
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2019) Volume 4, Issue 1
Effectiveness of Neuro Muscular Blockade in Conjunction of Low pneumoperitoneum in Resolving Postoperative Shoulder Pain in Laparoscopic Hysterectomy
2Anesthesia, Intensive Care and Pain Management Department, Faculty of Medicine; Ain Shams University, Egypt
Received Date: Mar 24, 2019 / Accepted Date: Mar 28, 2019 / Published Date: Apr 03, 2019
Copyright: ©Ekramy Abd Elmoneim Mohamed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Laparoscopic hysterectomy procedures are evolving and upgraded leading to more enhanced patient care levels. Post-operative shoulder pain after laparoscopic pneumoperitoneum is a common concern among laparoscopic surgeons and an annoying symptom causing discomfort of cases.
Aim: The research study investigates the difference between lowpressure level pneumoperitoneum 8mmHg in conjunction deep neuromuscular blockade in comparison to classic level pneumoperitoneum pressure 12mmHg in conjunction to moderate neuromuscular blockade if it could decrease the frequency of shoulder pain after performance of laparoscopic hysterectomy.
Methodology: A prospective research study that recruited 32 study subjects were randomized to either deep neuromuscular blockade and 8mmHg pneumoperitoneum (research Group 8-Deep) or moderate neuromuscular blockade and 12mmHg pneumoperitoneum (research Group 12-Moderate)both research groups were equal in number and were observed postoperatively for pain using VAS scoring system.
Conclusions and recommendations: The current research study reveal and displays that the conjunction of deep neuromuscular blockade and low pressure level pneumoperitoneum decreased the frequency and severity of shoulder pain after performance of laparoscopic hysterectomy in comparison to moderate level neuromuscular blockade and classic level –pressure pneumoperitoneum.
Introduction
Laparoscopic gynecological procedures are the uprising era in practice of all gynecological procedures that are considered highly skillful such as laparoscopic hysterectomy that is performed in every day practice for various indications from benign uterine disease such multiple fibroid uterus causing non medically resolving bleeding issues [1-2].
Furthermore, even oncological gynecological cases requiring hysterectomy are performed laparoscopically which is considered a high standard of care. Laparoscopic instrumental advances and safety precautions still didn’t resolve one of the most patient annoying side effects such as shoulder pain experienced post operatively that requires careful monitoring and follow up of pain management protocols [3-4].
Shoulder pain felt postoperatively is usually caused by the critical operative step of inducing pneumoperitoneum that aids in visualization of the abdominal and pelvic cavity contents and structures in a manner that allows safe and feasibility during intraoperative performance by clarifying the visual field. neuromuscular blockade in conjunction to laparoscopic surgical practice is becoming of a growing research interest as various prior research groups of investigators have revealed and displayed that it reduces the required pneumoperitoneal pressure required that favors the cardiovascular system during the anesthetic procedure furthermore it was revealed and displayed by various research groups that visual laparoscopic field is not affected by the procedure [5-8].
On the other hand, the precise and optimal indices and practice of neuromuscular blockade in conjunction to pneumoperitoneum implemented is still a matter of research debate among various investigators all over the globe [9-11].
Aim: The research study investigates the difference between low pressure level pneumoperitoneum 8mmHg in conjunction deep neuromuscular blockade in comparison to classic level pneumoperitoneum pressure 12mmHg in conjunction to moderate neuromuscular blockade if it could decrease the frequency of shoulder pain after performance of laparoscopic hysterectomy.
Methodology
After approval of local ethical committee on the current study and a written informed consent was taken from all participants, A prospective research double-blind study conducted at Mohammad Saleh Bashrahil Hospital in Holly Makkah, Saudi Arabia during the period between January 2016 and January 2019, that recruited Thirty-two study subjects randomized to either deep neuromuscular blockade and 8mmHg pneumoperitoneum (research Group 8-Deep, n=16) or moderate neuromuscular blockade and 12mmHg pneumoperitoneum (research Group 12-Mod n=16). Anesthesia was induced with propofol and remifentanil and maintained with propofol and remifentanil adjusted under the guidance of arterial blood pressure and an entropy target of 30 to 50 During induction, patients received 100% oxygen. After tracheal intubation, patients received 40% oxygen and the lungs were ventilated using pressure control ventilation, aiming for an end-tidal CO2 between 4.5 and 5.5 kPa. Anesthesia machine used is GE, carstation 650. Entroby GE, healthcare type E, Finland. With Neuromuscular monitoring the skin was cleaned with alcohol and rubbed with a piece of gauze and surface electrodes were placed over the right ulnar nerve close to the wrist. Forearm and ulnar fingers were immobilized and the acceleration transducer was placed on the thumb using a Hand Adapter.
