




Research Article - (2025) Volume 4, Issue 2
Eating the Unthinkable: PICA-Induced Plastic Bezoar Causing Peritonitis-A Call for Community Based Prevention and Early Recognition of Childhood Anxiety
Received Date: Apr 11, 2025 / Accepted Date: May 14, 2025 / Published Date: May 19, 2025
Copyright: ©Â©2025 Arihant Jain, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Rajoria, S., Jain, A., Grewal, A. G. (2025). Eating the Unthinkable: PICA-Induced Plastic Bezoar Causing Peritonitis-A Call for Community Based Prevention and Early Recognition of Childhood Anxiety. J Surg Care, 4(2), 01-06.
Abstract
Rapunzel syndrome is a rare condition where a bezoar extends from the stomach into the duodenum or distal small intestine. Bezoars are formed by the progressive accumulation of a nondegradable foreign body in the stomach. This case highlights the habit of ingesting nonnutritive substances in children (PICA) as the underlying reason for bezoar formation. We report a case of a 6-year-old male who presented with intestinal obstruction and, when operated on in an emergency setting, turned out to have a bezoar of plastic and kite wire threads with intestinal perforation. Bezoar was extracted via laparotomy, and resection-anastomosis was done to achieve a successful outcome. Notably, his siblings, rather than his parents, were more aware of his habit of chewing kite-flying threads, making it necessary to involve all family members in the counselling sessions irrespective of age. Thus, the comprehensive management of such complications needs the integration of surgical and psychological approaches to treat and prevent recurrence.
Keywords
PICA, Bezoar, Plasticobezoar, Intestinal Perforation
Introduction
Bezoars are formed by clumping together millions of strands of indigestible materials, such as hair, cotton threads, etc., in the gastrointestinal tract. They are most commonly formed in the stomach due to its large capacity and can extend into the small bowel. There are a few known types of bezoars, such as trichobezoars (hairs), phytobezoars (fruit fibers, cotton threads, shells, seeds), and pharmacobezoars (medicines), which are being reported in children with a history of PICA and mental retardation [1]. Bezoar forms the reason for 2 - 4% of small bowel obstructions and only 1% of acute surgical emergencies in the pediatric population [2]. Bezoar formation by the consumption of kite-flying threads in the developmentally normal child is rarely reported. This case report highlights the possibility of such an extreme life-threatening complication in children with PICA. Also, it emphasizes the importance of having a high index of suspicion for early diagnosis and the need for subtle psychological assessment and counseling of children in the community.
Case Presentation
A 6-year-old boy of normal mental age was brought to the emergency department of a tertiary care hospital in northern India with a complaint of abdominal pain that had persisted for 20 days, primarily located in the epigastric region. Initially, the pain was intermittent, non-radiating, and was relieved by medication, without any specific aggravating factors. The child also experienced a high-grade fever, reaching up to 104 degrees Fahrenheit. Over time, the abdominal pain became more severe and diffuse, accompanied by recurrent bilious vomiting and progressive abdominal distension. The patient underwent fluid resuscitation at a nearby hospital before arriving at the tertiary care facility. Upon physical examination, the child appeared pale, febrile, and dehydrated, with a pulse rate of 140 beats per minute and a blood pressure of 100/70 mmHg. The abdomen was tense and distended, exhibiting generalized tenderness and signs of peritonitis.
Investigations
Laboratory investigations revealed a hemoglobin level of 8 g/dL and leucocytosis of 12,380/mm³, accompanied by a left shift. There were also elevated inflammatory markers and hypoalbuminemia, with a serum total protein level of 2 g/dL. Additionally, the coagulation profile was deranged, indicating sepsis. The remaining blood tests were within normal limits. (Table 1).
