
Journal of Depression Anxiety Science(JDAS)

Case Report - (2025) Volume 2, Issue 1
Early Life Rejection, Poor Identify of Self and Others and Micro-Psychotic Episodes of Borderline Personality Disorder- A Case Report
Received Date: Aug 05, 2025 / Accepted Date: Sep 16, 2025 / Published Date: Sep 29, 2025
Copyright: ©2025 Amit Kumar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kumar, A. (2025). Early Life Rejection, Poor Identify of Self and Others and Micro-Psychotic Episodes of Borderline Personality Disorder- A Case Report. J Dep Anxiety Sci 2(1), 01-03.
Abstract
Prevalence of BPD in the general population varies between 0.7% and 2.7%, with symptoms usually manifesting in early adulthood [1]. Borderline personality disorder is associated with emotional suffering, self–harm attempts, poor interpersonal relationships and impairment in social functioning [2]. Currently, it is hypothesized that borderline personality disorder is caused by an interaction between genetic factors and adverse childhood experiences affecting brain development via neuropeptides and hormones [3]. Features mimicking BPD may be seen in various medical conditions like head trauma, neoplasms, HIV Encephalopathy and cerebrovascular accidents [4]. DSM- 5 lists several criteria for diagnosing borderline personality disorder, out of which minimum 5 criteria must be fulfilled [5]. Patient often presents with chronic low mood, difficulty maintain long term relationships, feelings of emptiness and abandonment [6]. Childhood trauma, disturbed family dynamics and temperament may be precipitating factors in many cases [7]. This case report tries to highlight the progression of various psychopathology in a 23-year-old girl, who underwent continuous troubled life circumstances and ultimately developed a chronic rebellious attitude towards others, mistrust and blurring of self-image.
Case Report
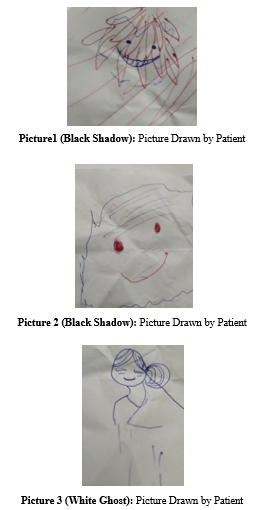
A 23-year-old female was brought to psychiatry opd for her intermittent excessive anger, deliberate self -harm attempts and difficulty in continuing the job for a period of 7 years. The problems started in the school age when she was in her higher secondary, with some altercations with her mentors. Few months later, she had multiple dissociative spells during that time when she had seizure like jerky movements of her body. After multiple such episodes she was shifted to another coaching centre and treatment given from various private clinics. After few years she had some conflict with a teacher at the institution for some reason. This incident caused lot of trauma to her mental health. She had more frequent dissociative spells and at times she attempted to kill herself. She was becoming more sensitive to critical comments and would seek pleasure after seeing her criticiser getting ill or sad. Her parents reported that she had extreme anger outbursts on trivial comments and would throw objects. On some occasions, she cut her wrist which she claimed to be attempts to take revenge. She claimed that she used to stalk people who made critical comments on her and she used to get gratified with the news of her opponents falling sick or getting harmed in any way. She was good at studies but the frequent interpersonal issues diverted her towards philosophical wings and she would search the meaning of life during the time of feelings of emptiness and rejection. She had good relations with opposite gender but was adamant towards females, though she could not maintain any long-lasting relationship with anyone. She reported that at times during stress, she would see some images, which she called black shadows (Figure 1, 2). According to her, these black shadows were scary and whenever she would see such black shadows, she would get scared and believe that the person on whom those black shadows are present are going to hurt her and she would maintain distance from such people. Sometimes, she would see a white ghost (Figure 3), which seemed like trying to pull her legs. She used to live scared but did not report these incidences before her parents assuming that they would believe her to be mentally ill. She also claimed that she cut her wrist in an attempt to threaten and punish her father who once scolded her, and such attempts gratified her ego. She consumed large number of benzodiazepines tablets in the past with suicidal intent. She however, did not repeat such lethal actions as on some occasions of self- harm attempts, she would hear some voices of Lord Krishna asking her not to kill herself and become a great person who can change the world. She was very happy while showing her 3 moles on her right side of face, which she claimed to be signs of very lucky and great person. During the time of interview, while discussing her past, she at times would clench her teeth in anger and say she has to remain alive to take revenge from people who passed comments on her in the past. Her mood was unpredictable and unstable and at times would start crying with meagre comments. She said, she resorted to cigarettes to ease her anxiety. She was lonely and felt the world has no room for her.