Intravenous (i.v.) cannula has been positioned in the opposite arm. Once the patient was anaesthetized, a 50 Hz tetanic stimulus was applied for 5 s, and after baseline stabilization (<5% variation for at least 2 min), supramaximal stimulation and calibration was ensured using the calibration function. Tracheal intubation was performed 2 min after administration of rocuronium in both groups. In research Group 8-Deep, a bolus of rocuronium was administered immediately aftertracheal intubation and then an infusion of rocuronium was taking place. In research Group 12-Mod, no additional rocuronium was administered after tracheal intubation, but instead a similar volume of saline 0.9% was given and an infusion of 0.9% saline began after 20 to 30 min and the neuromuscular function could recover spontaneously. After introduction of the vress needle, the abdomen was insufflated to either 8 or 12mmHg pneumoperitoneum according to allocation. Consequently, laparoscopic trocars were introduced, and the cases were placed in the lithotomic, Trendelenburg position Postoperatively study subjects received oxycodone 2.5 to 5.0 mg intravenously or orally.
Cases were carefully instructed to ingest paracetamol 1000mg four times per day and etodolac 300 mg two times daily for 4 days. Patients were also allowed to take oxycodone 5mg (maximum 30mg per day) when needed. After 4 days, patients were allowed to take paracetamol, etodolac and oxycodone when needed. Before surgery, patients were carefully instructed by the research team to record, every night before bedtime, any arising pain from shoulder, site of incisions, lower abdomen and overall pain (involving other forms of pain, such as headache) that occurred both during rest and mobilization for 14 days implementing a 100mm visual analogue scale scoring system (0 indicating no pain and 100 worst imaginable pain). During the hospital administration, an investigator
Evaluated pain levels by the us age of a 100mm visual analogue scale scoring system at post-operative Arrival time till postanesthetic care unit, at 2, 4 and 8 hours, and at discharge from hospital. VAS scores, number of days before recommencement of daily activities and in gestinganalgesic agents recorded and tabulated in a separate research data sheet and returned to the main researcher by day 14 postoperatively.
Statistical Analysis
Data were collected, revised, coded, and entered to the Statistical Package for Social Science (IBM SPSS) version 23. The quantitative data were presented as mean, standard deviations and ranges when parametric and median with inter-quartile range (IQR) when non parametric. Also qualitative variables were presented as number and percentages. The comparison between groups regarding qualitative data was done by using Chi-square test and/or Fisher exact test when the expected count in any cell found less than 5. The comparison between two independent groups with quantitative data and parametric distribution was done by using Independent t-test while with non-parametric data were done by using Mann-Whitney test. The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the p-value was considered significant at the level of < 0.05.
