
Journal of Novel Physiotherapies Research Reviews(JNP)
ISSN: 2771-7739 | DOI: 10.33140/JNP

Case Report - (2022) Volume 3, Issue 1
EEG Changes During the Therapeutic Use of the VR-glasses-A Single Case Study
Received Date: Jan 13, 2022 / Accepted Date: Jan 18, 2022 / Published Date: Jan 31, 2022
Copyright: ©Copyright: ©2022 Michael Jung. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Jung M, H
Abstract
Physiotherapy for children and adolescents, who are cognitively well can be demanding, because besides the therapeutic challenge, motivation must be sufficiently maintained. Especially among teenagers, therapy compliance decreases greatly and there are many who drop out.
Introduction
Physiotherapy for children and adolescents, who are cognitively well can be demanding, because besides the therapeutic challenge, motivation must be sufficiently maintained. Especially among teenagers, therapy compliance decreases greatly and there are many who drop out. Also, since March 2020, it has become more difficult to treat patients in the physiotherapy practice setting due to the COVID-19 pandemic. A therapeutically adequate and strongly motivating home exercise program in terms of telemedicine is therefore considered a helpful intervention. In the following, supplementary therapy with VR goggles for a teenager with left hemiparesis is described.
Background
Numerous studies demonstrate that mirror therapy can produce motor improvement on the side of the body affected by hemiplegia [1-3]. Researchers hope to achieve a more intense stimulation of the brain with the application of VR goggles, as a stronger immersion effect is created by the goggles and the three-dimensional video sequences. The patient sees the corresponding videos from a first-person perspective and believes they are part of the scenario. Such effects are also used in video gaming to guarantee a more intense gaming experience.
For the intervention investigated here, bimanual activities of daily life were filmed with a 3-D camera and played to the patient. demonstrated that hand-arm bimanual intensive therapy (HABIT) also produces improvements in hemiplegic patients [4].
Another study using surface EMG, demonstrated that the use of VR goggles with these three-dimensional video sequences activate the muscles of the affected side of the body [5].
The purpose of this study is to investigate whether clear changes can be observed in the EEG of a patient while VR goggles are used in this way.
Case Presentation
The patient is a girl, born in 2003, as a premature baby at 32+2 weeks gestation, (birth weight 1780g, the 1st of twins). She suffered RDS II°, respiratory and circulatory insufficiency, perinatal asphyxia, and an ischemic infarction in the area of the right PCR stromal area.
At 14 years of age, this girl who is cognitively well, presents as follows: Spastic hemiplegic cerebral palsy of the left side (G80.2), GMFCS level II, BFMF level III, with spastic pointed/blunt left foot, symptomatic epilepsy (seizure-free; G40.9) and hemianopsia to the left, resulting in neglect of the left side.
The patient appeared awake, alert and showed great interest in our intervention.
Objectives
The aim of this single-case study was to determine whether the affected area of the brain can be activated when stimulated using two-dimensional photographic material or when using three-dimensional video graphic material, mediated through VR goggles. The EEG activity during the two different stimulations is not only compared to the resting-state EEG of the patient, where there is no stimulation, but also compared to each other to see which produces most activity.
The main question of this study is: Can a two-/three-dimensional visual stimulation produce significant activity in the EEG of the affected hemisphere of the brain?
The secondary question: Is one of the two visual stimulations superior to the other?
Methodology
The study protocol was positively evaluated by the Ethics Committee of the Fresenius University of Applied Sciences. After the patient and parent information was handed out to and read by the parents, both signed the Informed Consent.
During the resting-state EEG and the interventions, the patient is sitting unsupported on a chair without armrests in a quiet examination room. The only other people present are the two investigators and the mother of the patient. This setting remains unchanged throughout the whole study. The EEG cap is placed, the photographic material is shown to the patient by one of the investigators (Figure 1) and the VR goggles are later put on over the EEG cap and fixed with Velcro fasteners (Figure 2).
