
Archivos de Ciencia e Investigación(ADCI)
ISSN: 3068-014X | DOI: 10.33140/ADCI

Research Article - (2026) Volume 2, Issue 1
Efficacy of Short-Term Versus Long-Term Radiotherapy in Rectal Cancer: A Frisbee-Based Meta-Analysis (A Friendly Evidence-Based Review of The Literature)
2G. Jazzolino Hospital, Vibo Valentia, Calabria, Italy
3Magna Graecia University, Catanzaro, Italy
Received Date: Sep 06, 2025 / Accepted Date: Nov 24, 2025 / Published Date: Jan 23, 2026
Copyright: ©2026 Gustavo Gomez Barbieri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Barbieri, G. G., Petracca, G., Capomolla, A. (2026). Efficacy of Short-Term Versus Long-Term Radiotherapy in Rectal Cancer: A Frisbee-Based Meta-Analysis (A Friendly Evidence-Based Review of The Literature). Arch Cienc Investig, 2(1), 01-06.
Abstract
Introduction Rectal cancer is the second most common cancer in Italy, with nearly 50,000 cases expected by 2024. Given the high cost and quality of life for its families, its mortality rate is low, ranging from 5 to 7% in the early stages too high in the advanced stages, with a mortality rate of 90%.
Methods A search was conducted in Epistemonikos, the largest database of systematic reviews in the healthcare field, maintained by screening multiple sources of information, including MEDLINE, EMBASE, and Cochrane, among others. Data were extracted from the identified reviews, data from the primary studies were analyzed, a meta-analysis was performed, and a summary table of the results was prepared using the GRADE method.
Results and Conclusions Six systematic reviews were identified, which together include thirty-seven primary studies, of which 37 correspond to randomized trials. It was concluded that the use of short-term IMRT plus immediate chemotherapy compared to neoadjuvant chemotherapy, surgery, and radiotherapy increases local control and disease-free survival and reduces complications and the need for surgery compared to long-term radiotherapy, with a high degree of evidence.
Keywords
RAP, TME, LAR, Opthra Protocol, Long-Term Survival Protocol, Rectal Cancer, IMRT Radiotherapy, Hospitalization, Epistemonikos, GRADE
Problem
Rectal cancer is the third most common cancer with the highest incidence and mortality worldwide and the first in terms of years of life lost. (Globocan, 2020) A study in medical history reveals the first wide abdominoperineal resection (RAP), which later became more common, followed by low anterior resection (LAR). More recently, the emphasis on TME (half-rectal transection) has significantly improved locoregional disease control rates thanks to en bloc resection of the mesorectum, which contains the perirectal lymph nodes, the first level of drainage of the rectal lymph nodes. (Khullar, 2022) Beginning in the 1970s, the first clinical trial evaluating local control and recurrence for surgery alone, surgery plus chemotherapy, radiotherapy plus chemotherapy, and radiotherapy plus surgery demonstrated that surgery and radiotherapy provided greater local control and subsequently improved overall patient survival. It was with the advent and improvement in the application of 2D radiotherapy concurrent with surgery that disease-free survival, as well as overall survival, improved. Sauer, in 2004, demonstrated that the combination of chemotherapy, surgery, and 2D radiotherapy in a long-term regimen improved local control but not overall survival. This paradigm has remained entrenched in clinical practice for the past 20 years.
Nowadays, with the advent of next-generation sequencing techniques and the genetic study of colorectal cancers, several drug targets and tumor markers have been discovered, which have made it possible to recognize genetic models of these tumors such as hereditary tumors such as familial adenomatous polyposis (FAP) due to mutations in the gene that regulates the degradation of beta-catenin and overexpression of the wnt-frizzled pathway causing the appearance of hundreds of polyps in the colon and Lynch syndrome explained by the Knudson double-hit theory where there are mutated genes acquired as hereditary, causing the development of multiple breast, ovarian and prostate tumors in multiple relatives.
