
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2021) Volume 6, Issue 2
Egocentric Networks and HIV in Pregnant and Breastfeeding Women Attending Antenatal Care in Lusaka, Zambia
2Duke Network Analysis Centre, Duke University, Durham, North Carolina, USA
3Department of Sociology, Duke University, Durham, North Carolina, USA
4UNC Global Projects Zambia, Lusaka, Zambia; Mildred Lusaka, MSc, UNC Global Projects Zambia, Lusaka, Zambia
5MD, MPH, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, North Carolin, USA
6Lecturer/Researcher, Dept. of Health Promotion and Education, School of Public Health, University of, Zambia
Received Date: Apr 26, 2021 / Accepted Date: May 04, 2021 / Published Date: May 12, 2021
Copyright: ©Kellie Freeborn, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kellie Freeborn, Maria C Ramos, Dana K Pasquale, Rose Lungu, Benjamin H Chi, Oliver Mweemba. (2021). Egocentric Networks and HIV in Pregnant and Breastfeeding Women Attending Antenatal Care in Lusaka, Zambia. Int J Women's Health Care, 6(2), 165-177.
Abstract
Human immunodeficiency virus (HIV) has a disproportionate effect on pregnant and breastfeeding women in sub-Saharan Africa. This study used egocentric social network analysis (SNA) to compare the social and sexual networks of HIV-negative and HIV-positive women attending an antenatal care (ANC) clinic in Lusaka, Zambia. In order to assess risk and protective factors for HIV acquisition and transmission, variables included self (ego) sociodemographic characteristics, main partner characteristics, features of the relationship between ego and her main partner, alter attributes, alter-ego ties, and alter-alter ties. Associations between the independent variables and ego HIV status were identified using bivariate tests. Logistic regression analyses were performed to assess the relationship between predictors and ego HIV status when multiple variables were included in the same model. Overall, 219 participating women (69 HIV-positive, 150 HIV-negative) nominated 1095 alters. Compared to HIV-negative egos, HIV-positive egos were older, had main partners who were more likely to consume alcohol before sex, disclosed their HIV status to fewer alters, had fewer alters with whom they had daily interactions, and had more alters who were HIV-positive or HIV-unknown. Number of alters who were HIV-positive or HIV-unknown and non-disclosure of HIV status were the greatest risks (with the effect of HIV-positive or HIV-unknown being of a slightly greater magnitude than non-disclosure of HIV status), which places breastfeeding women, their partners and their infants at risk of preventable HIV infection.
Keywords
Social Network Analysis, HIV Prevention, Pregnancy, Sub-Saharan Africa, Zambia, Egocentric Networks
Introduction
The disproportionate impact of the HIV epidemic on pregnant and breastfeeding women involves various biological, social, behavioural, cultural, economic and structural elements [1-3]. In sub-Saharan Africa (SSA), women face constraints on the naviga- tion of sexual safety, and factors operating across the socioecologi- cal arena at multiple levels (e.g., individual, partnership, peers and communities, societal) influence not only women’s HIV vulnera- bility, but also that of their male partner [4,5]. Additionally, fear of stigma, loss of social capital, gender inequality, discrimination and potential violent reactions causes many women in SSA to avoid HIV disclosure [6]. The disproportionate impact of HIV on preg- nant and breastfeeding women is evident in urban populations in Zambia, where more than 60% of new HIV infections occur within marriage or cohabiting relationships [7]. Despite several program- matic efforts to address HIV risks, many of the influences on the risk behaviours of pregnant and breastfeeding women are poorly understood, leaving many women, their partners, and their infants at continued risk of acquiring HIV [8,9].
Behaviours perceived as normative within social networks are ad- opted by individuals to reinforce a sense of identity and belonging to a group [10]. Thus, social network analysis (SNA) may be use- ful in understanding the influences on pregnant and breastfeeding women’s HIV protective behaviours and vulnerability. Howev- er, few have studied women’s social and sexual networks during pregnancy and breastfeeding, or how these networks contribute to HIV risk, prevention and transmission.
Egocentric SNA is a methodological tool used to understand the structure, function, and composition of network ties around an individual. Egocentric sampling is designed for the collection of network data from the index individual (known as the ego) about the people in their social network (known as alters) without re- cruitment or direct observation of the alters. It is particularly use- ful for the collection of sensitive data regarding sexual behaviors, substance and alcohol use and gambling [11-13]. SNA generally can reveal how individual, behavioral, and social network factors influence engagement in risk behavior and specifically how such factors shape pregnant and breastfeeding women’s HIV-related be- haviors and beliefs [14-18].
In Zambia, as in much of SSA, accessing healthcare is considered a predominantly female domain, and it is therefore often challeng- ing to recruit male study participants [19]. Taking a pragmatic view of this gender norm, we opted to use an egocentric approach to analyse pregnant/breastfeeding women’s social networks to reveal previously unobservable links to HIV risk and protective behaviours, not only for the women themselves but also for the men in their networks. We hypothesized that a woman’s social and sexual networks during pregnancy and breastfeeding contribute to continued HIV risk. In addition, we hypothesized that the patterns of relationships within the sexual networks of HIV-negative and HIV-positive women exhibit direct and indirect ties that affect HIV risk behaviour.
Materials and Methods
Site and Population
Study staff recruited pregnant and breastfeeding women attending mother and child health care visits at Chipata Level 1 Hospital, a government health facility run by the Lusaka District Health Office (LDHO) in Lusaka, Zambia. Serving a population of over 100,000, the mother and child clinic has an average of 400-450 new patients and 900-1000 return visits each month, and an HIV prevalence of ~15%. The study was conducted from December 2019 to March 2020. We planned to recruit a convenience sample of 300 participants similar to other published SNA studies howev- er, due restrictions related to the COVID-19 pandemic, the study was terminated early [20,21].
Recruitment and Enrolment Procedures
Before study commencement, a community worker sensitized the women to the study through a series of morning talks at the study site. Study staff provided women interested in the study with information regarding the study requirements and a referral to the study clinic. The inclusion criteria were: ≥18 years of age, pregnant or breastfeeding, documented HIV status (either positive or negative) in the antenatal record within 30 days of study par- ticipation, reported at least one current sexual partner within the past six months, ability to name five men in their social circle, and willingness to provide informed consent. At time of screening, women who expressed concerns about intimate partner violence (IPV) or social harms resulting from participation were considered ineligible for the study. All participants provided written informed consent as per local guidelines.