Results
Table 1: reveals and displays the demographic and basic characteristics of the research cohort in which 32 study subjects were categorized in to 2 research groups 16 study subjects in each Group 8-deep, Group 12-mod research groups there was no statistical significant difference between both as regards age, BMI, ASA classification parity previous surgery hysterectomy performance pattern (total, subtotal (p values=0.252, 0.063, 0.617, 0.617, 0.287and 0.723 consecutively)
|
|
Total |
Group 8-deep |
Group 12-mod |
Test value |
P-value |
Sig. |
|
No. = 32 |
No. = 16 |
No. = 16 |
||||
|
Age |
||||||
|
Mean ±SD |
44.15 ± 6.05 |
42.9 ± 6.27 |
45.4 ± 5.82 |
1.169• |
0.252 |
NS |
|
Range |
30 – 57 |
32 – 57 |
30 – 57 |
|||
|
BMI |
||||||
|
Mean ±SD |
23.32 ± 2.84 |
22.34 ± 2.41 |
24.3 ± 3.27 |
1.930• |
0.063 |
NS |
|
Range |
19.3 – 28.4 |
19.3 – 27.5 |
19.8 – 28.4 |
|||
|
ASA classification |
||||||
|
1 |
29 (90.6%) |
15 (93.8%) |
14 (87.5%) |
0.249* |
0.617 |
NS |
|
2 |
3 (9.4%) |
1 (6.3%) |
2 (12.5%) |
|||
|
Parity |
||||||
|
Median (IQR) |
2 (1 – 3) |
2 (1 - 2) |
2 (1 - 3) |
0.572≠ |
0.617 |
NS |
|
Range |
0 – 4 |
0 – 4 |
0 – 4 |
|||
|
Previous surgery |
||||||
|
No |
15 (46.9%) |
9 (56.3%) |
6 (37.5%) |
1.129* |
0.287 |
NS |
|
Yes |
17 (53.1%) |
7 (43.8%) |
10 (62.5%) |
|||
|
Hysterectomy |
||||||
|
Total |
17 (53.1%) |
8 (50.0%) |
9 (56.3%) |
0.125* |
0.723 |
NS |
|
Subtotal |
15 (46.9%) |
8 (50.0%) |
7 (43.8%) |
|||
•: Independent t-test; ≠: Mann-Whitney test *: Chi-square test
Table 2: reveals and displays the pain observed in each research group there was no statistical difference between both research groups as regards shoulder pain 4 days and 14 days postoperative, incisional pain 4 and 14 days postoperative, lower abdominal pain 4 and 14 days postoperative, pain 4 and 14 days post-operative (p values=0.712, 0.420, 0.602, 0.219, 0.809, 0.706, 0.615 and 0.092 consecutively)
|
|
Group 8-deep |
Group 12-mod |
Test value |
P-value |
Sig. |
|
No. = 16 |
No. = 16 |
||||
|
Shoulder pain (4 days) |
|||||
|
Median (IQR) |
15.6 (7.23 – 49.5) |
26.7 (5.34 – 56.7) |
0.650 |
0.712 |
NS |
|
Range |
3.12 – 65.7 |
2.34 – 72.3 |
|||
|
Shoulder pain (14 days) |
|||||
|
Median (IQR) |
29.3 (9.7 – 65.3) |
39.5 (10.2 – 85.4) |
1.021 |
0.420 |
NS |
|
Range |
6.4 – 77.5 |
5.91 – 98.4 |
|||
|
Incisional pain (4 days) |
|||||
|
Median (IQR) |
89.4 (32.5 – 170.4) |
95.3 (34.2 – 162.7) |
0.821 |
0.602 |
NS |
|
Range |
27.3 – 202.6 |
23.5 – 221.3 |
|||
|
Incisional pain (14 days) |
|||||
|
Median (IQR) |
137 (75.2 – 280.4) |
153.0 (62.4 – 318.6) |
1.213 |
0.219 |
NS |
|
Range |
38.5 – 326 |
42.5 - 347 |
|||
|
Lower abdominal pain (4 days) |
|||||
|
Median (IQR) |