Even in this 10% of cases, therefore, the new therapy will focus on gene therapy and immunotherapy, as well as the development of molecular scissors, gene editing, and genetic tweezers that modulate the expression and silence the activity of gene families through histone methylation and demethylation, which epigenetically regulate rectal cancer. Hereditary factors have been identified in these 20% of rectal cancers, and in the remaining 70%, risk factors such as alcohol, tobacco, a lack of plant-based diets, high salt and dried meat consumption, and lack of physical activity explain the development of these diseases, as well as ulcerative colitis and Crohn’s disease. Therefore, now more than ever, it is necessary to develop new therapies that involve not only the resection and treatment of a highly preventable disease with a high disease burden, but also the development of genetic vaccines that prevent the spread and persistence of this disease. Radiotherapy, chemotherapy, and surgery must evolve into a personalized, comprehensive precision medicine therapy that covers all variants of this set of diseases, which include cancer. Colorectal cancer, and in this case, rectal cancer.
In recent years, this clinical protocol, the cornerstone of treatment, has been questioned, with claims that it does not improve patient outcomes. On the contrary, IMRT radiotherapy technology contributes to improved dose fractionation and image resolution, optimizing planning, improving quality, and reducing complications and patient mortality.
Methods
We conducted a search in Epistemonikos, the largest database of systematic reviews in healthcare, which is maintained by searching multiple sources of information, including MEDLINE, EMBASE, Cochrane, and others. We extracted data from the identified reviews and analyzed data from the primary studies. With this information, we generated a structured summary called FRISBEE (Friendly Summaries of Body of Evidence using Epistemonikos), following a predefined format. This summary includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analyses of the total studies where possible, a GRADE summary table of results, and a section on other considerations for decision-making.

Regarding the body of evidence for this question
|
What is the evidence? See evidence matrix in Epistemonikos below. |
We found six systematic reviews [4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] that collectively included 37 primary studies addressing the clinical question, 37 of which were randomized controlled trials. This table and the summary in general are based on these latter studies, since observational studies did not increase the certainty of the existing evidence or provide any additional relevant information. |
|
What type of patients did the studies include?* |
All trials included patients with T2 to T4 rectal cancer, diagnosed clinically, by colonoscopy, and by magnetic resonance imaging (MRI) with computed tomography (CT) and/or positron emission tomography (PET). All patients included were over 18 years of age [15][16]. The age range in one trial was 48–79 years [15], while in the other, the mean age was 60.56 years [16].
Patients with a diagnosis or suspicion of other diseases on CT, such as colon cancer and inflammatory bowel disease, were excluded. One trial included patients with a history of previous acute diverticulitis [15]. |
|
What types of interventions did the studies include?* |
One trial used the intervention of administering 25 Gy IMRT in 5 short-course sessions without delay to chemotherapy or the need for surgery. The Stockholm III trial included an intervention with and without a 5- to 6-week delay to chemotherapy [15].
The other trial used the intervention of administering 60 Gy IMRT in 15 fractions followed by surgery and chemotherapy with a 6-week delay [16].