Ethics
Study participants were fully informed of the study procedures, the risks and benefits, privacy and confidentiality and their right to withdraw or not participate in the study. The study was approved by the University of Zambia Biomedical Research Ethics Com- mittee, the Zambian National Health Research Authority, the Lu- saka District Health Office, and the University of North Carolina at Chapel Hill Institutional Review Board.
Data Collection Tools
To inform our study questionnaire, we conducted a thorough liter- ature review of HIV risk factors for women in sub-Saharan Africa, of which the following were prioritised for further investigation: multiple concurrent sexual partners, transactional sex, dry sex, anal sex, polygamy, sex with older partners, fear of rejection, alcohol use and violence [22-28]. The literature review further revealed that in Zambia, only 41% of women use a condom when engaging in high-risk sexual practices, compared to 55% of the prevalence of alcohol consumption in pregnancy is 18.5% and an estimated 30% of women are intimate partner violence victims [7,29]. Add- ing to women’s HIV risk is the unknown serostatus of their male partners, as men in SSA are less likely than women to utilize HIV testing services [30]. Compounding these issues is the fact that, for economic reasons, both men and women in SSA mobilize for employment, which creates further opportunities for sexual net- working and is known to encourage high-risk sexual behaviour [31]. Thus, we included sections in the data collection instrument to elicit information regarding these known HIV risks.
Data Collection Tools
The data collection procedure consisted of two sections. First, due to the sensitive nature of many of our questions—and to ensure confidentiality of our participants—we utilised audio computer-as- sisted self-interview (ACASI) to collect non-network data similar to other studies [32,33]. The ACASI software was programmed us- ing Kobo Toolbox (Harvard Humanitarian Initiative, Cambridge, MA, USA) and installed onto tablet computers. The survey includ- ed questions about participants, their main partners’ sexual health, HIV status, alcohol use, number of partners and demographics. It took 15-30 minutes to complete. After informed consent was obtained, participants were shown how to use the ACASI by a local research assistant. The computer displayed one question at a time and read the questions and responses to the participant in the language of their choice (English, Bemba, Nyanja) using asso- ciated M4A audio files pre-recorded by a female native speaker. The participant entered responses using the keyboard, mouse or touch screen. As a direct interviewer is not required to conduct an ACASI, a single staff member supervised multiple interviews simultaneously [34].
After completing the ACASI, information regarding the partic- ipants’ sexual and social networks was collected using Ego Net 2.0™ software (Medical Decision Logic, Inc., Baltimore, MD). The participants entered their responses directly using a keyboard, mouse or touch screen [34]. Each participant (ego) provided the first name only of five men in her social network (alters) with whom she had had a friendship, familiar relationship, romantic relationship or sexual relationship over the past twelve months. Egos indicated the type of relationship they had with each alter named. They could choose one of the following categories: friend, husband, relative, sex client, someone who gives me money, some- one who pays for my shelter, or father of my child. The ego then answered the following questions about each alter: age; if they are a migrant worker; if they provide financial support; if they provide advice about preventing HIV; if they have disclosed their HIV sta- tus; if they use ART or PrEP; and if she has had sex with the alter. Lastly, the ego answered questions about the relationships between her alters. It took 10-20 minutes to complete the ego network sec- tion of the data collection procedure. Upon completion of study activities, including the ACASI and ego network portions of the interview, participants received transport reimbursement (equiva- lent of $5 USD) in local currency.
Study Variables
The study dependent variable was ego HIV status, which was cat- egorized according to the participant’s antenatal card, where is it typically recorded. Independent variables were grouped into six categories: (1) ego sociodemographic characteristics; (2) main partner characteristics; (3) features of the relationship between ego and her main partner; (4) features of the relationships between alters and egos (i.e., alter-ego ties); (5) alter attributes; and (6) fea- tures of the relationships between alters (i.e., alter-alter ties).
Ego sociodemographic characteristics included age in years, ethnicity (Bemba, Nyanja, and Other), level of education (no schooling, some schooling, and completed secondary school), and whether ego was financially dependent on their main partner. Main partner characteristics included ego’s main partner employment status (employed versus unemployed) and whether ego’s main partner had been circumcised.
Four variables described the relationship between egos and their main partners. We considered whether ego’s main partner had dis- closed his HIV status to ego, whether ego’s main partner used a condom for vaginal sex, and whether ego’s main partner consumed alcohol before sex. We also included the degree to which ego trust- ed her main partner when he said he did not have sex with others, measured in a scale ranging from 0 (do not trust him at all) to 3 (trust him completely).
Alter-ego tie variables shed light on the relationships between egos and alters. These variables included nominating one or more rel- atives, the number of alters who were fathers of ego’s children, the number of alters to whom egos had disclosed her HIV status, the number of alters with whom ego had daily interactions, and the number of occasional sexual partners (partners with whom ego had sexual relationships sometimes). In addition, we obtained the mean frequency of contact between ego and them alters using the item: “How frequently do you interact with [alter]? By that we mean talk to, spend time with” (once a year, every few months, monthly, weekly, or daily). We also considered the amount of sup- port egos received from alters. Then, we averaged the responses obtained at the ego level. We also calculated a measure of support by combining responses to the items about financial support and advice: “Does [alter] provide you with advice about preventing HIV?” and “Do you rely on [alter] for financial support?” For each alter and item, responses were coded as not at all, sometimes, of- ten, or all the time. Next, responses for each alter and item were summed per ego, resulting in a score at the ego level.
Four variables described alter attributes. First, we included the number of HIV-positive or HIV-unknown alters. A second vari- able described the ethnic similarity between ego and her alters: Krackhardt and Stern’s external-internal (E-I) Index, which mea- sures ego’s propensity to have ties to alters with the same nomi- nal characteristic, compared to the propensity to have alters with a different nominal characteristic [35]. The index ranges from −1 to +1 where −1 is completely homophilous (i.e., all alters are of the same ethnicity as ego) and +1 is completely heterophilous (i.e., all alters are ethnically different from ego). A third variable indicated whether ego had one or more sexual partners who were migrant workers. A fourth variable, the number of years between ego’s and her sexual partners’ age, captured age dissimilarity.
Finally, we included network density as a measure of the connec- tivity between alters. Network density is the number of ties among alters that are present in the network out of the possible number of ties if ego was connected to every other alter. In the present study, a tie between alters indicated they know each other. Appendix A presents a complete list of the variables included in the study, the interview items from which they were constructed, and the final coding utilized in the analyses. Variables were coded in order to maximize the differences between HIV-positive and HIV-negative egos while retaining variables with results greater than twenty per category.
