
World Journal of Otolaryngology Research(WJOR)


Case Report - (2026) Volume 3, Issue 1
Esthesioneuroblastoma Presenting as a Large Cervicofacial Mass: A Case Report and Review of the Literature
Received Date: Jan 09, 2026 / Accepted Date: Apr 07, 2026 / Published Date: May 22, 2026
Copyright: ©2026 Ichraq Horrane, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Horrane, I., Berdi, Z., Bencheikh, R., Benbouzid, A., Essakalli, L., et al. (2026). Esthesioneuroblastoma Presenting as a Large Cervicofacial Mass: A Case Report and Review of the Literature. World J Otolaryngol Res, 3(1), 01-07.
Abstract
Introduction and Importance: Esthesioneuroblastoma (ENB) is a rare malignant tumor arising from the olfactory neuroepithelium, accounting for a small proportion of sinonasal cancers. Its clinical presentation is often nonspecific, and advanced disease may manifest with orbital, intracranial, or cervical involvement, posing significant diagnostic and therapeutic challenges.
Case Presentation: We report the case of a 31-year-old man presenting with progressive nasal obstruction, epistaxis, anosmia, and headaches, followed by the rapid development of a large cervicofacial mass. Imaging revealed an aggressive sinonasal tumor with orbital, intracranial, and cervical lymph node involvement. Histopathological and immunohistochemical analysis confirmed a low-grade esthesioneuroblastoma (Hyams I–II), classified as Kadish stage C. Due to unresectability, the patient was treated with combined chemoradiotherapy.
Clinical Discussion: Esthesioneuroblastoma is characterized by heterogeneous clinical behavior and a high propensity for local extension and recurrence. Advanced-stage disease often requires multimodal treatment. Imaging and histopathological grading are essential for staging, prognostic assessment, and therapeutic decision-making.
Conclusion: This case highlights an unusual cervicofacial presentation of advanced esthesioneuroblastoma and underscores the importance of early diagnosis, comprehensive imaging, and multidisciplinary management to improve outcomes in this rare malignancy.
Keywords
Esthesioneuroblastoma, Olfactory neuroblastoma, Cervicofacial mass, Sinonasal malignancy, Kadish staging, Case report.
Introduction
Esthesioneuroblastoma (ENB) is a rare neuroectodermal neoplasm derived from the olfactory epithelium of the superior nasal cavity. Since its first description by Berger in 1924, ENB has represented approximately 3–6% of sinonasal malignancies and affects patients of all ages, with a bimodal peak in the second and sixth decades of life [1,2].
Typical manifestations include nasal obstruction (70–80%), epistaxis, anosmia, and headaches [3]. However, advanced tumors may invade the orbit, skull base, paranasal sinuses, or cervical lymph nodes. Cervical lymph node metastasis occurs in 5–10% at presentation and up to 20–25% during disease evolution [4,5]. Distant metastases remain uncommon but have been reported in the lungs, bones, spinal cord, and brain [6].
Diagnostic confirmation relies on histopathology and immunohistochemistry, while CT and MRI remain essential to assess local extent and guide treatment planning. Several staging systems exist, including the Kadish classification, the Dulguerov TNM system, and the Hyams histopathological grading, all offering prognostic insights [7-9].
Current standard management involves multimodal therapy, combining surgery, radiotherapy, and—more recently— chemotherapy, particularly in advanced or unresectable cases [10-12].
We report an uncommon presentation of ENB revealed by a voluminous cervicofacial mass, highlighting the diagnostic and therapeutic challenges inherent to advanced stages of the disease. This manuscript was prepared in accordance with the TITAN Guidelines 2025 governing the transparent declaration and responsible use of artificial intelligence in scientific writing [24]
Case Report
A 31-year-old male with no significant medical history presented with 6 months of headaches, progressive left-sided nasal obstruction, intermittent epistaxis, and anosmia evolving over 4 months. During the preceding 15 days, the patient noted the rapid development of a large left cervicofacial mass, prompting urgent consultation.