For comparison, both trials used one treatment, chemotherapy alone, surgery alone, and IMRT regimens with and without delay [15]. Trials using brachytherapy or comparing surgery with radiotherapy or chemotherapy alone were excluded from this study [16]. |
|
What kind of outcomes did they me |
The outcomes measured were as follows: Overall survival Local recurrence Local control Quality of life
Follow-up in both trials was 5.5 years[15][16]. |
|
Effectiveness of short versus long radiotherapy regimen in patients with locally advanced rectal cancer |
|||||
|
Patients Pacientes en tratamiento por cáncer de recto localmente avanzado T2-T3 Y T4 Intervention Radioterapia Comparison Radioterapia de esquema corto versus largo |
|||||
|
Desenlaces |
Absolut effect * |
Efecto relativo (IC 95%) |
Certeza de la evidencia (GRADE) |
||
|
RT SC |
RT LC |
||||
|
Difference: patie 1000 |
|||||
|
Overall Survival (5 years) |
362 per 1000 |
333 per 1000 |
RR 0.97 (0.88 a 1.07) |
⊕⊕⊕⊕ Alta |
|
|
Difference: 29 más (26 less to 31 plus) |
|||||
|
Local recurrence (5 years)** |
79 per 1000 |
121 per 1000 |
RR 0.65 (0.47 a 0.88) |
⊕⊕⊕⊕ Alta |
|
|
42 less per 1000 (from 64 less to 15 less) |
|||||
|
Toxicity |
147 per 1000 |
150 per 1000 |
RR 0.94 (0.79 a 1.12) |
⊕⊕⊕1,2 MODERADA |
|
|
9 less per 1000 (de 31 menos a 18 más ) |
|||||
|
R0 resection rate |
886 per 1000 |
953 per 1000 |
RR 0,93 (0,81 a 1,07) |
⊕⊕ 1,2 MODERADA |
|
|
Diferencia: 67 less per 1000 ( 54 less to 72 plus) |
|||||
|
Overall Quality of life |
240 per 400 |
242 per 400 |
RR 0,99 (0,99 a 1,09) |
⊕ ⊕ oo¯ 1,2 Baja |
|
|
7 menos por 1000 (de 63 menos a 63 más) |
|||||
|
Margin of error: 95% confidence interval (95% CI).
RR: Relative risk. MD: Mean difference. GRADE: GRADE Working Group levels of evidence (see below).
*Risks/averages are based on the risks/averages of the control group in the studies. The risk/average (and its margin of error) is calculated from the relative effect/mean difference (and its margin of error).
|
|||||

|
Regarding the certainty of the evidence(GRADE)* |
|
High: The investigation has a very good indication of the probable effect. The probability that the effect will be substantially different is low.
Moderate: The investigation enters into a good indication of the probable effect. The probability that the effect will be substantially different is moderate.
Low: The investigation has some indication of the probable effect. Sin embargo, the probability that the effect will be substantially different is the same.
Well, the investigation does not involve a reliable estimate of the probable effect. The probability that the effect is substantially different is very high. |
|
*This is also referred to as ‘quality of evidence’ or ‘confidence in effect estimates’.
†Substantially different = a difference large enough to affect the decision. |
|
Otras consideraciones para la toma de decisión |
|
To whom does this evidence apply and to whom does it not apply? The results of this study apply to patients with T2 and T4 stage rectal cancer without metastasis, managed in an inpatient setting.
|
|
Regarding the outcomes included in this summary |
of life and toxicity were not reported in all the systematic reviews evaluated. |
|
Balance of risk/Benefits and certainly of evidence. |
|
|
Consideration of the recommendation |
|
Some systematic reviews analyzed in this summary mention that long-course versus short-course treatment may be equivalent.
than the long-course regimen. |
|
What do you think about patients and clinicians |
|
While there is considerable national debate about whether the short-course versus the long- course regimen should be used, evidence suggests that two clinical trials, including RAPIDO, achieve the same disease-free survival (DFS) as OPRA in patients with a much worse prognosis. Which, then, is the best treatment? In T4 tumors, OPRA has 11% versus RAPIDO 32% disease survival, OPRA 28%, RAPIDO 9%, OPRA 76%, and RAPIDO 76%. It's worth noting that RAPIDO has a 4.6-year follow-up period compared to OPRA's 3 years. Furthermore, RAPIDO randomized 912 patients, while OPRA randomized 324. There is no reason to choose the OPRA protocol over the RAPIDO protocol. |
|
Hospers, 2020. [28,30] |
|
Difference between this summary and another research. |
|
|
¿Can that change this information in the future? |
study this same clinical question within an outpatient setting. |
Table 1: Information on the Evidence Set for this Question
Summary of Evidence
Information Both studies measured local control, local recurrence, overall survival, quality of life (1,151 patients), and recurrence (1,110 patients) [15,16].