100.5 (47.8 – 209.5) |
107.6 (52.9 – 211.4) |
0.217 |
0.809 |
NS |
|
Range |
25.4 – 232 |
33.8 – 256.4 |
|||
|
Lower abdominal pain (14 days) |
|||||
|
Median (IQR) |
176.8 (98.2 – 345.9) |
199.3 (87.9 – 338.4) |
0.670 |
0.706 |
NS |
|
Range |
57.9 – 372.8 |
62.8 – 384.6 |
|||
|
Overall pain (4 days) |
|||||
|
Median (IQR) |
102.9 (47.4 – 196.4) |
118.6 (55.5 – 202.9) |
0.750 |
0.615 |
NS |
|
Range |
25.2 – 232.7 |
21.8 – 247.2 |
|||
|
Overall pain (14 days) |
|||||
|
Median (IQR) |
187.1 (100.3 – 418.2) |
237.8 (115.6 – 407.4) |
1.674 |
0.092 |
NS |
|
Range |
37.4 – 448.9 |
42.6 – 427.3 |
|||
•: Independent t-test; ≠: Mann-Whitney test *: Chi-square test
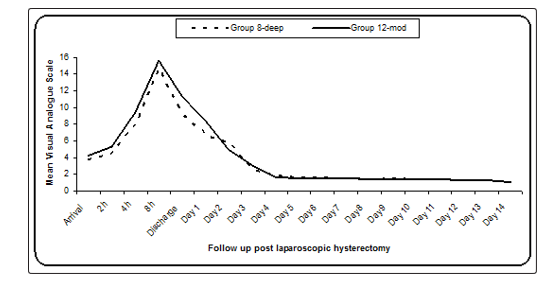
Table 3 and figure 1: reveal and display no statistical significant difference as regards VAS Scoring between both research groups from arrival from the operation room till day 14 postoperative (p values =0.219, 0.095, 0.144, 0.335, 0.095, 0.137, 0.071, 0.193, 0.532, 0.765, 0.775, 0.940, 0.933, 0.661, 0.851, 0.851, 0.888, 0.850 and 0.751 consecutively
|
|
Group 8-deep |
Group 12-mod |
Test value* |
P-value |
Sig. |
|
No. = 16 |
No. = 16 |
||||
|
Arrival |
3.73 ± 1.25 |
4.25 ± 1.09 |
1.254 |
0.219 |
NS |
|
2h |
4.48 ± 1.33 |
5.32 ± 1.42 |
1.727 |
0.095 |
NS |
|
4h |
7.94 ± 3.15 |
9.39 ± 2.24 |
1.501 |
0.144 |
NS |
|
8h |
14.65 ± 3.17 |
15.6 ± 2.24 |
0.979 |
0.335 |
NS |
|
Discharge |
9.19 ± 2.14 |
11.27 ± 4.32 |
1.726 |
0.095 |
NS |
|
Day 1 |
6.65 ± 3.11 |
8.37 ± 3.25 |
1.529 |
0.137 |
NS |
|
Day 2 |
5.78 ± 1.35 |
4.92 ± 1.25 |
1.870 |
0.071 |
NS |
|
Day 3 |
2.61 ± 0.98 |
3.1 ± 1.1 |
1.330 |
0.193 |
NS |
|
Day 4 |
1.87 ± 0.67 |
1.69 ± 0.92 |
0.633 |
0.532 |
NS |
|
Day 5 |
1.63 ± 0.52 |
1.57 ± 0.60 |
0.302 |
0.765 |
NS |
|
Day 6 |
1.61 ± 0.47 |
1.56 ± 0.51 |
0.288 |
0.775 |
NS |
|
Day 7 |
1.52 ± 0.57 |
1.54 ± 0.89 |
0.076 |
0.940 |
NS |
|
Day 8 |
1.43 ± 0.60 |
1.45 ± 0.72 |
0.085 |
0.933 |
NS |
|
Day 9 |
1.53 ± 0.42 |
1.43 ± 0.80 |
0.443 |
0.661 |
NS |
|
Day 10 |
1.42 ± 0.65 |
1.38 ± 0.54 |
0.189 |
0.851 |
NS |
|
Day 11 |
1.46 ± 0.57 |
1.42 ± 0.62 |
0.190 |
0.851 |
NS |
|
Day 12 |
1.32 ± 0.62 |
1.35 ± 0.57 |
0.142 |
0.888 |
NS |
|
Day 13 |
1.25 ± 0.46 |
1.28 ± 0.43 |
0.191 |
0.850 |
NS |
|
Day 14 |
1.05 ± 0.33 |
1.1 ± 0.53 |
0.320 |
0.751 |
NS |
*: Data were presented as mean and SD and compared using Independent t-test
Visual analogue scale > 20 in the two studied groups during the 14 days follow up
Table 4 and figure 2: reveals and displays that The VAS scoring below 20 and above 20 was statistically significantly different between both research groups p value =0.032 in which 12 cases in the 8 –deep research group had VAS scoring below 20 whereas only 6 cases had a VAS scoring below 20 within the 12 –moderate research group ,furthermore the VAS scoring above 20 was present in 10 cases among the 12 –moderate research group whilst only 4 cases among the 8 –deep research group had VAS scoring above 20