APPENDIX A
|
Study variables |
|||
|
Variable |
Item |
Original response options |
Final coding of responses |
|
Ego sociodemographics |
|
|
|
|
Ego age |
How old are you? |
Age in years |
Age in years |
|
Ego ethnicity |
Which ethnic groups do you belong to? |
Bemba (N = 77 - 35.16%) Nyanja (N = 121 - 55.25%) Tonga (N = 7 - 3.20%) Senga (N = 5 - 2.28%) Mambwe (N = 4 - 1.83%) Lozi (N = 1 - 0.46%) Ngoni (N = 3 - 1.37%) Ndebele (N = 1 - 0.46%) |
Bemba Nyanja Other (includes Tonga, Senga, Mambwe, Lozi, Ngoni, and Ndebele) All respondents identified as part of only one ethnic group |
|
Ego level of education |
What is your current education level? |
No school (N = 42 - 19.18%) Some primary school (N = 60 - 27.40%) Completed primary school (N = 22 - 10.05%) Some secondary school (N = 42 - 19.18%) Completed secondary school (N = 51 - 23.29 %) |
No school Some schooling (includes some primary school, completed primary school, and some sec- ondary school) Completed secondary school |
|
Ego depends financially on partner |
During the past 12 months, where did you get most of your money? |
Employment (N = 57 - 26.03%) Family (N = 72 - 32.88%) Friends (N = 9 - 4.11%) Partner (N = 79 - 36.07%) |
1 indicates ego obtains most of her money from partner, 0 otherwise |
|
Main partner characteristics |
|||
|
Main partner is employed |
Please answer the following questions about your MAIN PARTNER… Is he employed? |
Yes (N = 137 - 62.56%) No (N = 72 - 32.88%) I don’t know (N = 7 - 3.20%) |
Yes, No, NA (includes I don’t know and NA) |
|
Main partner has been circum- cised |
Please answer the following questions about your MAIN PARTNER… To the best of your knowledge, has this part- ner been circumcised? |
Yes (N = 101 - 46.12%) No (N = 100 - 45.66%) I don’t know (N = 11 - 5.02%) |
Yes, No, NA (includes I don’t know and NA) |
|
Relationship between ego and main partner |
|||
|
Main partner disclosure of HIV status to ego |
Please answer the following questions about your MAIN PARTNER… Has he told you his HIV status? |
Yes (N = 163 - 74.43%) No (N = 43 - 19.63%) I don’t know (N = 0 - 0%) |
Yes, No, NA (includes I don’t know and NA) |
|
Main partner uses condom during vaginal sex |
Please answer the following questions about your MAIN PARTNER… Do you use a condom when you have vaginal sex with him? |
Always (N = 22 - 10.05%) Sometimes (N = 81 - 36.99%) Never (N = 99 - 45.21%) |
1 = sometimes or always 0 = never |
|
Main partner consumes alcohol before sex |
Please answer the following questions about your MAIN PARTNER… How often does he have a drink containing al- cohol just before or during sex? |
Always (N = 15 - 6.85%) Sometimes (N = 47 - 21.46%) Never (N = 154 - 70.32%) |
1 = sometimes or always 0 = never |
|
Ego trusts main partner |
Please answer the following questions about your MAIN PARTNER… Do you trust him when he tells you he does not have sex with other people? |
I do not trust him at all (N = 47 - 21.46%) I trust him some of the time (N = 47 - 21.46%) I trust him most of the time (N = 45 - 20.55%) I trust him completely (N = 55 - 25.11%) |
Coded as a numeric scale: 0 = I do not trust him at all, 1 = I trust him some of the time, 2 = I trust him most of the time, 3 = I trust him completely. |
|
Alter-ego tie variables |
|||
|
One or more relatives |
How would you describe your relationship with [alter]? |
Friend (N = 525 - 47.95%) Husband (N = 175 - 15.98%) Relative (N = 308 - 28.13%) Sex client (N = 11 - 1.00%) Someone who gives me money (N = 5 - 0.46%) Someone who pays for my shelter (N = 1 - 0.09%) Father of my child (N = 75 - 6.85%) |
1 = one or more alters are relatives 0 = none of ego’s alters are relatives |
|
Number of alters fathers of ego’s children |
How would you describe your relationship with [alter]? |
Friend (N = 525 - 47.95%) Husband (N = 175 - 15.98%) Relative (N = 308 - 28.13%) Sex client (N = 11 - 1.00%) Someone who gives me money (N = 5 - 0.46%) Someone who pays for my shelter (N = 1 - 0.09%) Father of my child (N = 75 - 6.85%) |
Number of alters who are fathers of ego’s children. |
|
Mean frequency of contact |
How frequently do you interact with [alter]? By that we mean talk to, spend time with. |
Daily (N = 329 - 30.05%) Weekly (N = 252 - 23.01%) Monthly (N = 228 - 20.82%) Every few months (N = 118 - 10.78%) Once a year (N = 173 - 15.80%) |
For each alter, responses were coded as: 1 = once a year, 2 = every few months, 3 = month- ly, 4 = weekly, 5 = daily. Then, an average was calculated at the ego level |
|
Number of alters with whom ego has daily interactions |
How frequently do you interact with [alter]? By that we mean talk to, spend time with. |
Daily (N = 329 - 30.05%) Weekly (N = 252 - 23.01%) Monthly (N = 228 - 20.82%) Every few months (N = 118 - 10.78%) Once a year (N = 173 - 15.80%) |
Number of alters with whom interactions occur daily. |
|
Support (sum of advice and financial support scores) |
Does [alter] provide you with advice about preventing HIV? Do you rely on [alter] for finan- cial support? |
Not at all (N = 584 - 53.33%) Sometimes (N = 297 - 27.12%) Often (N = 123 - 11.23%) All the time (N = 96 - 8.77%) Not at all (N = 672 - 61.37%) Sometimes (N = 249 - 22.74%) Often (N = 59 - 5.39%) All the time (N = 120 - 10.96%) |
For each alter and item, re- sponses were coded as: 1 = not at all, 2 = sometimes, 3 = often, 4 = all the time. Then, respons- es for each alter and item were summed per ego, resulting in a score at the ego level. |
|
Number of alters to whom ego has disclosed HIV status |
Have you disclosed your cur- rent HIV status to [alter]? |
Yes (N = 465 - 42.47%) No (N = 620 - 56.62%) I don’t know (N = 15 - 1.37%) |
Yes, No, NA (includes I don’t know and NA) |
|
Number of “sometimes” sexual partners |
