
Journal of Educational & Psychological Research(JEPR)
ISSN: 2690-0726 | DOI: 10.33140/JEPR
Impact Factor: 1.4

Review Article - (2026) Volume 0, Issue 0
Entangled Minds: A Medical Narrative of AuDHD, Autonomic Dysregulation, and the Complexity of Neurodevelopmental Overlap
Received Date: Mar 23, 2026 / Accepted Date: Apr 22, 0026 / Published Date: May 06, 2026
Copyright: ©2026 Bruce H Knox. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Knox, B. H. (2026). Entangled Minds: A Medical Narrative of AuDHD, Autonomic Dysregulation, and the Complexity of Neurodevelopmental Overlap. J Edu Psyc Res, 8(2), 01-05.
Abstract
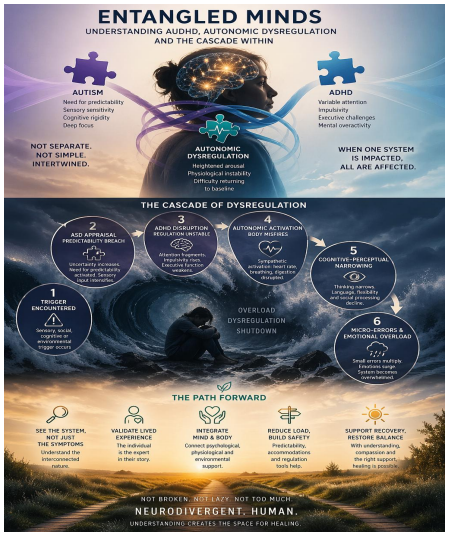
Co-occurring Level 1 Autism Spectrum Disorder (ASD) and Attention-Deficit/Hyperactivity Disorder (ADHD), commonly termed AuDHD, represent a complex neurodevelopmental profile characterised by interacting cognitive, behavioural, and physiological systems [1-3]. This paper integrates clinical literature with detailed lived experience to examine how ASD, ADHD, and autonomic dysfunction form an interdependent entanglement, producing cascade-based dysregulation rather than isolated symptoms [2,4,5]. The narrative introduces a sequential model of escalation, moving from trigger through cognitive appraisal, autonomic activation, perceptual narrowing, and functional collapse [4-7]. The analysis demonstrates how overlapping conditions amplify one another and why siloed diagnostic frameworks are often inade- quate [1,2,8]. Clinical implications include the need to recognise cascade dynamics, to integrate physiological as well as psychological interventions, and to value patient narrative as essential diagnostic data [5,6,9].
This paper is also expressed in the terms of musical lyrics, with the composition and presentation for you to listen to. Please click on the following link, turn the page, and click on the bottom right-hand corner.
https://heyzine.com/flip-book/a117aa6649.html
Keywords
AuDHD, Autism, ADHD, Dysautonomia, Neurodivergence, Autonomic Dysfunction, Lived Experience
Introduction
The co-occurrence of ASD and ADHD is now well recognised, with research suggesting substantial overlap between the two conditions across childhood and adulthood [1,2]. Historically, however, clinical systems have tended to assess and conceptualise them separately, often overlooking the interactive nature of their effects [2,3].
This separation does not match lived reality. For many individuals, these are not parallel diagnoses operating independently, but interwoven processes affecting attention, sensory regulation, behavioural control, emotional response, and bodily state at the same time [4,8].
This paper argues that AuDHD is most accurately understood as a dynamic neurodevelopmental system, particularly when accompanied by autonomic dysregulation. It draws on lived experience and clinical literature to propose a cascade-based model in which ASD, ADHD, and physiological instability do not merely coexist, but amplify one another [5,6,9].
The Lived Experience of Cognitive Entanglement
The internal experience is not one of tidy diagnostic separation. It is one of simultaneity, contradiction, and cumulative load. The lived narrative expresses this clearly:
“A symphony of struggles, a chaotic dance… each note a challenge.”
This description reflects not chaos in the sense of absence of order, but multiple systems competing for regulatory control.