|
Parameter |
Reference Range |
Patient Value |
Interpretation |
|
Hemoglobin (g/dL) |
12.0 – 17.0 |
8.0 |
Low – Anemia |
|
Platelet Count (10³/μL) |
150 – 450 |
452 |
Slightly Elevated – Reactive? |
|
Total Leukocyte Count (10³/μL) |
4.0 – 10.0 |
12.38 |
Elevated – Leukocytosis |
|
Neutrophils (%) |
40 – 80 |
70.6 |
Normal |
|
Lymphocytes (%) |
20 – 40 |
14.5 |
Low |
|
Monocytes (%) |
2 – 10 |
12.8 |
Elevated |
|
Eosinophils (%) |
1 – 6 |
0.1 |
Low |
|
Basophils (%) |
0 – 1 |
0.0 |
Normal |
|
Urea (mg/dL) |
10 – 50 |
26 |
Normal |
|
Creatinine (mg/dL) |
0.7 – 1.2 |
0.26 |
Low – Likely age-related |
|
Sodium (mmol/L) |
136 – 148 |
139.0 |
Normal |
|
Potassium (mmol/L) |
3.5 – 5.0 |
3.96 |
Normal |
|
Chloride (mmol/L) |
96 – 106 |
103.0 |
Normal |
|
SGOT (U/L) |
0 – 40 |
16.0 |
Normal |
|
SGPT (U/L) |
0 – 41 |
8.0 |
Normal |
|
Alkaline Phosphatase (U/L) |
40 – 269 |
37.0 |
Low |
|
Total Proteins (g/dL) |
6.6 – 8.7 |
4.5 |
Low – Hypoproteinemia |
|
Albumin (g/dL) |
3.5 – 5.2 |
2.02 |
Low – Hypoalbuminemia |
|
C-Reactive Protein (mg/L) |
0.0 – 6.0 |
126.93 |
Markedly Elevated – |
|
Inflammation |
|
|
|
|
Prothrombin Time (seconds) |
9.3 – 12.6 |
16.9 |
Prolonged – Coagulopathy |
|
INR |
0.8 – 1.1 |
1.54 |
Elevated |
Table 1: Hematological and Biochemical Profile of the Patient at Presentation
Legend - The laboratory profile reveals anemia, elevated inflammatory markers (CRP and leukocytosis), hypoalbuminemia, hypoproteinemia, and coagulopathy. These findings are suggestive of systemic inflammation and possible nutritional compromise, consistent with an ongoing inflammatory process.
A contrast-enhanced computed tomography (CECT) scan of the abdomen revealed a severely distended stomach filled with large mottled material in the lumen, accompanied by a retroperitoneal collection of air. (Figures 1a and 1b).
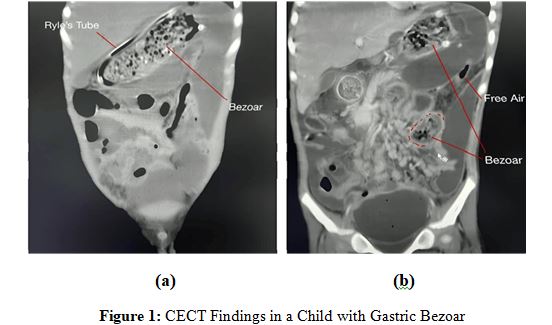
Legend - Coronal computed tomography (CT) scan images showing bezoars. (A) Bezoar in the stomach with a Ryle’s tube in situ. (B) Bezoar in the small intestine with free intraperitoneal air suggestive of perforation.
Treatment
After the preliminary fluid resuscitation, the child was taken for emergency exploratory laparotomy via midline abdominal incision, which showed bilious-purulent contamination with perforation at the proximal jejunum just distal to the duodenojejunal junction with sharp plastic fibers noted coming out of the perforated jejunum. On retrograde palpation, a similar material with a wire-like consistency was noted occupying the complete lumen of the stomach. (Figure 2) Since the bezoar was quite large, the anterior wall gastrotomy was made, and the bezoar was extracted slowly without significant spillage (Figure 3a). Resection of the diseased duodeno-jejunal segment was done with end-to-end anastomosis. Bezoar was the blended cluster of plastic fibers and entrapped food material (Figure 3b). Peritoneal lavage was done and abdominal drains were kept. Post-operatively the child was closely monitored in the pediatric intensive care unit with the necessary ventilator and ionotropic support due to the florid sepsis.