Do you have sex with [alter]? |
Always (N = 169 - 15.43%) Sometimes (N = 162 - 14.79%) Never (N = 769 - 70.23%) |
Number of “sometimes” sexual partners |
|
Alter attributes |
|||
|
Number of HIV-positive or HIV-unknown alters |
Is [alter] HIV-positive? Is [alter] HIV-negative? |
Yes (N = 86 - 7.85%) No (N = 503 - 45.94%) I don’t know (N = 511 - 46.67%) Yes (N = 458 - 41.83%) No (N = 37 - 3.38%) I don’t know (N = 605 - 55.25%) |
Number of alters identified by the respondent as HIV-posi- tive or HIV-unknown. Alters about whom ego provided inconsistent responses (e.g., “yes” to both items or “no” to both items) are coded as “unknown.” |
|
E-I based on ethnicity |
Which ethnic groups does [alter] belong to? |
Bemba (N = 353 - 32.24%) Nyanja (N = 368 - 33.61%) Tonga (N = 113 - 10.32%) Senga (N = 100 - 9.13%) Mambwe (N = 71 - 6.48%) Lozi (N = 47 - 4.29%) Ngoni (N = 31 - 2.83%) Ndebele (N = 17 - 1.55%) |
Number of alters of ethnicity different from ego (external ties) minus the number of alters of the same ethnicity as ego (internal ties), divided by the total number of alters. All re- spondents mentioned only one ethnic group per alter. |
|
One or more sexual partners are migrant workers |
Is [alter] a migrant worker? |
Yes (N = 209 - 19.09%) No (N = 843 - 76.99%) I don’t know (N = 48 - 4.38%) |
One or more sexual partners (i.e., alters with whom ego has sexual relationships sometimes or always) identified as migrant workers |
|
Euclidean distance between ego’s and sexual partners’ age |
How old is [alter]? |
Age in years |
For each alter identified as a sexual partner (i.e., an alter with whom ego has sexual relationships sometimes or always), we obtain the mean of squared differences between ego’s age and each alters’ age. |
|
Alter-alter ties |
|||
|
Network density |
Think about the relationship between [alter] and [alter]. Which of the following would describe how they know one another? |
Friends Relatives Know each other ONLY be- cause they know me Work together Know each other by name Know each other by sight Do not know each other |
Number of ties out of possible ties. We do not distinguish be- tween types of ties because ex- ploratory analyses revealed the number of ties per type of tie are very similar for HIV-posi- tive and HIV-negative egos. |
Analytical Strategy
In this exploratory study, we started by identifying associations between the dependent variable (ego HIV status) and six sets of independent variables, grouped according to the six categories pre- viously described. To identify associations, we conducted bivari- ate tests between ego HIV status and each independent variable individually. Test statistics included the Wilcoxon-Mann-Whitney test for interval or ordinal variables and chi-square test for cate- gorical variables.
We conducted logistic regression analyses to assess the relation- ship between predictors and ego HIV status when multiple vari- ables were included in the same model. Because bivariate analyses of the relationships between predictors suggested the presence of collinearity, we did not include all predictors in the logistic regres- sion models [35]. To reduce multicollinearity and promote a par- simonious specification, we narrowed the set of predictors based on: (1) the magnitude of the observed differences in the variable by ego HIV status (using the bivariate tests mentioned above); and (2) the variable’s substantive relevance as suggested from previous empirical work.
We fitted logistic regression models using a sequential approach, wherein we examined the association between five sets of vari- ables (e.g., ego sociodemographic characteristics, main partner characteristics) and ego HIV status separately to assess relation- ships when other types of variables were excluded from the model. Final models included independent variables from all five sets to assess the unique contribution of each variable with all other sets of predictors present in the model. Two variables strongly associ- ated with ego HIV status were collinear (number of alters to whom ego has disclosed her HIV status and number of HIV-positive or HIV-unknown alters). Therefore, we fitted two final regression models reported here, each including one of the two collinear vari- ables and all other independent variables. We displayed all logistic regression analysis results using odds ratios (ORs) and 95% con- fidence intervals. We also calculated variance inflation factors for every model to identify any remaining issues of multicollinearity
Results
Of the 219 women enrolled, 69 (31.5%) were HIV-positive and 150 (68.5%) were HIV-negative. All participants nominated five men as alters, for a total of 1095 alters. Table 1 presents sample characteristics by ego HIV status and in the whole sample. The mean age of the participants was 26, over 90% of women iden- tified as either Nyanja or Bemba, 56% had some schooling, and 36% were financially dependent on their main partner.
Bivariate Results
Table 1 presents bivariate associations between predictors and ego HIV status. Results indicate HIV-positive egos were, on average, older than HIV-negative egos. In addition, the main partners of HIV-positive egos were more likely to consume alcohol before sex. HIV-positive egos tended to disclose their HIV status to fewer alters compared with HIV-negative egos. HIV-positive egos had fewer alters with whom they had daily interactions and tended to have more alters who were HIV-positive or whose HIV status was unknown. The networks of HIV-positive egos tended be more het- erophilous in terms of ethnicity. Finally, HIV-positive egos tended to be more dissimilar to their sexual partners in terms of age when compared to HIV-negative egos.