Clinical Examination
Nasal endoscopy revealed a gray-pink, friable mass completely filling the right nasal cavity. The oropharynx was normal. An obvious left cervicofacial mass was palpable, firm, mobile but tender, and progressively enlarging. No cranial nerve deficit was noted. (Figure 1)

Figure 1: Clinical Figure showing the left cervicofacial mass
Imaging Findings
A contrast-enhanced cervicofacial CT scan revealed:
• A homogeneous soft-tissue mass centered on the nasal cavities
• Extension into the left maxillary sinus
• Bilateral orbital involvement, more pronounced on the left
• Intracranial extension through the anterior skull base
• Multiple lateral cervical lymph nodes, the largest measuring 56 mm (left side)
Magnetic resonance imaging (MRI) of the craniofacial region demonstrated a large, aggressive soft-tissue mass centered in the nasal cavities, occupying both nasal fossae. (Figure 2)
The lesion extended laterally into the left maxillary sinus and superiorly into the ethmoid sinuses, with evidence of associated bony destruction. (Figures 2,3)
Orbital involvement was noted, characterized by invasion of the extraconal space, predominantly on the left side, resulting in clinically evident exophthalmos. (Figure3)
Superior extension through the anterior skull base was observed, with intracranial involvement at the level of the anterior cranial fossa, as demonstrated on brain MRI sequences. (Figure 4) In addition, cervical MRI revealed multiple enlarged lymph nodes, including left retropharyngeal and parotid lymphadenopathy, consistent with regional metastatic spread. (Figure 5)
Overall, MRI provided detailed assessment of the tumor’s soft-tissue extension, orbital and intracranial invasion, and nodal involvement, findings consistent with an advanced-stage esthesioneuroblastoma.
These radiologic features suggested an aggressive sinonasal malignancy.

Figure 2: Axial MRI of the facial skeleton demonstrating a tissue-signal mass centered in the nasal cavities, filling the nasal fossae with extension into the left maxillary sinus

Figure 3: Axial MRI of the facial skeleton demonstrating a mass filling the ethmoid sinus with associated bone destruction and invasion of the extraconal orbital space, resulting in left-sided exophthalmos

Figure 4: Brain MRI demonstrating intracranial extension of the lesion at the anterior cranial fossa, with involvement of the left frontal sinus
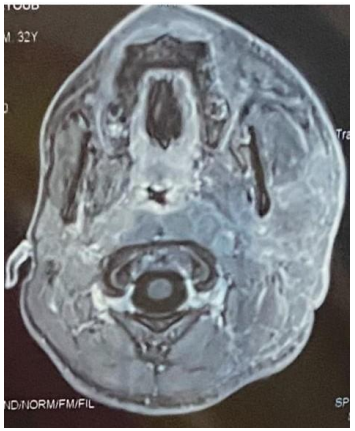
Figure 5: Axial cervicofacial MRI demonstrating left retropharyngeal and parotid lymphadenopathy
Based on radiologic findings, the patient was classified as Kadish stage C corresponding to extension beyond the nasal cavity and paranasal sinuses (Figure 1).”
Histopathology
Endoscopic biopsy demonstrated features consistent with olfactory neuroblastoma, with small round blue cell morphology and positive immunohistochemistry (synaptophysin+, chromogranin+, NSE+, S-100+ sustentacular cells).
Histopathological and immunohistochemical findings were consistent with a low-grade olfactory neuroblastoma (Hyams grade I–II).
Histopathological grading according to the Hyams classification remains a key prognostic factor in esthesioneuroblastoma (Figure 2)
Management
Due to the extensive intracranial and orbital invasion, surgical resection was deemed not feasible. The patient received combined chemoradiotherapy and supportive pain management.
The patient deceased 3 months after starting chemoradiotherapy from its complications.
Discussion
Esthesioneuroblastoma is an uncommon malignant tumor originating from the olfactory neuroepithelium of the superior nasal cavity. Although classically presenting with nasal obstruction, anosmia, epistaxis and headaches, its clinical manifestations may vary widely, especially in advanced stages where invasion of the orbit, skull base or cervical lymph nodes can occur. In the present case, the patient displayed typical rhinologic complaints initially, but the rapid development of a large cervicofacial mass reflected aggressive locoregional spread, an evolution described in advanced stages of the disease [3,4].