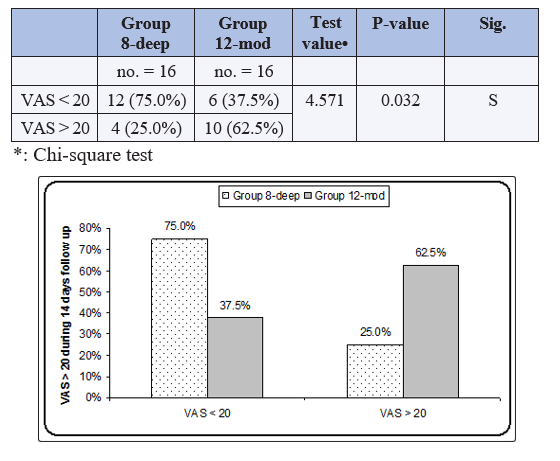
Table 5: Reveals and displays that there was no statistical significant difference between both research groups as regards Oxycodone requirements within 24 h , within 14 days, Return to daily activities, Length of hospital stay, Duration of surgery (min); p values =0.945, 0.803, 0.685, 0.406 and 0.775 consecutively
|
|
Group 8-deep |
Group 12-mod |
Test value |
P-value |
Sig. |
|
No. = 16 |
No. = 16 |
|
|
|
|
|
Oxycodone requirements within 24 h (mg); Median (IQR) |
20 (0 – 55) |
20 (0 – 65) |
0.062≠ |
0.945 |
NS |
|
Oxycodone requirements within 14 days (mg); Median (IQR) |
25 (0 – 200) |
25 (0 – 155) |
0.151≠ |
0.803 |
NS |
|
Return to daily activities; Mean ± SD |
9.23 ± 3.15 |
8.64 ± 2.9 |
0.551• |
0.685 |
NS |
|
Length of hospital stay; Median (IQR) |
18 (5 – 57) |
21 (5 – 39) |
1.120≠ |
0.406 |
NS |
|
Duration of surgery (min); mean ± SD |
73.3 ± 32.3 |
76.4 ± 28.3 |
0.289• |
0.775 |
NS |
≠: Mann-Whitney test; •: Independent t-test.
Discussion
Laparoscopic practice in gynecology is an uprising practice all over the world reducing pain and other clinically annoying issues for the patients is considered the enhancement of the level of patient safety and care offered to those category of cases, neuromuscular blockade is considered an adjunctive procedure that have been demonstrated by various researchers to enhance operative field visualization even at lower pneumo peritoneal pressure levels even in general surgery procedures not only gynecological practice [12-13].
Laparoscopic hysterectomy is becoming in an evolving manner the golden standard management protocol in many clinical scenarios in gynecological practice all over the world, however shoulder pain and other site pain issues are considered patient annoying that raised the research interest to reduce this side effect without affecting the level of patient care [14-15].
Multidisciplinary management of laparoscopic hysterectomy candidate patients is considered the cornerstone of safety for the cases as integrative and coordinate management between the anesthetic and gynecological teams reduce the draw backs and possible expected complications. Additionally, neuromuscular blockade is considered one of the safe guard actions from sudden abdominal wall motion during the surgical procedure that increases the surgical feasibility particularly in surgically challenging cases with dense adhesions [1, 3,7].