Table 1: Bivariate Differences between HIV-positive and HIV-negative egos
|
|
Overall |
HIV Positive |
HIV Negative |
p-value* |
||||
|
N/Mean |
Proportion |
N |
Proportion/ Mean |
N |
Proportion/ Mean |
|||
|
Total |
219 |
100% |
69 |
31.51% |
150 |
68.49% |
|
|
|
Sociodemographic characteristics |
|
|
|
|
|
|
|
|
|
Ego age |
26.45 |
|
|
28.1 |
|
25.7 |
0 |
** |
|
Ego ethnicity |
|
|
|
|
|
|
|
|
|
Bemba |
77 |
35.16% |
22 |
31.88% |
55 |
36.67% |
0.48 |
|
|
Nyanja |
121 |
55.25% |
42 |
60.87% |
79 |
52.67% |
|
|
|
Other |
21 |
9.59% |
5 |
7.25% |
16 |
10.67% |
|
|
|
Ego level of education |
|
|
|
|
|
|
|
|
|
No schooling |
42 |
19.18% |
18 |
26.09% |
24 |
16.00% |
0.19 |
|
|
Some schooling |
124 |
56.62% |
38 |
55.07% |
86 |
57.33% |
|
|
|
Completed secondary school |
51 |
23.29% |
13 |
18.84% |
38 |
25.33% |
|
|
|
Ego depends financial- ly on partner |
79 |
36.07% |
29 |
42.03% |
50 |
33.33% |
0.310 |
|
|
Main partner charac- teristics |
|
|
|
|
|
|
|
|
|
Main partner is em- ployed |
137 |
62.56% |
42 |
60.87% |
95 |
63.33% |
0.66 |
|
|
Main partner has been circumcised |
153 |
69.86% |
28 |
40.58% |
73 |
48.67% |
0.510 |
|
|
Relationship between ego and main partner |
|
|
|
|
|
|
|
|
|
Main partner disclosure of HIV status to ego |
163 |
74.43% |
47 |
68.12% |
116 |
77.33% |
0.25 |
|
|
Main partner uses con- dom during vaginal sex |
103 |
47.03% |
37 |
53.62% |
66 |
44.00% |
0.24 |
|
|
Main partner consumes alcohol before sex |
62 |
28.31% |
27 |
39.13% |
35 |
23.33% |
0.02 |
* |
|
Ego trusts main partner |
1.56 |
|
|
1.32 |
|
1.66 |
0.11 |
|
|
Alter-ego tie variables |
|
|
|
|
|
|
|
|
|
One or more relatives |
130 |
59.36% |
35 |
50.72% |
95 |
63.33% |
0.11 |
|
|
Number of alters fa- thers of ego’s children |
0.34 |
|
|
0.38 |
|
0.33 |
0.95 |
|
|
Mean frequency of contact |
3.40 |
|
|
3.28 |
|
3.46 |
0.08 |
|
|
Number of alters with whom ego has daily interactions |
1.50 |
|
|
1.28 |
|
1.60 |
0.01 |
* |
|
Support (sum of advice and financial support scores) |
1.42 |
|
|
1.45 |
|
1.41 |
0.63 |
|
|
Number of alters to whom ego has dis- closed HIV status |
2.15 |
|
|
1.66 |
|
2.37 |
0 |
** |
|
Number of “some- times” sexual partners |
0.42 |
|
|
0.46 |
|
0.40 |
0.180 |
|
|
Alter attributes |
|
|
|
|
|
|
|
|
|
Number of HIV-posi- tive or HIV-unknown alters |
2.93 |
|
|
3.99 |
|
2.45 |
<0.001 |
*** |
|
E-I based on ethnicity |
0.23 |
|
|
0.40 |
|
0.16 |
0.01 |
** |
|
One or more sexual partners are migrant workers |
60 |
27.40% |
16 |
23.19% |
44 |
29.33% |
0.43 |
|
|
Euclidean distance be- tween ego’s and sexual partners’ age |
5.82 |
|
|
6.53 |
|
5.48 |
0.04 |
* |
|
Alter-alter ties |
|
|
|
|
|
|
|
|
|
Network density |
0.47 |
|
|
0.44 |
|
0.48 |
0.28 |
|
* Wilcoxon-Mann-Whitney test statistic was calculated for interval or ordinal variables; Chi-square test was calculated for categorical variables. *p < 0.05; ** p < 0.01; ***p < 0.001
Logistic Regression Models
Table 2 presents results from logistic regression models on ego HIV status. Models 1-5 show results from separate regression models for each of five sets of variables in the study. Models 6a and 6b are final models. Model 6a includes number of HIV-positive or HIV-unknown alters and excludes number of alters to whom ego had disclosed her HIV status. Model 6b includes number of alters to whom ego had disclosed her HIV status and excludes number of HIV-positive or HIV-unknown alters.
Results shown in Table 2 indicate consistency in the magnitude, direction, and confidence intervals for most estimates across mod- els. We centred our description of results on the associations with the lowest observed p-values. Results indicated that as ego age increased, so too did the estimated odds of being HIV-positive (OR = 1.09, p < 0.01; Model 1). Nonetheless, the relationship between ego age and being HIV-positive did not attain statistical signifi- cance in the full models. That the ego ages did not attain statistical significance in the full models was not surprising: ego ages’ ORs were close to 1.00 across models and the increase of parameters in the full model resulted in a loss of precision.
Findings shown in Table 2 also suggest women whose main part- ners consumed alcohol before sex were more than twice as likely to be HIV-positive compared to women whose main partners did not consume alcohol before sex (OR = 2.20, p < 0.05, Model 3; and OR = 2.25, p < 0.05, Model 6b). Main partner’s alcohol con- sumption did not remain statistically significant in the full model that included number of HIV-positive or HIV-unknown (Model 6a). However, the magnitude, direction and confidence intervals for main partner’s alcohol consumption were approximate across models. Figure 1, Panel A presents the predicted probability (es- timated using Model 6b) of being HIV-positive when ego’s main partner consumed and did not consume alcohol before sex. Women whose main partners consumed alcohol before sex had a predicted probability of being HIV-positive of 56.3%, holding other vari- ables at their means or reference categories. Meanwhile, women whose main partners did not consume alcohol before sex had a predicted probability of being HIV-positive of 36.3%, holding oth- er variables at their means or reference categories.
Our findings also provide evidence of a negative association be- tween the number of alters to whom ego disclosed her HIV status and being HIV-positive: the more alters cognizant of ego HIV sta- tus, the smaller the odds of ego being HIV-positive (OR = 0.72, p < 0.01, Model 4; and OR = 0.66, p < 0.01, Model 6b). Figure 1, Panel B plots the predicted probability, estimated using Model 6b, of being HIV-positive as the number of alters to whom ego disclosed her HIV status increased. Women who had not disclosed their HIV status to any of them alters had a predicted probability of being HIV-positive equal to 57.5%, holding all other variables at their means or reference categories. By contrast, the probability of being HIV-positive was 15.4% for women who had disclosed their HIV status to all five of their nominated alters, holding all other variables at their means or reference categories.