Endoscopic appearance alone is often insufficient to establish the diagnosis, as ENB may mimic benign nasal polyposis, presenting as a smooth, polypoid, or friable vascular mass [16]. This resemblance to benign conditions can delay diagnosis and contribute to late-stage presentation. Imaging plays a pivotal role in evaluation. Computed tomography usually demonstrates a homogeneous soft-tissue mass with moderate enhancement and may reveal intratumoral calcifications as well as bone remodeling or destruction [17].
Magnetic resonance imaging provides superior assessment of soft-tissue extension, particularly regarding orbital invasion, intracranial involvement, perineural spread, and dural infiltration, features which carry significant prognostic value [18]. In our patient, extensive sinus, orbital, and intracranial involvement were evident, consistent with a Kadish stage C tumor, which is associated with poorer outcomes and reduced resectability [7].
Histopathological confirmation remains essential for diagnosis. ENB typically exhibits lobules of small round blue cells with rosette formation, and immunohistochemistry demonstrates neuroendocrine markers such as synaptophysin, chromogranin, and neuron-specific enolase, along with S-100–positive sustentacular cells. These features help distinguish ENB from other small round blue cell tumors of the sinonasal tract, including sinonasal undifferentiated carcinoma, lymphoma, and Ewing sarcoma [19]. Hyams histologic grading further refines prognostication, with higher-grade tumors correlating with increased recurrence and poorer survival [8].
Management of ENB has shifted toward multimodal therapy. Surgery remains the cornerstone for resectable tumors, with endoscopic endonasal approaches increasingly favored due to lower morbidity and comparable oncologic outcomes to traditional craniofacial resection [20].
Radiotherapy is a critical component of treatment, improving both local control and survival, particularly in patients with advanced Kadish stage or high Hyams grade [11,21]. Chemotherapy, often platinum-based, is reserved for unresectable tumors, high-grade disease, metastatic presentations, or as part of neoadjuvant therapy to downstage lesions [12]. In the presented case, extensive intracranial invasion and bulky cervical lymphadenopathy rendered surgical resection unfeasible, necessitating combined chemoradiotherapy, an approach supported for advanced, nonresectable disease [10].
Prognosis in ENB depends on multiple factors including stage at diagnosis, histologic grade, completeness of resection, and the presence of cervical lymph node metastasis. Survival rates vary widely, with 5-year overall survival ranging from 45% to 90% depending on stage and treatment modality [22]. Cervical lymph node metastasis, as observed in our patient, occurs in fewer than 10% of cases at presentation but is associated with a less favorable prognosis [4,5]. Importantly, ENB is known for its potential for late recurrence, sometimes occurring more than a decade after initial treatment, underscoring the necessity for prolonged and vigilant follow-up [23].
This case highlights the aggressive nature of advanced ENB and the diagnostic difficulty posed by atypical or rapidly progressive presentations. Early recognition of sinonasal symptoms, comprehensive radiological evaluation, and prompt histopathological confirmation are essential to avoid delayed diagnosis. Although multimodal therapy remains the standard of care, unresectable cases continue to pose therapeutic challenges, emphasizing the need for continued research into more effective systemic therapies and advanced radiotherapy techniques.
|
Kadish Stage |
Tumor Extension |
|
Stage A |
Tumor confined to the nasal cavity |
|
Stage B |
Tumor involving the nasal cavity and paranasal sinuses |
|
Stage C |
Tumor extending beyond the nasal cavity and paranasal sinuses (e.g., orbit, skull base, intracranial space) |
|
Stage D (modified Kadish – Morita) |
Cervical lymph node and/or distant metastases |
Table 1: Kadish grading system (clinical/anatomical staging)
|
Hyams Grade |
Degree of Differentiation |
Main Histopathological Features |
|
Grade I |
Well differentiated |
Lobular architecture, abundant neurofibrillary stroma, frequent Homer–Wright rosettes, rare mitoses, no necrosis |
|
Grade II |
Moderately differentiated |
Preserved lobulation, occasional rosettes, mild nuclear atypia, low mitotic activity |
|
Grade III |
Poorly differentiated |
Reduced lobulation, rare rosettes, increased mitotic activity, focal necrosis |
|
Grade IV |
Undifferentiated |
Loss of lobular architecture, marked nuclear pleomorphism, numerous mitoses, extensive necrosis, absence of rosettes |
Table 2: Hyams histopathological grading system
Conclusion
This case illustrates a rare presentation of esthesioneuroblastoma revealed by a voluminous, rapidly progressive cervicofacial mass. In addition to classic rhinologic symptoms, this patient developed bulky cervical lymphadenopathy and intracranial/orbital extension, consistent with advanced Kadish C disease. The case underscores the importance of early recognition, comprehensive imaging, histopathological diagnosis, and the role of multimodal treatment. Unresectable cases require chemoradiotherapy and long-term follow-up, given the tumor’s propensity for late recurrence and metastatic spread.