The summary of the results is as follows:
It is possible to clearly establish whether the use of short-course RT compared to long-course RT results in better local control (high certainty of evidence). The use of short-course RT may result in a slight improvement in quality of life or no difference in quality of life (low certainty of evidence); however, given the large heterogeneity between studies and measures, further evidence is needed to confirm this (low certainty of evidence). The use of short-course RT will result in better local control, disease-free survival, and less recurrence (high certainty of evidence). The use of the short-term Rt regimen presents lower toxicity than the long- term regimen, an essential pillar of the birth of this regimen (high certainty of the evidence).
How We do this Meta-Analysis
Using automated and collaborative methods, we collect all the evidence relevant to the question of interest and present it in an evidence matrix.
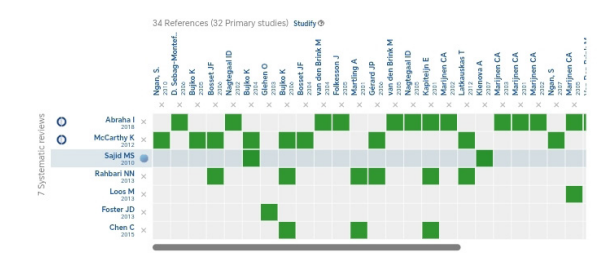
Follow the link to access the interactive version: Link to the relationship matrix from
http:/ /www.epistemonikos.org/matrixes/630fa7ab7d- b23a429db05042
If new systematic reviews on this topic are published after this summary is published, a “new evidence” alert will appear at the top of the matrix. While the project plans to update these summaries periodically, users are encouraged to comment on the Medwave website or contact the authors by email if they believe there is evidence justifying an earlier update.
After creating an Epistemonikos account, saving your matrices will automatically notify you whenever new evidence potentially answers this question.
This article is part of the Epistemonikos evidence synthesis project. It is prepared using a predefined methodology, following rigorous methodological standards and an internal peer review process. Each of these articles corresponds to a summary, called FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos)whose primary objective is to synthesize the body of evidence for a specific question in a format that is friendly to clinical professionals. Its main resources are based on the Epistemonikos evidence matrix and the analysis of results using the GRADE methodology.
The Epistemonikos Foundation is an organization that seeks to bring information closer to healthcare decision makers through the use of technology. Its main development is the Epistemonikos database ( www.epistemonikos.org ).
References
- Abraha, I., Aristei, C., Palumbo, I., Lupattelli, M., Trastulli, S., Cirocchi, R., ... & Valentini, V. (2018). Preoperative radiotherapy and curative surgery for the management of localised rectal carcinoma. Cochrane Database of Systematic Reviews, (10).
- Gastrointestinal Tumor Study Group. (1985). Prolongation of the disease-free interval in surgically treated rectal carcinoma. New England Journal of Medicine, 312(23), 1465-1472.
- Bujko, K. (2013). Short-course preoperative radiotherapy for low rectal cancer. J Clin Oncol, 31(14), 1799.
- Bosset JF, Collette L, Calais G, et al. Chemioterapia con radioterapia preoperatoria nel cancro del retto. N Engl J Med. 2006;355:1114–23
- Sauer, R., Becker, H., Hohenberger, W., Rödel, C., Wittekind, C., Fietkau, R., ... & Raab, R. (2004). Preoperative versus postoperative chemoradiotherapy for rectal cancer. New England Journal of Medicine, 351(17), 1731-1740.
- Sebag-Montefiore D, Stephens RJ, Steele R, et al. (2009) Radioterapia preoperatoria versus chemioradioterapia postoperatoria selettiva in pazienti con cancro del retto (MRC CR07 e NCIC-CTG C016): uno studio multicentrico randomizzato. Lancetta.373:811–20.
- Folkesson J, Birgisson H, Pahlman L, et al. (2005) Cancro del retto svedese REVISIONE ONCOLOGIA ED EMATOLOGIA51 Il ruolo in evoluzione della radioterapia nel cancro del retto localmente avanzato e il potenziale per uno studio di gestione non operatoria: benefici a lungo termine della radioterapia sulla sopravvivenza e sul tasso di recidiva locale. J Clin Oncol. 23:5644–50.