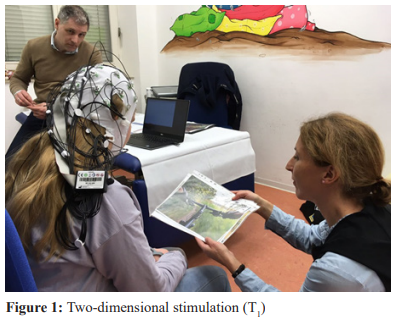
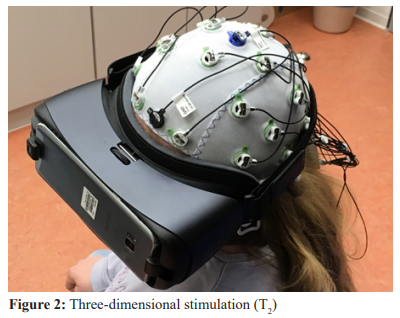
For this single case study, three EEG measurements were performed in a standardized setting: T0 = resting state without stimulation, T1 = under two-dimensional stimulation with photographs, T2 = under three-dimensional stimulation with VR goggles.
The EEG was recorded from 32 electrodes (500 Hz sampling rate) using a LiveAmp mobile EEG amplifier and the BrainVision Recorder software (BrainProducts GmbH, Gilching, Germany). EEGLAB was used for the EEG analysis. This is a bipolar derivation which measures the potential difference between two electrodes [6].
Intervention
Each of photographs presented, showed typical, child-like ambidextrous activities of daily living from a first-person perspective. The three-minute video sequences for the VR goggles, previously filmed with a special camera, showed the same bimanual activities as the photographs. These included riding a bicycle, playing table soccer or pinball, eating pizza or spaghetti with a knife and fork or spoon, and tying shoelaces. In two of the videos, participation was simulated, as the activities required cooperative action.
Results
The results only relate to our patient who has a left hemiparesis due to perinatal stroke.
In the EEG analysis, the high gamma frequency range (30-80 Hz) was cut off by a bandpass filter to eliminate noise and electrical interference. A recording rate of 128 Hz was documented. We omitted the gamma range since it features less in scientific literature. Afterwards, all electrodes that showed artifacts were taken out to evaluate only complete data sets. Subsequently, the EEG data was analyzed using an FFT and assigned to groups according to frequency.
Low frequencies: Delta = 1-4 Hz, Theta = 4-8 Hz, Alpha = 8-13 Hz, higher frequencies: Beta = 13-30 Hz. The definitions of where which frequency starts and where it ends, can differ in scientific literature.
In the following a descriptive evaluation of the seconds 30-60 (of a 180 second EEG) is shown as an example. (Figure 3)

Figure 3: EEG results at the points of measurement T , T and T
In the resting-state EEG (T0), a tendency for higher delta frequencies on the right side of the brain is shown, but also significantly lower alpha frequencies on the right and lower beta and theta frequencies on the left side of the brain. In summary, well discernible lateral differences were revealed in the above frequencies in the resting-state EEG.
Under two-dimensional stimulation (T1) with photos, no clear side difference is shown in the beta frequency. In the alpha frequency, there is a small increase on the left side of the brain, but a clear increase on the right side compared to T0, which is almost twice as high as the increase of the left side.
The delta frequencies show a small decrease on the left side during the course from T0 to T1, but a minimal increase on the right side at the electrodes C4, CP6, CP2. The theta frequencies show a small drop on both, the left and right side at 3/4 of the electrodes during this time. Side differences remain well discernible.
During three-dimensional stimulation (T2) with the VR goggles, there is a relative increase in beta frequency at electrodes C4, CP5, CP6, and P7. A relative decrease in alpha, delta, and theta frequencies is readily apparent from two-dimensional (T1) to three-dimensional (T2). A lateral difference (left > right) is clearly visible in the alpha - and beta frequencies.
The patient shows a clearer activity in the higher frequencies at rest (T0 ), only the low delta frequency is higher on the affected right side at rest than on the left. Two-dimensional stimulation (T1) leads to an increase in activity on the right side. The overall evaluation of the EEG shows that this patient has an affinity for high frequencies under three-dimensional stimulation (T2) with exciting situations. It can be noted that higher frequencies tend to show higher activity.