Finally, we observed increases in the odds of being HIV-positive for egos with a greater number of HIV-positive or HIV-unknown alters (OR = 2.22, p < 0.001, Table 2, Model 1; and OR = 2.30, p < 0.001, Model 6a). Figure 1, Panel C shows predicted probabilities (using Model 6a) of being HIV-positive at different numbers of alters who are HIV-positive or HIV-unknown, while holding all other variables at their means or reference categories. The predict- ed probability of being HIV-positive was 3.8% for women with five HIV-negative alters compared to 71.7% for women with five HIV-positive or HIV-unknown alters, holding all other variables at their means or reference categories.
Table 2: Logistic regression of HIV Status On Ego and Network Characteristics
|
|
Model 1 |
Model 2 |
Model 3 |
Model 4 |
Model 5 |
Model 6a |
Model 6b |
|
|
Esti mate (95% CI) |
Estimate (95% CI) |
Estimate (95% CI) |
Estimate (95% CI) |
Estimate (95% CI) |
Estimate (95% CI) |
Estimate (95% CI) |
|
Ego Sociodemographics |
|
|
|
|
|
|
|
|
Ego age |
1.09 (1.03 - 1.16)** |
|
|
|
|
1.05 (0.98 - 1.14) |
1.07 (1.00 - 1.15) |
|
Ego level of education (reference: No school) |
|||||||
|
Some schooling |
0.54 (0.25 - 1.16) |
|
|
|
|
0.75 (0.29 - 1.98) |
0.57 (0.23 - 1.41) |
|
Completed secondary school |
0.43 (0.17 - 1.06) |
|
|
|
|
0.49 (0.16 - 1.49) |
0.52 (0.18 - 1.47) |
|
Ego depends financially on partner |
1.24 (0.66 - 2.29) |
|
|
|
|
1.00 (0.46 - 2.12) |
0.85 (0.41 - 1.74) |
|
Main partner characteristics |
|
|
|
|
|
|
|
|
Main partner has been circumcised |
|
0.78 (0.42 - 1.42) |
|
|
|
0.80 (0.38 - 1.68) |
0.88 (0.44 - 1.77) |
|
Relationship between ego and main partner |
|
|
|
|
|
|
|
|
Main partner consumes alcohol before sex |
|
|
2.20 (1.18 - 4.09)* |
|
|
2.18 (1.00 - 4.82) |
2.25 (1.07 - 4.76)* |
|
Alter-ego tie variables |
|
|
|
|
|
|
|
|
Number of alters to whom ego has dis- closed HIV status |
|
|
|
0.72 (0.58 - 0.89)** |
|
|
0.66(0.51 - 0.85)** |
|
Alter attributes |
|||||||
|
Number of HIV-positive or HIV-un- known alters |
|
|
|
|
2.22 (1.73 - 2.94)*** |
2 . 3 0 (1.75 - 3.14)*** |
|
|
One or more sexual partners who migrant workers |
|
|
|
|
0.57 (0.27 - 1.18) |
0.68 (0.29 - 1.55) |
0.79 (0.34 - 1.75) |
|
Constant |
0.07 (0.01 - 0.36)** |
0.49 (0.32 - 0.74)*** |
0.35 (0.24 - 0.50)*** |
0.85 (0.52 - 1.39) |
0.04 (0.01 - 0.10)*** |
0 . 0 1 (0.00 - 0.10)*** |
0.23 (0.03 - 1.76) |
|
N |
215 |
201 |
216 |
208 |
219 |
194 |
184 |
|
Null deviance |
269.85 |
246.74 |
267.52 |
256.77 |
272.92 |
238.36 |
222.73 |
|
Residual deviance |
256.03 |
246.08 |
261.33 |
246.92 |
221.22 |
181.45 |
200.77 |
Notes: Results presented in odds ratios. Variance inflation factors (VIF) were calculated to determine the presence of moderate multicol- linearity. All VIFs were below 1.5. *p < 0.05; ** p < 0.01; ***p < 0.001
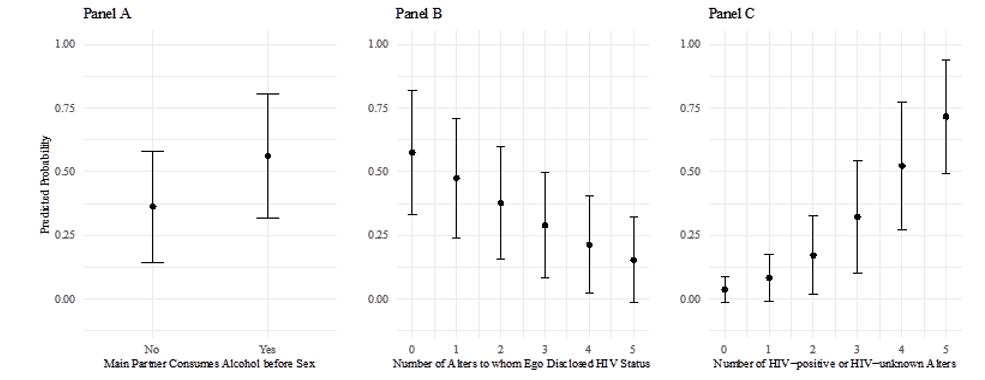
Figure 1: Predicted probabilities and 95% prediction intervals of being HIV-positive as a function of three variables: main partner alcohol consumption (Panel A), number of alters to whom ego has disclosed her HIV status (Panel B), and number of alters that are HIV-positive or HIV-unknown (Panel C). For each panel, all other variables are set at either their means (for continuous variables) or reference categories (for categorical variables). All predicted probabilities are estimated from full models. We use Model 6b in Table 2 for panels A and B and Model 6a in Table 2 for panel C.
Discussion
Our findings reveal differences in known HIV risk and protec- tive factors between HIV-negative and HIV-positive pregnant and breastfeeding women. Protective factors including higher educa- tion, partner circumcision and disclosure of HIV status to part- ners were higher in HIV-negative women. However, risk factors including sex partners who are migrant workers, condom less and dry sex, a belief that partners have sex with men and lack of trust in partner were high in HIV-negative women. Condom use was low among all the women in this study and there was no significant association between education or sexual partners outside marriage and condom use (see Table S2 of supplemental data). In Zambia a number of factors resulting from gender inequity make it diffi- cult for women to insist on condom use and may contribute to the low condom use found in our study [36]. Additionally, the social norm that condom use is considered unnecessary within marriage or when a woman is pregnant may also have influenced this result. The risk of HIV acquisition among the sexual partners of HIV-pos- itive study participants was potentially exacerbated due to the lack of HIV status disclosure and the use of alcohol during sex observed in this cohort. Previous studies in SSA have shown a low rate of disclosure of HIV serostatus to sexual partners and decreased con- dom use among users of alcohol [37]. HIV-positive participants in our study reported stigma associated with their serostatus as evidenced by lower rates of disclosure of HIV status, fewer men who were relatives within their networks and more diversity in partners’ ethnicity (meaning they chose sexual partners outside of their own tribe). Other studies in the region have also shown that HIV-positive women are more likely to choose to have sexual part- ners outside of their community in order to preserve their social capital and to reduce HIV-related stigma [38-40].
