



Research Article - (2024) Volume 9, Issue 3
Epidemiological Aspect of Pericarditis during Systemic Diseases at the University Hospital of Bogodogo: 13 Cases
2Rheumatology Department, Bogodogo University Hospital, West Africa
Received Date: Sep 19, 2024 / Accepted Date: Oct 12, 2024 / Published Date: Oct 17, 2024
Copyright: ©Â©2024 Wendlassida Martin Nacanabo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nacanabo, W. M., Bayala, Y. L. T., Seghda, T. A. A., Tinni, I. A., Samadoulougou, A. K. (2024). Epidemiological Aspect of Pericarditis during Systemic Diseases at the University Hospital of Bogodogo: 13 Cases. Cardio Open, 9(3), 01-04.
Abstract
Introduction/Objective: Systemic pericarditis is caused by inflammation of the pericardial leaflets during systemic diseases. The aim of this study was to describe the epidemiological aspects of systemic pericarditis at Bogodogo University Hospital.
Patients and Methods: This were a descriptive cross-sectional study in the cardiology department of Bogodogo University Hospital from 1er January 2017 to 31 December 2023. We had included all patients admitted for pericardial effusion secondary to systemic disease. The variables collected were sociodemographic, clinical, paraclinical, therapeutic and evolutionary.
Results: A total of 13 patients were included, 9 women and 4 men. The mean age was 36.53 years (range 16-78 years). Asymptomatic forms accounted for 61.54% of our population. Chest pain, dyspnea and pericardial friction were found in 30.76%, 38.46% and 53.84% of patients respectively. Pericardial effusion was circumferential in 12 patients, with two cases of tamponade. Corticosteroid therapy combined with immunosuppressive treatment was instituted in 8 cases. The outcome was favorable in 69.23% of cases. Four deaths occurred, including two dues to tamponade and two other cases due to acute respiratory distress.
Conclusion: Pericarditis of systemic origin is relatively less frequent at Bogodogo University Hospital. Their aetiologies are dominated by systemic lupus erythematosus, with a high mortality rate.
Keywords
Pericarditis, Effusion, Systemic Diseases, Burkina Faso
Introduction
Systemic pericarditis is characterized by inflammation of the pericardium with or without pericardial effusion, often associated with systemic diseases [1]. The aetiologies of systemic pericarditis are largely dominated by connective diseases such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), scleroderma and vasculitis [2]. These aetiologies represent a significant diagnostic and therapeutic challenge for clinicians, despite medical advances [3]. Although the management of these conditions appears to be better codified, a multidisciplinary approach is required to optimize diagnosis and treatment [4]. To the best of our knowledge, few studies have focused on systemic pericarditis of any cause in Burkina Faso. Although this condition is relatively rare, it represents a complex and often under-diagnosed group of diseases, particularly in our context. The aim of this study is to describe the epidemiological features of systemic pericarditis at Bogodogo University Hospital.
Patients and Methods
This was a retrospective descriptive cross-sectional study that took place from 1st January 2017 to 31th December 2023 in the cardiology department of the Bogodogo University Hospital. Patients of both sexes hospitalized for pericardial effusion secondary to systemic disease were included in the study. Patients with pericarditis of non-systemic aetiology were excluded. The following variables were identified:
• Sociodemographic data: sex, age, occupation, place of residence;
• Clinical data including functional signs, blood pressure, height, weight, physical examination findings;
• Biological data including haemogram, CRP, ESR, creatinine, blood sugar, rheumatoid factors, anti-nuclear factors, antibodies anti-nuclear Ac, anti-native DNA Ac, anti-sm Ac, anti-nucleosome Ac, anti-ssa Ac, anti-ssb Ac, reduction in complement C3, C4.
• Electrocardiographic parameters were: presence of atrial or ventricular hypertrophy, repolarization disorder, micro or low voltage;
• The echo cardio graphic and Doppler parameters were the state of the cardiac chambers (compressed or not), the systolic function of the two ventricles, the segmental kinetics; the quantity of the effusion, the presence or not of a fibrin network;
Data entry and statistical analysis of the data collected were performed using the Epi-info software version 7.2.5.0. Graphs were produced using the Excel module of Microsoft Office 2019. The descriptive study of the different variables was carried out with the calculation of proportions for the qualitative variables and the position and dispersion parameters for the quantitative variables.
The anonymity and confidentiality of the data were respected in accordance with the recommendations of the Declaration of Helsinki. Identifiers were assigned to each patient during data collection, so that no names were found on our database.
Results
There were 13 patients, 9 women and 4 men. The mean age of our patients was 36.53 years, with extremes of 16 and 78 years. Pericarditis was asymptomatic and incidental in 61.54% (n=8) of cases. Dyspnoea and retrosternal chest pain were present in 5 patients (38.46%) and 4 patients (30.76%) respectively. Pericardial friction was present in 53.84% of patients. Pericardial effusion was circumferential in 12 (92.30%) of patients. Two patients had a very large effusion with tamponade. Figure 1 shows the distribution of patients according to the degree of pericardial effusion. No patient had a fibrin network or constriction. Pericarditis was secondary to SLE in five patients. The distribution of patients according to aetiology is shown in Figure 2. Pericarditis was inaugural to the underlying systemic disease in three cases. Corticosteroid therapy was instituted in 11 patients (84.61%). Corticosteroid therapy was combined with immunosuppressive treatment in 8 cases (61.53%). Progression under specific treatment was favorable in 69.23% of cases. Four of our patients died of tamponade in two cases and acute respiratory distress in the other two.