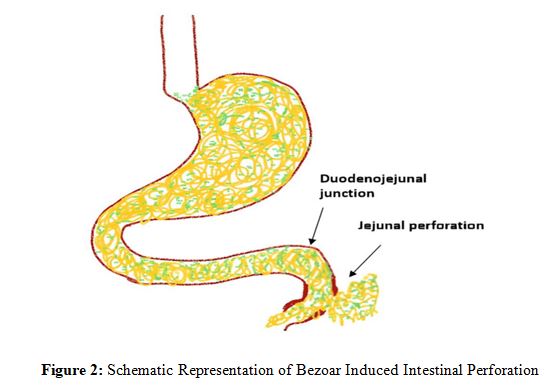
Legend - Represents the intraoperative findings in a child with a plastico-bezoar in the stomach, with an extension into the small intestine leading to jejunal perforation just distal to the duodenojejunal junction. This figure is original and was created bythe authors using digital drawing tools.
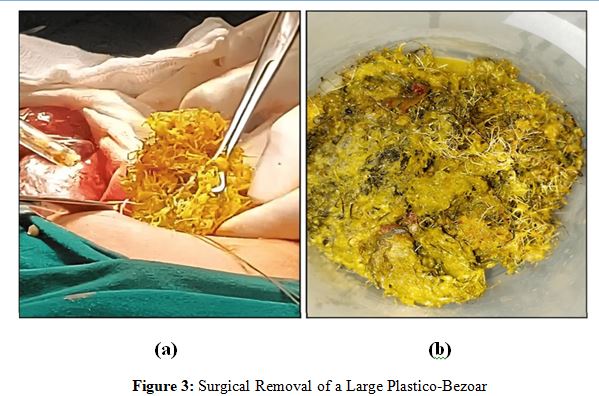
Legend - Intraoperative findings with an image on the left showing extraction of a plastic bezoar with entangled undigested plant fibers and an image on the right showing the removed plastico- bezoar with undigested food fibers in the specimen tray.
Outcome and Follow-up
After the surgery, the child was closely monitored in the pediatric intensive care unit and received necessary ventilator and inotropic support due to significant sepsis. Fortunately, the child's condition improved rapidly. By the first postoperative day, the child was taken off both ventilatory and inotropic support and gradually began oral feeding starting on the fifth postoperative day. The child, along with accompanying family members including siblings, underwent psychological counselling. During this process, the child’s younger sister revealed that he frequently chews on plastic wires, including kiteflying strings. However, the older family members were unaware of this habit and could not provide any related samples. He was then discharged in stable condition. The child did not come for physical follow-up counseling sessions but on a telephonic conversation. after 1 year, the child appeared to be doing well with no abnormal eating habits.
Discussion
Rapunzel syndrome is a rare entity where the bezoar formed in the stomach extends distally into the lumen of the duodenum and jejunum like the long-tied hairs of a princess in a fairy tale by the Grimm Brothers [3]. This, rather than being a gastrointestinal disorder, is a psychological disorder. Therefore, this is often encountered in children with depression, anxiety, and obsessive- compulsive disorders like trichotillomania (pulling out of self- hair), trichophagia (eating of hair), and PICA [4]. PICA is defined as the persistent and compulsive eating of non-nutritive substances for at least one month. PICA is most commonly noted in children at 36 months of age with a common co-occurrence in children with autism and intellectual disabilities, but the index case was normal intellectually and developmentally [5]. Trichobezoar is formed only in 1% of children with trichophagia, and only 20-30% of trichotillomaniacs will do trichophagia [6,7]. The incidence of trichobezoars is 0.5% worldwide, while the incidence of plastic bezoars is unknown and seldom reported [8]. (Table 2).