In Zambia, high levels of gossip within a community have been found to decrease male testing rates for fear of community rejec- tion [36]. Our study site was located at a level 1 hospital within a compound, where the community interact daily and rely upon one another for work, water and food, and our findings of non-disclo- sure of HIV status may reflect fear of being ostracised from the community.
Within the egocentric networks of both HIV-positive and HIV-neg- ative participants, non-disclosure of HIV status was predominant. Similar to other studies in the region, concern regarding negative consequences linked to HIV disclosure (violence, abandonment, loss of social capital or income) may have been barriers to disclo- sure. Women who had disclosed their HIV status had reduced odds of being HIV-positive suggesting that finding ways to encourage women to disclose their HIV status will lead to positive health out- comes. Disclosure may be particularly crucial for pregnant wom- en. During pregnancy, women are at considerably increased risk for HIV acquisition (male-to-female) and transmission (female- to-male). Without partner support, it is often difficult for women to adhere to recommended HIV treatment and breastfeeding regi- mens, behaviours that are necessary to reduce transmission of HIV to their infants, protect their own health, and ensure the health of their partner [41,42].
Limitations
These findings must be interpreted within the context of the study’s limitations. First, participants were recruited solely from one clinic and may not represent pregnant and breastfeeding women residing in other regions. Residential instability is common among wom- en in Zambia, making residential sampling challenging, and often convenience sampling at ANC clinics serving pregnant women is the only viable way to collect data from this population. Second, although we conducted a thorough literature review there may be domains that effect HIV risk and prevention that were missing. Third, due to the early closure of the study due to COVID-19 pan- demic, the recruitment of HIV-positive women was lower than the HIV-negative group. It is possible there are greater differences be- tween the groups than found in this study, a larger sample size may have revealed previously unobserved differences. Fourth, while the original study design included qualitative interviews to explore further the findings from the surveys, it was not possible to com- plete this portion of the study due to early closure. The qualitative study may have provided depth to understanding reasons why this cohort did not disclose their HIV status. Finally, data on alter be- haviours and HIV status relied on the ego’s perspective, a method used when, as in this case, the alters are difficult to access.
Conclusions
In an era of the Undetectable = Untransmissable (U=U) campaign and pre-exposure prophylaxis (PrEP), ways to assist women with safe disclosure of HIV status may improve not only their own health, but also the health of their partners and infants. Given the many obstacles to obtaining information to influence behaviour change, there is value in understanding both the prevention and risk potential within egocentric networks to inform efforts to de- sign and implement behaviour change interventions. This study provides some evidence that non-disclosure of HIV status occurs among the networks of both HIV-negative and HIV-positive pregnant and breastfeeding women. Further research is needed to in- form strategies to improve HIV disclosure within complex social networks.
Funding
This work was supported by the Fogarty International Centre and the National Institute of Nursing Research (D43 TW009340). Ad- ditional support was provided by the National Institute of Allergy and Infectious Diseases (K24 AI120796, R01 AI131060) and Eu- nice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), NIH, through Grant Award Number R25 HD079352 to Duke University.
Acknowledgement
Dana K Pasquel is supported by Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), NIH, through Grant Award Number R25 HD079352 to Duke University.
References
- Teasdale CA, Abrams EJ, Chiasson MA, Justman J, Blanchard K, et al. (2017) Sexual Risk and Intravaginal Practice Behav- ior Changes During Pregnancy. Arch Sex Behav 46: 539-548.
- World Health Organization (2016) Global Health Sector Strat- egy on HIV 2016–2021 Towards Ending AIDS. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/246178/ WHO-HIV-2016.05-eng.pdf?sequence=1
- World Health Organization (2017) Global guidance on criteria and processes for validation: elimination of mother-to-child transmission of HIV and syphilis, (2nd edition. ed. Vol. Li- cence: CC BY-NC-SA 3.0 IGO). Geneva.
- Lewis R, Mitchell KR, Mercer CH, Datta J, Jones KG, et al. (2020) Navigating new sexual partnerships in midlife: a so- cioecological perspective on factors shaping STI risk percep- tions and practices. Sex Transm Infect 96: 238-245.
- Mugo NR, Heffron R, Donnell D, Wald A, Were EO, et al. (2011) Increased risk of HIV-1 transmission in pregnancy: a prospective study among African HIV-1-serodiscordant cou- ples. AIDS 25: 1887-1895.
- Ngoma C, Roos J, Siziya S (2016) Exploring Sexual Behaviour of Women in Zambia: A Qualitative Study. British Journal of Education, Society & Behavioural Science 12: 1-19.
- AVERT (2018) Global information and education on HIV and AIDS. Retrieved from https://www.avert.org/professionals/ hiv-around-world/sub-saharan-africa/zambia
- Hatzold K, Gudukeya S, Mutseta MN, Chilongosi R, Na- lubamba M, et al. (2019) HIV self-testing: breaking the barriers to uptake of testing among men and adolescents in sub-Saharan Africa, experiences from STAR demonstration projects in Malawi, Zambia and Zimbabwe. J Int AIDS Soc 22: e25244.
- UNAIDS (2018) Miles to Go - Closing Gaps, Breaking Barri- ers, Righting Injustices. Retrieved from Geneva, Switzerland.
- Tedeschi JT (2017) The social influence processes: Routledge.
- Asrese K, Mekonnen A (2018) Social network correlates of risky sexual behavior among adolescents in Bahir Dar and Mecha Districts, North West Ethiopia: an institution-based study. Reproductive Health 15: 61.
- Meisel MK, Clifton AD, MacKillop J, Goodie AS (2015) A social network analysis approach to alcohol use and co-occur- ring addictive behavior in young adults. Addictive Behaviors 51: 72-79.
- Meisel MK, Clifton AD, Mackillop J, Miller JD, Campbell WK, et al. (2013) Egocentric social network analysis of pathological gambling. Addiction 108: 584-591.