Figure 1: Distribution of the Number of Patients According to the Level of Abundance of Pericardial Effusion
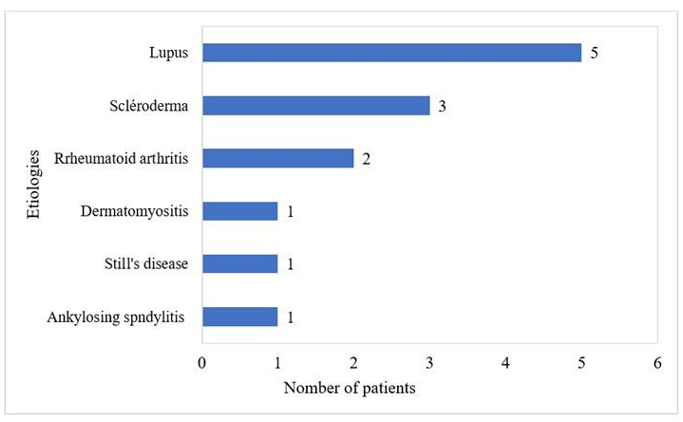
Figure 2: Distribution of Patients According to Aetiology
Discussion
Systemic etiologies of pericardial effusions in the cardiology and rheumatology departments of Bogodogo University Hospital total 13 cases in 7 years. African data concerning pericarditis of all origins exist, but very little specifically concerns pericarditis secondary to systemic diseases. For example, the hospital prevalence of liquid pericarditis from all causes was estimated at 1.7% and 5.9% in the studies conducted by Maiga et al., and Kinga et al., in Mali and Libreville respectively [5,6]. In Togo, systemic aetiologies of pericardial effusions accounted for 6% in the series by Pio et al. involving 15 patients [7]. Pericarditis of systemic origin is probably under-diagnosed in our context because, in the absence of any cardiac warning sign, cardiac ultrasound is not systematically prescribed as part of the follow-up of these patients. It is therefore difficult to assess the actual hospital prevalence of pericarditis. Also, the difficulties sometimes encountered in measuring antibodies of systemic aetiology could contribute to an under-diagnosis of these autoimmune or auto-inflammatory diseases in our context.
The mean age of our sample was 36.53 years, with a higher prevalence in women. These data are consistent with the findings of Tekaya et al, who show that systemic pericarditis often affects young adults, particularly women [2]. Thus, these pericardial attacks are consequences of systemic diseases that are generally more prevalent in women than in men. In our study, the main symptoms were chest pain and dyspnoea in 30.76% and 38.46% respectively. The clinical presentation of all pericardial lesions is identical, without prejudice to the aetiology. Chest pain and dyspnoea are contemporaneous with compression of the heart chambers, especially in large effusions. These results are consistent with several series, such as that by Tekaya et al, who reported these two signs as the main reasons for consultation [2]. The presence of pericardial friction in our series was relatively higher (53.84%) than that reported by Izibdih et al., which was 48.64% [8]. This is generally the most frequent clinical manifestation of systemic pericarditis and is of great semi logical value in this condition, although its absence does not exclude pericarditis [8].
Two of our patients presented with tamponade. Systemic pericarditis may be accompanied by tamponade in around 2% of cases, but very rarely develops into constriction [9]. The latter complication is a feature of bacterial forms of the disease, particularly tuberculosis [10]. The often-asymptomatic nature of these conditions contributes to delaying consultations, sometimes until complications arise. Hence the importance of echocardiography in assessing pericarditis and the need for careful monitoring to detect potentially serious complications such as tamponade. Pericarditis is common in rheumatological diseases, with a variable frequency ranging from 4.6 to 50% in subjects with SLE [11]. This is in line with the literature, which frequently associates SLE with systemic pericarditis. Indeed, Asri Hanane et al., reported SLE (41%) as the most frequent etiology of cardiac involvement in internal medicine, followed by neoplasia (18%) [12]. This can certainly be explained by the high prevalence of SLE, but above all by the increased risk of seritis associated with lupus markers [13]. In addition, African origin seems to be a factor favoring the association between SLE and pericarditis. In a study of 2,390 American lupus patients, pericarditis was statistically more frequent in patients of African- American origin [14].