|
Case reports |
Age in years/gender |
Presentation |
History of PICA |
Procedure done |
|
This report |
6/male |
Acute intestinal obstruction with peritonitis |
PICA was revealed postoperatively by a younger sibling. |
Exploratory laparotomy with gastrotomy and resection and anastomosis of the duodenojejunal junction. |
|
Shrivastava RKP et al [15] |
14/female |
Gastric outlet obstruction |
PICA revealed preoperatively by parents |
Exploratory laparotomy with gastrotomy and extraction of plastic bezoar. |
|
Yaka M et al [16] |
14/female |
Recurrent vomiting due to gastric bezoar and jejunal perforation |
Parents revealed PICA postoperatively of chewing plastic material of chairs, and charpoys. |
Exploratory laparotomy with gastrotomy to extract plastic bezoar, and resection and anastomosis of the involved small intestine. |
|
Sultan N et al [17] |
58/female |
Acute kidney injury with incidental small intestinal foreign body on CT scan |
No history of PICA |
Plastic foreign at the gastric outlet and 90 cm proximal to the ileocecal junction was retrieved by enterotomy. |
|
Verma VK et al [18] |
12/male |
Chronic abdominal pain and palpable abdominal mass |
No history of PICA |
Gastric plastic bezoar with extension till proximal jejunum. Endoscopic followed by exploratory laparotomy. |
|
Aggarwal V et al [19] |
16/female 13/female |
Pain, nonpassage of stools and flatus, palpable lump. |
PICA of consuming chair knitting plastics revealed postoperatively. |
Gastric plastic bezoar with extension into jejunum. Exploratory laparotomy and retrieval via gastrostomy. |
Table 2: A Review of Case Reports of Plastico-Bezoar in Children and AdultsLegend - The table summarizes a few reported cases of plastic bezoars, detailing patient demographics, clinical presentation, history of PICA (if known), and the surgical procedures performed, along with our case report.
A bezoar is formed when the slippery fibrous strands escape gastric peristalsis and accumulate in the gastric mucosal folds. Peristalsis and the gastric secretions force the fibers to interweave and gradually form a large ball of indigestible fibers that cannot pass through the gastric outlet but can easily extend into the small bowel like a tail. Due to this sheltered increase in the size of bezoar, they are often diagnosed late [9]. Rapunzel syndrome is usually reported in the 13-20 age group and mostly in females, as shown in Table 2 [9]. The index case is a 6-year-old who presented in a surgical emergency with signs of perforation peritonitis, which is a rare presentation. Early presentations with just the complaints of abnormal ingestion or psychological behavior are rare. The history of unknowingly chewing plastic and kite threads is often discovered retrospectively after surgery, as in our case, where even the parents failed to recognize and address the issue as in the literature (Table 2). Incipiently, patients usually have epigastric pain, early satiety, loss of appetite, and sometimes a palpable abdominal mass with signs and symptoms of malabsorption. The symptoms worsen due to gradual entanglement and an increase in the size of the bezoar. They may present with melena or hematemesis due to pressure erosive gastritis or duodenal ulcers. Few may present with mechanical obstruction and perforation due to the pressure necrosis of the adjacent mucosa, as in the index case, where the stiff, wire-like fibers were noted popping out of the small intestine at the duodenojejunal junction, the fixed part of the gastrointestinal tract [10]. Although the diagnosis is often delayed due to the lack of proper history and complications, intestinal perforation is the most common complication noted among 108 cases of bezoar reported in the literature [11].
Bezoars are best managed through complete removal, along with regular psychological counseling sessions to help prevent recurrence. For smaller bezoars, several minimally invasive removal methods can be utilized, including endoscopic retrieval, bezotriptors to break down the tough fibers, enzymatic dissolution, and laparoscopic retrieval [12,13]. Large and complicated bezoars are removed through surgical gastrotomy or enterotomy, depending on their location, with careful attention to avoid intraperitoneal spillage [11]. The recurrence rate of a bezoar may be as much as 13.5% [14]. Even after the pertinent surgical management, the treatment is considered deficient without genuine cognitive behavioral therapy (CBT) and emotional support to prevent the recurrence of PICA and related complications.
Conclusion
Early recognition of PICA is crucial, as it can lead to severe gastrointestinal complications. Bezoarrelated perforation necessitates timely surgical intervention for favorable outcomes. The treatment is considered incomplete if it's not accompanied by family counselling sessions. Family members, especially siblings, may be more aware of abnormal eating behaviors than parents, emphasizing the role of family-wide counseling. Long-term behavioral therapy and multidisciplinary follow-up are essential in preventing the recurrence [15-19].
Key Clinical Message
• Early recognition of PICA is crucial, as it can lead to severe gastrointestinal complications.
• Bezoar-related perforation necessitates timely surgical intervention for favorable outcomes.
• Family members, especially siblings, may be more aware of abnormal eating behaviors than parents, emphasizing the role of family-wide counseling.
• Long-term behavioral therapy and multidisciplinary follow- up are essential in preventing recurrence.
Patient Consent
Written informed consent was obtained from the patient’s legal guardian to publish this case report.