Research Registration
• Not applicable. This study did not require prior registration.
Data Availability Statement
• All data generated or analyzed during this study are included in this published article.
Ethical Approval:
Not applicable
Informed Consent:
• Written informed consent was obtained from the patient’s family for publication of this case report and accompanying Figures
Sources of Funding:
• This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest:
• The authors declare that they have no competing interests.
References
- Thompson, L. D. (2009). Olfactory neuroblastoma. Head and neck pathology, 3(3), 252-259.
- Stelow EB, et al. (2016). Olfactory neuroblastoma: update.Adv Anat Pathol, 23,51-60.
- Rimmer J, et al. (2016). Clinical features of ENB. Clin Otolaryngol., 41:145-152.
- Dulguerov, P., Allal, A. S., & Calcaterra, T. C. (2001). Esthesioneuroblastoma: a meta-analysis and review. The lancet oncology, 2(11), 683-690.
- Wallace H, et al. (2017). Regional metastases in ENB. Head Neck, 39, 215-222.
- Saade R, et al. (2021). Distant metastases in ENB. J Neurol Surg B, 82, 123-130.
- Kadish, S., Goodman, M., & Wang, C. C. (1976). Olfactory neuroblastoma—a clinical analysis of 17 cases. Cancer, 37(3), 1571-1576.
- Hyams, V. J., Batsakis, J. G., & Michaels, L. (1988). Tumors of the upper respiratory tract and ear. Armed Forces Institute of Pathology.
- Dulguerov P, Allal AS. (2006). TNM staging for ENB.Rhinology, 44, 197-201.
- Patel SG, et al. (2016). Management of ENB. Cancer, 122,502-510.
- Yin LX, et al. (2020). Role of radiotherapy. Oral Oncol, 102,104552.
- Song CM, et al. (2017). Chemotherapy outcomes. Rhinology,55, 339-347.
- Broich G, et al. (1997). Epidemiology of ENB. Neurosurgery,41, 1056-1064.
- Tajudeen BA, et al. (2015). Presentation features. Am J Rhinol Allergy, 29, 99-104.
- Kim HJ, et al. (2019). Orbital involvement in ENB. Radiographics, 2019, 39:200-216.
- Buohliqah L, et al. (2016). Endoscopic appearance. Head Neck, 38, E32-E36.
- Sasaki T, et al. (2018). CT features. Acta Otolaryngol, 138, 746-752.
- Yin Z, et al. (2019). MRI characteristics. World Neurosurg,128, e850-e857.
- Thompson LDR. (2016). Pathology of ENB. Head Neck Pathol, 10:1-12.
- Nicolai P, et al. (2014). Endoscopic vs open resection. Laryngoscope, 124, 504-513.
- Bak M, et al. (2018). Radiotherapy results. J Craniomaxillofac Surg, 46, 145-151.
- Carey RM, et al. (2017). Survival outcomes. Int Forum Allergy Rhinol, 7, 1186-1194.
- Jiang Z, et al. (2023). Late recurrence patterns. BMC Cancer, 23, 112.
- Agha, R. A., Mathew, G., Rashid, R., Kerwan, A., Al-Jabir, A., Sohrabi, C., ... & Agha, M. (2025). Transparency in the reporting of artificial intelligence–the TITAN guideline. Premier Journal of Science, 10, 100082.