Three out of thirteen patients in our study population presented with pericarditis as the inaugural manifestation of the underlying systemic disease. According to Tekaya et al, 66.66% of patients presenting with systemic diseases had cardiac involvement [2]. For this reason, an exhaustive complementary work-up appears justified in the presence of a notable history or in the presence of general or systemic clinical manifestations. Treatment consisted mainly of corticosteroid therapy, often combined with immunosuppression (61.54% of cases). This therapeutic approach is well established for systemic pericarditis, particularly those associated with systemic diseases [2,15]. All the difficulties in accessing certain immunosuppressive agents in our context sometimes make it difficult to apply these therapeutic protocols. This does not improve the prognosis of our patients. Mortality in this series was high, with four deaths out of thirteen, mainly due to serious complications such as tamponade and acute respiratory distress. This mortality rate is higher than in other studies such as Toujani et al [1]. The prognosis for this condition appears to be even worse in our context because our intensive care units are under-equipped. However, good interdisciplinary collaboration is required for early and effective management, which would help to improve patient prognosis.
Conclusion
In conclusion, this study provides important data on the clinical, echocardiographic, aetiological and therapeutic characteristics of pericarditis of systemic origin at the Bogodogo University Hospital. Among the aetiologies, SLE was the most frequent. Although less important than bacterial aetiologies in our context, their mortality was high. Large-scale studies are needed to determine the factors associated with death in this nosological entity.
Ethical Consideration
In conclusion, this study provides important data on the clinical, echocardiographic, aetiological and therapeutic characteristics of pericarditis of systemic origin at the Bogodogo University Hospital. Among the aetiologies, SLE was the most frequent. Although less important than bacterial aetiologies in our context, their mortality was high. Large-scale studies are needed to determine the factors associated with death in this nosological entity.
References
- Toujani, S., Daoud, F., Aydi, Z., Baili, L., Dhaou, B. B., & Boussema F. (2015). Pericarditis in systemic diseases. Rev Medecine Interne, 36, A153.
- Tekaya, A., Hamdi, M. S., Kechaou, I., Jebri, M., Cherif, E., Azzabi, S., ... & Hassine, L. B. (2023). Atteinte cardiaque au cours des maladies systémiques: profil épidémiologique, clinique, étiologique et thérapeutique. La Revue de Médecine Interne, 44, A446.
- Kervarrec, T., Binois, R., Bléchet, C., & Esteve, E. (2015, January). Hypocomplementaemic urticarial vasculitis with bullous lesions and pericardial involvement. In Annales de Dermatologie et de Venereologie, 142(10), 557-562.
- Geri, G., & Cacoub, P. (2011). Péricardites aiguësrécidivantes: mise au point et actualités 2011. La Revue de médecine interne, 32(12), 736-741.
- Maiga, B. H. (2005). Epidemiological and clinical study of acute pericarditis in the cardiology department of the HNPG: about 76 cases. Medical Thesis, 72.
- Kinga, A., Bivigou, E. A., Allognon, C., Mackanga, J. R., Mipinda, J. B., & Nzengue, J. E. (2020). Epidémiologie des étiologies des péricardites liquidiennes à Libreville. HEALTH SCIENCES AND DISEASE, 21(9).
- Pio, M., Afassinou, Y. M., Pessinaba, S., Mossi, K. E.,Kotosso, A., Baragou, S., ... & Damorou, F. (2016). Les péricardites liquidiennes: aspects cliniques et étiologiques à Lomé. Med Santé Trop, 26(1), 92-96.
- Izidbih, Y., Mouna, S., Damak, C., Bensalah, R., Frikha, F., Marzouk, S., et al. (2021). Pericarditis during systemic lupus erythematosus: about 37 cases. Rev Rhum, 88, A278.
- Dein, E., Douglas, H., Petri, M., Law, G., & Timlin, H. (2019). Pericarditis in lupus. Cureus, 11(3), e4166.
- Wazaren, H., Idrissa, A., Boussaadani, B. E., & Bakkali, A. (2024, April). Management of Constrictive Pericarditis: A study of 43 operated cases. In Annales de Cardiologie et D'angeiologie, 73(3), 101742.
- MaksimoviÄ?, R., SeferoviÄ?, P. M., RistiÄ?, A. D., VujisiÄ?- TešiÄ?, B., SimeunoviÄ?, D. S., RadovanoviÄ?, G., ... & Maisch, B. (2006). Cardiac imaging in rheumatic diseases. Rheumatology, 45(suppl_4), iv26-iv31.
- Yahia, WB, Bouker, A., Atig, A., Guiga, A., Ghannouchi, N., & Bahri, F. (2016). Etiological profile of pericarditis in an internal medicine department. The Journal of Internal Medicine , 37 , A152-A153.
- Somai, M., Daoud, F., Rachdi, I., Zoubeidi, H., Aydi, Z., Ben-Dhaou, B., et al. (2018). Prevalence and risk factors of serositis in patients with systemic lupus erythematosus. Rev Internal Medicine, 39, A159.
- Ryu, S., Fu, W., & Petri, M. A. (2017). Associates and predictors of pleurisy or pericarditis in SLE. Lupus science & medicine, 4(1), e000221.
- Pieta, A., Pelechas, E., Gerolymatou, N., Voulgari, P. V., & Drosos, A. A. (2021). Calcified constrictive pericarditis resulting in tamponade in a patient with systemic lupus erythematosus. Rheumatology International, 41(3), 651-670.