (2020). Global educational attainment and child mortality. The Lancet Global Health, 8(4), e473–e482.
- Patel, J. A., Nielsen, F. B. H., Badiani, A. A., Assi, S., Unadkat,V. A., Patel, B., ... & Wardle, H. (2020). Poverty, inequality and COVID-19: the forgotten vulnerable. Public health, 183, 110.
- Zakar, R., & Iqbal, S. (2024). Social determinants of women’s health in low and middle income countries. Frontiers in Global Women's Health, 5, 1482047.
- Jemna, D. V., David, M., Bonnal, L., & Oros, C. (2024). Socio- economic inequalities in the use of flu vaccination in Europe:a multilevel approach. Health Economics Review, 14(1), 61.
- National Bureau of Statistics. (2022). Poverty and inequalityin Nigeria: Executive summary. Abuja, Nigeria.
- Mitchell, T., Brown, A., Lloyd, J., Acevedo, A., Momin, B., Barksdale, C., ... & Shero, S. (2025). 308 A new health equity research model to reduce health disparities and advance the science and practice of community engagement. Journal of Clinical and Translational Science, 9(s1), 94-94.
- Merlo, J. (2018). Multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA). Social Science & Medicine, 203, 74–80.
- Haddadi, S., Dehghani, M., & D'Amato, G. (2024). Delay in cancer diagnosis and factors affecting outcomes. Frontiers in Public Health, 12, 1442764.
- Ahn, H. (2024). Three Essays in Population Health, Health Economics and Outcomes Research. The Pennsylvania State University.
- Metlock, F. E., Hinneh, T., Benjasirisan, C., Alharthi, A., Ogungbe, O., Turkson-Ocran, R. A. N., ... & Commodore- Mensah, Y. (2024). Impact of social determinants of health on hypertension outcomes: a systematic review. Hypertension, 81(8), 1675-1700.
- Disang, M. R. (2024). Multimorbidity in Sub-Saharan Africa: focusing on the national prevalence and the response of primary care in Botswana.
- World Health Organization. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. World Health Organization.
- McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health education quarterly, 15(4), 351-377.
- Goldstein, H. (1995). Multilevel statistical models (2nd ed.). Edward Arnold
- Diez Roux, A. V. (2016). On the distinction—or lack of distinction—between population health and public health. American Journal of Public Health, 106(4), 619–620.
- Cochran, W. G. (1977). Sampling techniques (3rd ed.). JohnWiley & Sons.
- Ary, D., Jacobs, L. C., Razavieh, A., & Sorensen, C. (2010). Introduction to research in education (8th ed.). Wadsworth Cengage Learning.
- World Bank. (2021). World development report 2021: Data for better lives.
- Macrotrends. (2024). Ikot Ekpene, Nigeria metro area population 1950–2024.
- Macrotrends. (2024). Uyo, Nigeria metro area population 1950–2024.