Acknowledgements
The authors used ChatGPT (OpenAI) to assist in initially drafting the cover letter and title page. The content was subsequently reviewed and edited by the authors to ensure accuracy and originality.
References
1. Mirza, M. B., Talat, N., & Saleem, M. (2020). Gastrointestinal trichobezoar: an experience with 17 cases. Journal of Pediatric Surgery, 55(11), 2504-2509.
2. Salemis, N. S., Panagiotopoulos, N., Sdoukos, N., & Niakas, E. (2013). Acute surgical abdomen due to phytobezoar-induced ileal obstruction. The Journal of emergency medicine, 44(1), e21-e23.
3. Grimm, B. (1994). Rapunzel. Translated by Godwin-Jones R. Richmond. Virginia Commonwealth University: Department of Foreign Languages, 1994-1999.
4. Gerstenblith, T. A., Jaramillo-Huff, A., Ruutiainen, T., Nestadt, P. S., Samuels, J. F., Grados, M. A., ... & Bienvenu, O. J. (2019). Trichotillomania comorbidity in a sample enriched for familial obsessive-compulsive disorder. Comprehensive psychiatry, 94, 152123.
5. Papini, N. M., Bulik, C. M., Chawner, S. J., & Micali, N. (2023). Prevalence and recurrence of pica behaviors in early childhood: findings from the ALSPAC birth cohort. MedRxiv.
6. Irving,P.M.,Kadirkamanathan,S.S.,Priston,A.V.,&Blanshard, C. (2007). Gastrointestinal: rapunzel syndrome. Journal of gastroenterology and hepatology, 22(12), 2361-2361.
7. Grant, J. E., & Odlaug, B. L. (2008). Clinical characteristics of trichotillomania with trichophagia. Comprehensive psychiatry, 49(6), 579-584.
8. Agarwal, K., Agarwal, R., Agarwal, V., & Goel, S. R. (2025). Untangling rapunzel syndrome: A unique presentation of gastric trichobezoar. International Journal of Surgery Case Reports, 126, 110714.
9. Gonuguntla, V., & Joshi, D. D. (2009). Rapunzel syndrome: a comprehensive review of an unusual case of trichobezoar. Clinical medicine & research, 7(3), 99-102.
10. Avgoustou, C., Jannoussis, D., & Avgoustou, E. (2023). Gastrointestinal bezoars, a challenge to research and practice: A review. World Journal of Advanced Research and Reviews. 15:438-44.
11. Gorter, R. R., Kneepkens, C. M. F., Mattens, E. C. J. L., Aronson, D. C., & Heij, H. A. (2010). Management of trichobezoar: case report and literature review. Pediatric surgery international, 26, 457-463.
12. Wang, Y. G., Seitz, U., Li, Z. L., Soehendra, N., & Qiao, X. A. (1998). Endoscopic management of huge bezoars. Endoscopy, 30(04), 371-374.
13. Groenewald, C. B., Smoot, R. L., & Farley, D. R. (2006). A football-sized gastric mass in a healthy teen. Contemp Surg, 62, 531-534.
14. Abbas, T. O. (2011). An unusual cause of gastrointestinal obstruction: bezoar. Oman Medical Journal, 26(2), 127.
15. Shrivastava, R. K. P., & Shrivastava, A. (2024). Swallowed secrets-Plastic bezoar-induced gastric outlet obstruction in a 14-year-old girl: A case report. International Journal of Surgery Case Reports, 122, 110075.
16. Yaka, M., Ehirchiou, A., Alkandry, T. T. S., & Sair, K. (2015). Huge plastic bezoar: a rare cause of gastrointestinal obstruction. Pan African Medical Journal, 21(1).
17. Sultan, N., Attar, H., Sembawa, H., & Alharthi, H. (2024). A plastic bezoar causing bowel obstruction: A case of table cover ingestion. International Journal of Surgery Case Reports, 117, 109506.
18. Verma, V. K. (2013). Plastic bezoars—a unique introduction in bezoars family. Indian Journal of Surgery, 75(Suppl 1), 51- 53.
19. Agrawal, V., Joshi, M. K., Jain, B. K., & Gupta, A. (2009). Plasticobezoar-another new entity for Rapunzel syndrome. The Indian Journal of Pediatrics, 76, 229-230.