From a clinical perspective, ASD may contribute a heightened need for predictability, sensory sensitivity, and cognitive rigidity [10]. ADHD may contribute variable attention, impulsivity, executive instability, and inconsistent self-regulation [3,11]. Autonomic dysfunction may contribute bodily overactivation, fatigue, tachycardia, dizziness, gastrointestinal disruption, and difficulty returning to baseline [5,6]. Together, these create a system that is both highly responsive and highly vulnerable to overload.
The lived experience is therefore not of “having several separate things wrong,” but of inhabiting one organism in which cognition, behaviour, and physiology are tightly entangled.
Why Diagnostic Silos Fail
Conventional diagnostic thinking often assumes that symptoms can be allocated cleanly to one disorder or another. In practice, this may obscure the underlying pattern [2,8]. For example:
• A need for routine may be coded as autistic rigidity
• Distractibility may be coded as ADHD
• Racing heart and dizziness may be treated as separate medical complaints
Yet in lived experience these do not arise in isolation. They unfold together. One disturbance may trigger the next, until the whole system is affected.
This is a clinically important point. If assessment focuses only on discrete symptoms without attending to sequence and interaction, the result may be partial diagnosis, fragmented intervention, and repeated misunderstanding [8,9,12].
The Entanglement Cascade Model
Drawing from lived experience, a sequential model of dysregulation emerges. This does not imply that every episode is identical, but that a recognisable pattern often unfolds.
Stage 1: Trigger Encountered
A trigger may be sensory, social, cognitive, or environmental. Examples include unexpected noise, interruption, ambiguity, schedule change, excessive demand, or interpersonal tension [10,13].
Stage 2: ASD Appraisal — Predictability Breach
The autistic component of the system responds first to disruption of structure. Uncertainty and unpredictability increase cognitive strain, and sensory input may become more salient [10,14]. The system begins to shift from open engagement to containment.
Stage 3: ADHD Disruption — Regulation Becomes Unstable
At this stage, attentional control may fragment. Competing inputs multiply. Task sequencing becomes less reliable, and impulsive or scattered responses may emerge [3,11]. The need for order intensifies, while the ability to maintain it weakens.
Stage 4: Autonomic Activation — The Body Misfires
Once the threshold is crossed, the body begins to participate more visibly. Sympathetic activation may produce tachycardia, dizziness, shallow breathing, gastrointestinal discomfort, tremor, or heat changes [5,6,15].
Stage 5: Cognitive–Perceptual Narrowing
As autonomic arousal rises, higher-order executive processes begin to constrict [7,16]. Language retrieval may falter. Social interpretation becomes harder. Flexibility declines. Thought becomes more defensive, narrowed, or locked.
Stage 6: Micro-Errors Accumulate
Small mistakes now begin to multiply: missed cues, misplaced items, sequencing errors, incomplete steps, misread tone, or failed transitions. In a system already under strain, these errors do not remain minor. They act as further triggers.
Stage 7: Emotional Dysregulation
At this stage, feelings such as frustration, shame, urgency, or resignation may intensify rapidly. Emotional dysregulation is not simply psychological in origin here; it is being driven by the combined effects of overload, autonomic arousal, and executive collapse [7,17].
Stage 8: Functional Spillover
What began as one disruption now spills into multiple domains. Work, communication, memory, social engagement, physical regulation, and planning all begin to deteriorate together. The individual is no longer dealing with a single problem, but with a cascading systems event.
Stage 9: Shutdown, Overwhelm, or Collapse
The lived narrative expresses this vividly: “My brain, a battlefield… internal conflict, day and night.” At this point, the presentation may resemble panic, shutdown, freeze, or complete functional exhaustion. The outward behaviour may appear disproportionate to the original trigger, but the internal sequence explains why it is not [6,7,15].
Stage 10: Recovery and Reframing
Recovery requires more than “calming down.” It requires reduction of input, restoration of bodily regulation, cognitive simplification, and often time. If properly understood, this phase also offers an opportunity for pattern recognition, self-understanding, and preventive adaptation [9,12].