The current research study involved 32 study subjects were categorized in to 2 research groups 16 study subjects in each Group 8-deep, Group 12-mod research groups there was no statistical significant difference between both as regards age, BMI, ASA classification parity previous surgery hysterectomy performance pattern (total, subtotal (p values= 0.252, 0.063, 0.617, 0.617, 0.287 and 0.723 consecutively) as regards pain the research team observed the following in which there was no statistical difference between both research groups as regards shoulder pain 4 days and 14 days postoperative, incisional pain 4 and 14 days postoperative, lower abdominal pain 4 and 14 days postoperative, overall pain 4 and 14 days post-operative (p values =0.712, 0.420, 0.602, 0.219, 0.809, 0.706, 0.615 and 0.092 consecutively), furthermore at analyzing pain scores in a more detailed manner the following was revealed in which there was no statistical significant difference as regards VAS Scoring between both research groups from arrival from the operation room till day 14 postoperative (p values = 0.219, 0.095, 0.144, 0.335, 0.095, 0.137, 0.071, 0.193, 0.532, 0.765, 0.775, 0.940, 0.933, 0.661, 0.851, 0.851, 0.888, 0.850 and 0.751 consecutively. However the VAS scoring below 20 and above 20 was statistically significantly different between both research groups p value =0.032 in which 12 cases in the 8 –deep research group had VAS scoring below 20 whereas only 6 cases had a VAS scoring below 20 within the 12 –moderate research group, furthermore the VAS scoring above 20 was present in 10 cases among the 12 –moderate research group whilst only 4 cases among the 8 –deep research group had VAS scoring above 20.
Finally, there current research study finding revealed and displayed that there was no statistically significant difference between both research groups as regards Oxycodone requirements within 24 hours, within 14 days, return to daily activities, Length of hospital stay, Duration of surgery (min); p values =0.945, 0.803, 0.685, 0.406 and 0.775 consecutively.
A prior research group of investigators revealed and displayed from a similar research study to the current one that that deep neuromuscular blockade and pneumoperitoneum 8 mmHg in comparison to standard neuromuscular blockade and pneumoperitoneum 12 mmHg prohibited abrupt abdominal contractions during the operative conductance of laparoscopic hysterectomy [2,4,8].
Furthermore, deep neuromuscular blockade and pneumoperitoneum 8 mmHg enhanced surgical circumstances when performing abdominal fascia suturing procedure in comparison to regular neuromuscular blockade and pneumoperitoneum 12 mmHg.
Those research findings are in harmony with the current research and could be justified by the fact that a stable and steady operative field would reduce manipulations and therefore would reduce the operative tissue trauma expected subsequently reducing postoperative shoulder pain that is considered of paramount importance during laparoscopic hysterectomy performance. On the other hand, another research group of investigators performed a similar research study to the current research in methodology and approach have revealed and observed that creation of deep neuromuscular blockade during the surgical procedure is incapable to avoid adverse surgical events e.g. bladder injury, hematoma development [9,12,13].
A prior research systematic review revealed and displayed that deeper levels of neuromuscular blockade in comparison to neuromuscular blockade levels enhances subjective rating levels of surgical situations during particular laparoscopic procedures another prior research group of investigators compared deep neuromuscular blockade (PTC 0-1) with a standard neuromuscular blockade regimen defined as spontaneous recovery after a single dosage of rocuronium if the cases developed sudden movements during surgery, the research team adopted the anesthetic option to administer a an opioid bolus or to raise the anesthesia depth, on the other hand this could negatively impact the cardiovascular system and may perhaps more over not successful each time in prevention of sudden movements [5,14].
Furthermore, another research study previously conducted similar in methodology to the current research in which, deep NMB and 8mmHg pneumoperitoneum was compared with moderate NMB and 12mmHg Pneumoperitoneum in which the research team has observed statistically significantly decreased shoulder pain incidence during the 14 days after performing laparoscopic hysterectomy. In the research group of deep neuromuscular blockade in conjunction with low-pressure pneumoperitoneum without prolongation of operative time or manipulating the operative procedure completion furthermore the research team of investigators in harmony with the current research study results didn’t observe any statistical differences in other pain outcomes this could be justified by the fact that cases were already sufficiently treated with the standardized multimodal pain management protocol [1,15].
Another research team demonstrated reduced absolute risk in the manifestation of shoulder pain of around 31% by integration of deep neuromuscular blockade and low-pressure level pneumoperitoneum. Another previous research study investigating laparoscopic hysterectomy procedure performance comparing low-pressure (8mmHg) with usual - pneumoperitoneum pressure (12mmHg) mentioned an absolute risk reduction. In the existence of shoulder pain. This reduction, on the other hand, was only observed within the first 3 hours postoperative hours. Another research study investigating laparoscopy surgery revealed and displayed that the Usage of deep NMB in comparison no NMB prohibited sudden movements and accidental visceral perforations [3,11].