- van Gijn, W., Marijnen, C. A., Nagtegaal, I. D., Kranenbarg, E.M. K., Putter, H., Wiggers, T., ... & van de Velde, C. J. (2011). Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. The lancet oncology, 12(6), 575-582.
- Bujko K, Nowacki MP, Nasierowska-Guttmejer A, et al. (2006). Risultati a lungo termine di uno studio randomizzato che confronta la radioterapia preoperatoria a breve termine con la chemioradioterapia preoperatoria convenzionalmente frazionata per il cancro del retto. Fr. J Surg.93:1215–23.
- Ngan SY, Burmeister B, Fisher RJ, et al. (2012) Studio randomizzato di radioterapia a breve termine rispetto a chemioradioterapia a lungo termine confrontando i tassi di recidiva locale in pazienti con cancro del retto T3: studio Trans-Tasman Radiation Oncology Group 01.04. J Clin Oncol.30:3827–33.
- Bujko K, Wyrwicz L, Rutkowski A, et al. (2016). Chemioradioterapia preoperatoria a lungo termine a base di oxaliplatino rispetto a 5 × 5 Gy e chemioterapia di consolidamento per cancro del retto cT4 o cT3 fisso: risultati di uno studio randomizzato di fase III. Anna Oncol.27:834–42.
- Erlandsson J, Holm T, Pettersson D, et al. (2017). Frazionamento ottimale della radioterapia preoperatoria e timing dell’intervento chirurgico per il cancro del retto (Stoccolma III): uno studio multicentrico, randomizzato, non- in cieco, di fase 3, di non inferiorità. Lancetta Oncol.18:336–46.
- Zhu J, Gu W, Lian P, et al. (2013) Uno studio di fase II sulla chemioradioterapia neoadiuvante basata su IMRT seguita da un ciclo di capecitabina per l’adenocarcinoma rettale in stadio II/III. Radioterapia Oncol. 8:130.
- Gao, Y. H., Zhang, X., An, X., Cai, M. Y., Zeng, Z. F., Chen,G., ... & Ding, P. R. (2014). Oxaliplatin and capecitabine concomitant with neoadjuvant radiotherapy and extended to the resting period in high risk locally advanced rectal cancer.
- Foster, J. D., Jones, E. L., Falk, S., Cooper, E. J., & Francis, N.K. (2013). Timing of surgery after long-course neoadjuvant chemoradiotherapy for rectal cancer: a systematic review of the literature. Diseases of the colon & rectum, 56(7), 921-930.
- Maas, H. A. A. M., Lemmens, V. E. P. P., Nijhuis, P. H. A., De Hingh, I. H. J. T., Koning, C. C. E., & Janssen-Heijnen,M. L. G. (2013). Benefits and drawbacks of short-course preoperative radiotherapy in rectal cancer patients aged 75 years and older. European Journal of Surgical Oncology (EJSO), 39(10), 1087-1093.
- Rahbari, N. N., Elbers, H., Askoxylakis, V., Motschall, E., Bork, U., Büchler, M. W., ... & Koch, M. (2013). Neoadjuvant radiotherapy for rectal cancer: meta-analysis of randomized controlled trials. Annals of surgical oncology, 20(13), 4169- 4182.
- Bahadoer, R. R., Dijkstra, E. A., van Etten, B., Marijnen,C. A., Putter, H., Kranenbarg, E. M. K., ... & Silviera,M. L. (2021). Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. The Lancet Oncology, 22(1), 29-42.
- Garcia-Aguilar, J., Patil, S., Gollub, M. J., Kim, J. K., Yuval,J. B., Thompson, H. M., ... & Saltz, L. B. (2022). Organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. Journal of clinical oncology, 40(23), 2546-2556.
- Zhou, Z. R., Liu, S. X., Zhang, T. S., Chen, L. X., Xia, J., Hu,Z. D., & Li, B. (2014). Short-course preoperative radiotherapy with immediate surgery versus long-course chemoradiation with delayed surgery in the treatment of rectal cancer: asystematic review and meta-analysis. Surgical oncology, 23(4),211-221.