Physiological Amplification: The Role of Dysautonomia
The inclusion of autonomic dysfunction is essential to this paper’s argument. Too often, behavioural and emotional dysregulation in neurodivergent individuals is explained purely in cognitive or psychiatric terms. Yet the body is not a passive bystander [5,6].
The lived material states:
“Heart racing… a delicate dance of regulation.”
This is clinically significant. Dysautonomia involves dysregulation of the autonomic nervous system, especially in the balance between sympathetic and parasympathetic activity [5,15]. When this system becomes unstable, bodily arousal can escalate quickly and resolve slowly. The result is that a cognitive or sensory trigger is converted into a full-bodied stress event.
Once this occurs, physiology feeds back into cognition. The individual now has to interpret not only the external situation, but also internal signals such as pounding heart, light-headedness,
nausea, or breathlessness. These signals themselves can intensify vigilance and distress [16,18]. A self-reinforcing loop is created.
This helps explain why the resulting reaction may appear “too big” in relation to the trigger. The trigger is only the entry point. The magnitude of the response reflects the total system response.
Cognitive Conflict Within AuDHD
One of the most difficult aspects of AuDHD is that the component conditions may pull in opposite directions [2,3]. The autistic part of the system may seek order, routine, and predictability. The ADHD part may generate variability, restlessness, impulsivity, novelty-seeking, or difficulty sustaining organization [3,11].
This creates an internal contradiction. The person may desperately need structure, yet struggle to maintain it. They may crave predictability, yet be drawn into distraction or inconsistency. They may have the capacity for intense hyperfocus, yet also lose track of sequencing, timing, and transitions.
The lived narrative captures this tension:
“My brain, a battlefield… a constant fight.”
This internal conflict is not a sign of poor motivation or weak character. It is the felt consequence of overlapping neurodevelopmental demands acting on the same system [2,8].
Functional Impact in Daily Life
The impact of this entanglement is cumulative rather than merely episodic. It is not confined to obvious crises. It also shapes everyday functioning through vigilance, fatigue, anticipatory planning, and the need to recover from seemingly ordinary demands [9,12].
The lived material notes:
“Each note a challenge… a unique circumstance.”
This is an important clinical insight. Many adults with complex neurodevelopmental profiles are not struggling only in moments of visible distress. They are expending significant energy every day to maintain baseline functioning. Outward competence may therefore conceal continuous adaptive labour [9,19].
Patient Voice
It does not feel as if I have several separate conditions that take turns appearing. It feels like one integrated system, fast-moving and hard to regulate, with different aspects becoming more visible at different moments.
Sometimes I need structure more than anything else. At other times, I cannot hold that structure in place. Something small goes wrong, and it does not stay small. It spreads through attention, body, emotion, and function until the whole day is affected.
From the outside, this can look like overreaction or inconsistency. From the inside, it is a system reaching its regulatory limit. Recovery is not indulgence. It is part of how the system survives.
Clinical Implications
Move Beyond Siloed Diagnosis
Clinicians should avoid assuming that ASD, ADHD, and autonomic symptoms can be fully understood in isolation [2,8]. Their interaction may be more clinically relevant than their separate descriptions.
Attend to Sequence, Not Just Symptoms
The order in which events unfold is diagnostically important. A cascade model helps identify early stages of dysregulation, before full functional collapse occurs [9,12].
Include Physiology in Formulation
Assessment should include autonomic symptoms, interoceptive experience, bodily signs of overload, and recovery time [5,15,18].
Use Multi-Domain Intervention
Effective support may require environmental structure, executive supports, sensory regulation, physiological calming strategies, and psychoeducation that helps the individual understand the sequence of escalation [6,7,20].
Value Narrative as Data
Patient accounts of sequence, subjective experience, and contextual triggers are not ancillary. They are essential to understanding how the system actually functions [9,12].