Conclusions and Recommendations
The current research study reveals and displays that the conjunction of deep neuromuscular blockade and lowpressure level pneumoperitoneum decreased the frequency and severity of shoulder pain after performance of laparoscopic hysterectomy in comparison to moderate level neuromuscular blockade and classic level –pressure pneumoperitoneum (12mmHg), however the results of the current research study should be interpreted with caution as other research variables could influence the pain scoring such as BMI differences between research study subjects that should be considered in future research studies. Furthermore future research studies should be conducted in a multicentric fashion with larger sample sizes putting in consideration intraabdominal and pelvic adhesions that could influence postoperative pain issues involving shoulder pain .
References
- Blobner M, Frick CG, Stäuble RB (2015) Neuromuscular blockade improves surgical conditions (NISCO). Surg Endosc 29: 627-636
- Dubois PE, Putz L, Jamart J (2014) Deep neuromuscular block improves surgical conditions during laparoscopic hysterectomy a randomized controlled trial. Eur J Anaesthesiol 31: 430-6.
- Staehr-Rye AK, Rasmussen LS, Rosenberg J (2014) Surgical space conditions during low-pressure laparoscopic cholecystectomy with deep versusmoderate neuromuscular blockade: a randomized clinical study. Anesth Analg 119: 1084 1092.
- Pandit JJ, Andrade J, Bogod DG (2014) The 5th National Audit Project (NAP5) on accidental awareness during general anesthesia: summary of main findings and risk factors. Anaesthesia 69: 1089-1101.
- Martini CH, Boon M, Bevers RF (2014) Evaluation of surgical conditions during laparoscopic surgery in patients with moderate vs deep neuromuscular block. Br J Anaesth112: 498-505.
- Madsen MV, Istre O, Staehr-Rye AK (2016) Postoperative shoulder pain after laparoscopic hysterectomy with deep neuromuscular blockade and low pressure pneumoperitoneum: A randomised controlled trial. Eur J Anaesthesiol 33: 341-347.
- Madsen MV, Staehr-Rye AK, Gätke MR (2015) Neuromuscular blockade for optimizing surgical conditions during abdominal and gynecological surgery: a systematic review. Acta Anaesthesiol Scand 59: 1-16.
- Donatsky AM, Bjerrum F, Go¨ genur I (2013) Surgical techniques to minimizeshoulder pain after laparoscopic cholecystectomy. A systematic review.Surg Endosc 27: 2275-2282.
- Madsen MV, Staehr-Rye AK, Gatke MR, Claudius C (2015) Neuromuscular blockade for optimizing surgical conditions during abdominal and gynecological surgery: a systematic review. Acta AnaesthesiolScand 59: 1-16.
- Dubois PE, Putz L, Jamart J (2014) Deep neuromuscular block improvessurgical conditions during laparoscopic hysterectomy: a randomized controlled trial. Eur J Anaesthesiol 31: 430-436.
- Staehr-Rye AK, Rasmussen LS, Rosenberg J (2014) Surgical space conditions during low-pressure laparoscopic cholecystectomy with deep versus moderate neuromuscular blockade: a randomized clinical study. AnesthAnalg 119: 1084-1092.
- Donati F, Brull SJ (2014) More muscle relaxation does not necessarily mean bettersurgeons or ‘‘the problem of muscle relaxation in surgery’’. AnesthAnalg 119: 1019-1021.
- Bogani G, Uccella S, Cromi A (2014) Low vs standard pneumoperitoneumpressure during laparoscopic hysterectomy: prospective randomized trial. J Minim Invasive Gynecol 21: 466-471.
- Blobner M, Frick CG, Stauble RB (2015) Neuromuscular blockade improves surgical conditions (NISCO). Surg Endosc 29:627-636.
- Lindekaer AL, Halvor Springborg H, Istre O (2013) Deep neuromuscular blockade leads to a larger intraabdominal volume during laparoscopy. J Vis Exp 76: 50045.