- Eitta,MA, El-Wahidi, GF, Fouda, MA, El-Hak, NG, Abo El-Naga, EM, Radioterapia preoperatoria nel cancro rettale resecabile: uno studio prospettico randomizzato di due diversi approcci, Journal of Egyptian National
- Marijnen, Ca, Nagtegaal, Id, Kranenbarg, Em, Putter, H, Wiggers, T, Rutten, Hj, Påhlman, L, Glimelius, B, Velde, Cj, Radioterapia preoperatoria combinata con escissione mesorettale totale per cancro del retto resecabile: Follow-up a 12 anni dello studio multicentrico, randomizzato e controllato sulla TME, The Lancet. Oncologia, 12, 575-582, 2011.
- Adua, D. (2019). Validazione di un profilo biomolecolare e mutazionale in pazienti affetti da tumore del retto localmente avanzato candidati a trattamento multimodale.
- Sebag-Montefiore, D., Stephens, R. J., Steele, R., Monson, J., Grieve, R., Khanna, S., ... & Parmar, M. (2009). Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. The Lancet, 373(9666), 811-820.
- Ríos Juvenal A., Barake M. Francisca, Arce María José, López-Köstner Francisco, Labbe Tomas P., Villena Jessica et al. Situazione attuale del cancro al colon in Cile: uno sguardo traslazionale. Rev. medico Cile [Internet]. 2020 giugno [citato il 23 dicembre 2022]; 148(6): 858-867. Disponibile su:
- MINSALE. Guida alla pratica clinica - Problema sanitario AUGE n. 70 Cancro colorettale nelle persone di età pari o superiore a 15 anni [Internet]. [citato il 18 settembre 2019]. Disponibile da:
- Conroy, T., Bosset, J. F., Etienne, P. L., Rio, E., François, É., Mesgouez-Nebout, N., ... & Marquis, I. (2021). Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): a multicentre, randomised, open-label, phase 3 trial. The Lancet Oncology, 22(5), 702-715.
- Fokas, E., Schlenska-Lange, A., Polat, B., Klautke, G., Grabenbauer, G. G., Fietkau, R., ... & German Rectal Cancer Study Group. (2022). Chemoradiotherapy plus induction or consolidation chemotherapy as total neoadjuvant therapy for patients with locally advanced rectal cancer: long-term results of the CAO/ARO/AIO-12 randomized clinical trial. JAMA oncology, 8(1), e215445-e215445.
- Geke Hospers, Renu R. Bahadoer, Esmee A. Dijkstra, Boudewijn van Etten, Corrie Marijnen, Hein Putter, Elma Meershoek – Klein Kranenbarg, Annet G. Roodvoets, IrisD. Nagtegaal, Regina GH Beets-Tan, Lennart K. Blomqvist, Tone Fokstuen, Albert J. ten Tije, Jaume Capdevila, MathijsP. Hendriks, Ibrahim Edhemovic, Andres Cervantes, Per J. Nilsson, Bengt Glimelius e Cornelis JH Van De Velde Journal of Clinical Oncology 2020 38:15_suppl, 4006- 4006.
- Garcia-Aguilar, J., Patil, S., Gollub, M. J., Kim, J. K., Yuval,J. B., Thompson, H. M., ... & Saltz, L. B. (2022). Organpreservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. Journal of clinical oncology, 40(23), 2546-2556.
- Dijkstra, E. A., Nilsson, P. J., Hospers, G. A., Bahadoer, R. R., Kranenbarg, E. M. K., Roodvoets, A. G., ... & Collaborative Investigators. (2023). Locoregional failure during and after short-course radiotherapy followed by chemotherapy andsurgery compared with long-course chemoradiotherapy and surgery: a 5-year follow-up of the RAPIDO trial. Annals of surgery, 278(4), e766-e772.
- Bachelet, V. C., & Rada, G. (2018). 51 Living friendly summary of the body of evidence using epistemonikos (frisbees) in medwave–a chilean experience of summarising the existing body of evidence on a specific clinical question.