Key Learning Points for Clinicians
i. **AuDHD is best understood as an interactive system rather than two parallel diagnoses [1,2,8].**
ii. Dysregulation often follows a cascade pattern. Early recognition of stages may prevent full system overload [9,12].
iii. Autonomic dysfunction can play a major amplifying role. Behavioural and emotional escalation may be physiologically driven as well as cognitively mediated [5,6,15].
iv. Internal contradiction is a core lived feature of AuDHD. The simultaneous need for structure and difficulty maintaining it should not be misread as oppositionality or lack of effort [2,3].
v. Narrative accounts improve formulation. They reveal patterns, timing, and context that are often invisible in standard assessments [9,12].
vi. Intervention must be synchronised across domains. Cognitive, behavioural, sensory, and physiological supports are most effective when integrated [17,20].
Conclusion
The entanglement of ASD, ADHD, and autonomic dysregulation creates a complex neurodevelopmental system in which cognition, behaviour, emotion, and physiology are mutually influential. The lived experience is not one of separate symptoms appearing one by one, but of interacting processes that build upon one another until the system either stabilises or collapses.
This paper has argued that understanding AuDHD requires a shift in clinical perspective: from diagnosis to dynamics, from isolated traits to sequence, and from externally observed symptoms to internally lived process.
Only when the full system is seen can the response become accurate, humane, and effective.
References
- Leitner, Y. (2014). The co-occurrence of autism and attention deficit hyperactivity disorder in children–what do we know?. Frontiers in human neuroscience, 8, 268.
- Antshel, K. M., & Russo, N. (2019). Autism spectrum disorders and ADHD: Overlapping phenomenology, diagnostic issues, and treatment considerations. Current psychiatry reports, 21(5), 34.
- Faraone, S. V., & Biederman, J. (1998). Neurobiology of attention-deficit hyperactivity disorder. Biological psychiatry, 44(10), 951-958.
- Kooij, S. J., Bejerot, S., Blackwell, A., Caci, H., Casas-Brugué, M., Carpentier, P. J., ... & Asherson, P. (2010). European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC psychiatry, 10(1), 67.
- Benarroch, E. E. (1993, October). The central autonomic network: functional organization, dysfunction, and perspective. In Mayo clinic proceedings (Vol. 68, No. 10, pp. 988-1001). Elsevier.
- Raj, S. R. (2013). Postural tachycardia syndrome (POTS).Circulation, 127(23), 2336-2342.
- Arnsten, A. F. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature reviews neuroscience, 10(6), 410-422.
- Sonuga-Barke, E. J. (2005). Causal models of attention-deficit/ hyperactivity disorder: from common simple deficits to multiple developmental pathways. Biological psychiatry, 57(11), 1231-1238.
- Livingston, L. A., & Happé, F. (2017). Conceptualising compensation in neurodevelopmental disorders: Reflections from autism spectrum disorder. Neuroscience & Biobehavioral Reviews, 80, 729-742.
- Robertson, C. E., & Baron-Cohen, S. (2017). Sensory perception in autism. Nature reviews neuroscience, 18(11), 671-684.
- Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychological bulletin, 121(1), 65-94.
- Pellicano, E., & den Houting, J. (2022). Annual research review: Shifting from ‘normal science’to neurodiversity in autism science. Journal of child psychology and psychiatry, 63(4), 381-396.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. 5th ed. Washington (DC): American Psychiatric Association.
- Corbett, B. A., Simon, D. (2014). Emotion regulation in autism spectrum disorder. J Autism Dev Disord. 44(9), 2263-73.
- Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotion regulation and dysregulation. Journal of affective disorders, 61(3), 201-216.
- Craig, A. D. (2002). How do you feel? Interoception: the sense of the physiological condition of the body. Nature reviews neuroscience, 3(8), 655-666.
- Shah, P., Hall, R., Catmur, C., & Bird, G. (2016). Alexithymia, not autism, is associated with impaired interoception. cortex, 81, 215-220.
- Porges, S. W. (2007). The polyvagal perspective. Biological psychology, 74(2), 116-143.
- Cassidy, S., Bradley, L., Shaw, R., & Baron-Cohen, S. (2018). Risk markers for suicidality in autistic adults. Molecular autism, 9(1), 42.
- Deci, E. L., & Ryan, R. M. (2000). The" what" and" why" of goal pursuits: Human needs and the self-determination of behavior. Psychological inquiry, 11(4), 227-268.