- Clare Barrington, Carl Latkin, Michael D Sweat, Luis More- no, Jonathan Ellen, et al. (2009) Talking the talk, walking the walk: social network norms, communication patterns, and condom use among the male partners of female sex workers in La Romana, Dominican Republic. Soc Sci Med 68: 2037- 2044.
- King KM, Latkin CA, Davey-Rothwell MA (2015) Love on lockdown: how social network characteristics predict sepa- rational concurrency among low income African-American women. J Urban Health 92: 460-471.
- Doherty IA, Serre ML, Gesink D, Adimora AA, Muth SQ, et al. (2012) Sexual networks, surveillance, and geographical space during syphilis outbreaks in rural North Carolina. Epi- demiology 23: 845-851.
- Kharsany AB, Karim QA (2016) HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportu- nities. Open AIDS J 10: 34-48.
- Kinuthia J, Drake AL, Matemo D, Richardson BA, Zeh C, et al. (2015) HIV acquisition during pregnancy and postpartum is associated with genital infections and partnership character- istics. AIDS 29: 2025-2033.
- Colvin CJ (2019) Strategies for engaging men in HIV ser- vices. The Lancet HIV 6: e191-e200.
- Amirkhanian YA (2014) Social networks, sexual networks and HIV risk in men who have sex with men. Curr HIV/AIDS Rep 11: 81-92.
- Neblett RC, Davey-Rothwell M, Chander G, Latkin CA (2011) Social network characteristics and HIV sexual risk behavior among urban African American women. J Urban Health 88: 54-65.
- Balkus JE, Gonasagrie Nair, Montgomery ET, Mishra A, Palanee-Phillips T, et al. (2015). Age-disparate partnerships and risk of HIV-1 acquisition among south african women participating in the VOICE trial. J Acquir Immune Defic Syn- dr 70: 212-217.
- Davey-Rothwell MA, Latimore A, Hulbert A, Latkin CA (2011) Sexual networks and housing stability. J Urban Health 88: 759-766.
- Adrian Dobra, Till Bärnighausen, Alain Vandormae, Frank Tanser (2017) Space-time migration patterns and risk of HIV acquisition in rural South Africa. AIDS 31: 137-145.
- Joseph Davey D, Farley E, Gomba Y, Coates T, Myer L (2018) Sexual risk during pregnancy and postpartum periods among HIV-infected and -uninfected South African women: Impli- cations for primary and secondary HIV prevention interven- tions. PLoS One 13: e0192982.
- M’Soka NC, Mabuza LH, Pretorius D (2015) Cultural and health beliefs of pregnant women in Zambia regarding preg- nancy and child birth. Curationis 38: 1232.
- Omori R, Chemaitelly H, Abu-Raddad LJ (2015) Dynamics of non-cohabiting sex partnering in sub-Saharan Africa: a modelling study with implications for HIV transmission. SexTransm Infect 91: 451-457.
- Owen BN, Elmes J, Silhol R, Dang Q, McGowan I, et al. (2017) How common and frequent is heterosexual anal inter- course among South Africans? A systematic review and me- ta-analysis. J Int AIDS Soc 19: 21162.
- Popova S, Lange S, Probst C, Gmel G, Rehm J (2017) Esti- mation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: a system- atic review and meta-analysis. The Lancet Global Health 5: e290-e299.
- Hensen B, Taoka S, Lewis JJ, Weiss HA, Hargreaves J (2014) Systematic review of strategies to increase men’s HIV-testing in sub-Saharan Africa. AIDS (London, England) 28: 2133- 2145.
- Kayukwa A, Butts SA, Barylski NA, Alcaide ML, Rodriguez VJ, et al. (2019) HIV Prevention among Zambian Itinerant Workers: Challenges and Solutions. J Health Care Poor Un- derserved 30: 358-377.
- Bhatnagar T, Brown J, Saravanamurthy PS, Kumar RM, De- tels R (2013) Color-coded audio computer-assisted self-inter- views (C-ACASI) for poorly educated men and women in a semi-rural area of South India: “good, scary and thrilling”. AIDS Behav 17: 2260-2268.
- Kurth AE, Martin DP, Golden MR, Weiss NS, Heagerty PJ, et al. (2004) A Comparison Between Audio Computer-Assist- ed Self-Interviews and Clinician Interviews for Obtaining the Sexual History. Sexually Transmitted Diseases 31: 719-726.
- Macalino GE, Celentano DD, Latkin C, Strathdee SA, Vla- hov D (2002) Risk Behaviors by Audio Computer-Assisted Self-Interviews among HIV-Seropositive and HIV-Seroneg- ative Injection Drug Users. AIDS Education and Prevention 14: 367-378.
- Perry BL, Pescosolido BA, Borgatti SP (2018) Egocentric Network Analysis: Foundations, Methods, and Models. Cam- bridge: Cambridge University Press.
- Gari S, Malungo JRS, Martin-Hilber A, Musheke M, Schin- dler C, et al. (2013) HIV Testing and Tolerance to Gender Based Violence: A Cross-Sectional Study in Zambia. PLoS One 8: e71922.
- Ferreira-Borges C, Charles D H Parry, Babor TF (2017) Harmful Use of Alcohol: A Shadow over Sub-Saharan Africa in Need of Workable Solutions. International Journal of Envi- ronmental Research and Public Health 14: 346.
- Mukoswa GM, Charalambous S, Nelson G (2017) The asso- ciation between social capital and HIV treatment outcomes in South Africa. PLoS One 12: e0184140.
- Pronyk PM, Harpham T, Busza J, Phetla G, Morison LA, et al. (2008) Can social capital be intentionally generated? A randomized trial from rural South Africa. Social Science & Medicine 67: 1559-1570.
- Wouters E, Meulemans H, Van Rensburg HCJ (2009) Slow to share: social capital and its role in public HIV disclosure among public sector ART patients in the Free State province of South Africa. AIDS Care 21: 411-421.
- C Jasseron, L Mandelbrot, C Dollfus, N Trocmé, R Tubiana, et al. (2013) Non-disclosure of a pregnant woman’s HIV sta- tus to her partner is associated with non-optimal prevention of mother-to-child transmission. Multicenter Study, AIDS Behav17: 488-497.
- Walcott MM, Hatcher AM, Kwena Z, Turan JM (2013) Facili- tating HIV status disclosure for pregnant women and partners in rural Kenya: a qualitative study. BMC Public Health 13: 1115.