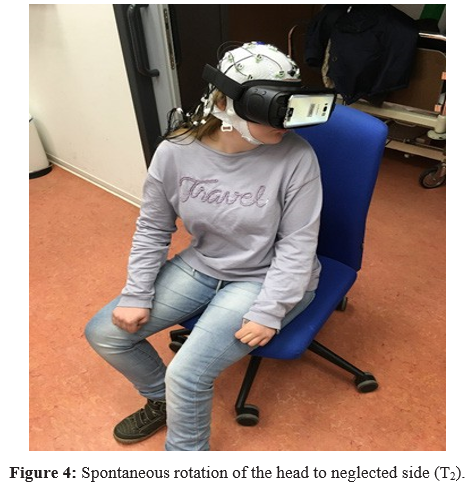
Particularly striking for the mother was the first reaction of her daughter under the intervention with the VR goggles (T2). The patient played the first video sequence and spontaneously turned her head to the left side, which is normally ignored due to neglect. (Figure 4) In the video sequence shown, no visual simulation from the left was offered, only cycling down a straight road was presented. The patient’s mother was very surprised about this “body effect” of the head movement. Meanwhile, the investigators noticed that presenting the video sequences led to better core stability (postural background) in the patient. Figure 4: Spontaneous rotation of the head to neglected side (T2). As a result, both two- and three-dimensional visual stimulation evoked activation at some right-hemispheric EEG electrodes. Since an increase in activity is seen at some electrodes while reduced activity is seen at others, neither stimulation can be said to be superior to the other.
As a result, both two- and three-dimensional visual stimulation evoked activation at some right-hemispheric EEG electrodes.
Since an increase in activity is seen at some electrodes while reduced activity is seen at others, neither stimulation can be said to be superior to the other.
Discussion
The investigators positively evaluate the fact that, in addition to the good acceptance of the VR goggles as therapy support, there is also an indication that an activation of the affected area takes place in the CNS. In addition to visible body effects, such as increased use of the affected arm, improved postural control and overcoming neglect, this study shows evidence of a neurophysiological correlate. To verify the high EEG frequencies as a result of exciting video sequences, and to produce exciting videos for the future, further studies with larger numbers of subjects should take place. In this context, it is recommended to also evaluate the gamma frequency range, which is less focused on in scientific literature.
Furthermore, it can be discussed whether 180 seconds of EEG recording are sufficient or whether a longer period of time causes further adaptation or activation processes.
The initial position (sitting without armrests) requires higher muscle tension, which may irritate the EEG derivation. Similarly, the muscular activities achieved under T1 and T2 stimulations may interfere with EEG derivations. A disadvantage of the EEG cap may be that the hair under the cap could increase transfer resistance.
fMRI images or CT images during a VR goggles application would be technically more differentiated and informative as an assessment. However, this is very challenging both technically and financially.
This first promising result, as well as the result from the EMG study of a hemiplegic boy (Jung, Burger & Höning, 2018), prompted the authors to start a 12-week randomized controlled VR glasses study.
Conclusion
This single-case study provided the first contribution to the hypothesis that supplementary therapy with VR goggles is as effective as mirror therapy for patients with CNS hemiparesis. The results of this study give hope to the assumption that visual stimulation with VR-goggles supports an activation of the affected area of the brain and thus can contribute to the motor rehabilitation for hemiplegic patients.
References
- Feltham M, Ledebt A, Deconinck F, Savelsbergh G (2010) Mirror visual feedback induces lower neuromuscular activity in children with spastic hemiparetic cerebral palsy. Research in Developmental Disabilities 31: 1525-1535.
- Gygax M, Schneider P, Newman C (2011) Mirror therapy in children with hemiplegia: a pilot study. Developmental Medicine & Child Neurology 53: 473476.
- Jung M, Wachter S, Tomczak M (2017) Einzelfallstudie über die Effekte von Spiegeltherapie auf die motorische Funktionsfähigkeit bei einem Kind mit Hemiparese. Single Case Study on the Effects of Mirror Therapy on Motor Functions in a Child with Hemiparesis. Physioscience 13: 65-72.
- Gordon AM, Hung YC, Brandao M, Ferre CL, Kuo HC, et al. (2011) Bimanual Training and Constraint Induced Movement Therapy in Children with Hemiplegic Cerebral Palsy: A Randomized Trial. Neurorehabilitation and Neural Repair 25: 692-702.
- Jung M, Burger R, Höning J (2018) EMG pattern analysis for a hemiplegic boy while using VR-glasses. Res Med Eng Sci 7: 2-4.
- Delorme A, Makeig S (2004) EEGLAB: an open-source toolbox for analysis of single-trial EEG dynamics including independent component analysis. Journal of Neuroscience Methods 13: 9-21.