She also reported having a troubled childhood with frequent altercations between her parents which made her sad and lonely and she would spend time talking to herself. There was no family history of psychiatric illnesses. Her blood investigations and NCCT-Brain were within normal limits. She, however, had nystagmus the cause of which was yet to be discovered, and Tab Lacosamide prescribed by previous clinician was stopped assuming it to be the likely offending agent. She was started on Tab Sertraline 50 mg OD, Tab Aripiprazole 5mg HS, Tab Etizolam + Propranolol (0.5+20mg) OD, Tab Clonazepam 0.5 mg HS under close supervision.
Discussion
The patient in this case, had a troubled life with frequent quarrels between her parents. Belonging to a nuclear family, she found no one to share her feelings and wishes, and she got self-absorbed with time talking to herself. During the school days she had setback when she was teased by peers and at the same time teachers were rigid too. This made her develop a strong negative view of the world. Since childhood she was demanding in nature and her temperament was getting more fixated with adverse life situations. Stephanie D Stepp et al, describes childhood temperament dimensions of emotionality, activity, low sociability, and shyness as predictors of adolescent BPD symptom development [8]. With frequent rejections, she started living in low mood during which time she had some micro-psychotic episodes, when she used to see some images or hear some voices [9]. People with borderline personality have strong superego and thus her psychotic episodes were congruent to her mood as well as her thoughts, when she used to hear voices of Lord Krishna asking her not to kill herself because she has to change the world [10]. With growing age, she was becoming more impulsive and tried to cut her wrists on many occasions. Patients with borderline personality disorder use immature ego defense mechanism of projective identification, when she assured the psychiatrist that she had trust on him and wanted him to help her control her anger and that he is a good person (ingratiation), [11].
Conclusion
Borderline personality disorders are frequently encountered clinical entities in psychiatry practice. The aim of treatment should be focussed on reducing self-harm attempts, correcting the faulty cognition and provide emotional support. There is clearly a link between borderline personality disorder and bipolar disorder and thorough serial examinations may be necessary. The nature and nurture plays an important role in the development off this disorder [12].
Author Contribution
Entire work of this study has been done by the corresponding author.
Conflict of Interest
Author declares that there is no conflict of interest.
References
- Clarkin, J. F., Widiger, T. A., Frances, A., Hurt, S. W., & Gilmore, M. (1983). Prototypic typology and the borderline personality disorder. Journal of Abnormal Psychology, 92(3), 263.
- Paris, J. (2019). Suicidality in borderline personality disorder. Medicina, 55(6), 223.
- Leichsenring, F., Fonagy, P., Heim, N., Kernberg, O. F., Leweke, F., Luyten, P., ... & Steinert, C. (2024). Borderline personality disorder: a comprehensive review of diagnosis and clinical presentation, etiology, treatment, and current controversies. World psychiatry, 23(1), 4-25.
- Hagiwara, E., Katsuse, O., Okubo, T., Shirai, A., Itoh, A., & Ishigatsubo,Y. (2000).Two cases of HIV infectionaccompanied with borderline personality disorder. Kansenshogaku zasshi. The Journal of the Japanese Association for Infectious Diseases, 74(12), 1077-1080.
- Nuckols, C. C., & Nuckols, C. C. (2013). The diagnostic and statistical manual of mental disorders,(DSM-5). Philadelphia: American Psychiatric Association.
- Klonsky, E. D. (2008). What is emptiness? Clarifying the 7th criterion for borderline personality disorder. Journal of personality disorders, 22(4), 418-426.
- Herman JL, Perry JC, van der Kolk BA. (1989). Childhood trauma in borderline personality disorder. Am J Psychiatry.146(4),490-5.
- Stepp, S.D., Keenan, K., Hipwell, A.E. et al. (2014). The impact of childhood temperament on the development of borderline personality disorder symptoms over the course of adolescence. bord personal disord emot dysregul 1, 18.
- D'Agostino A, Rossi Monti M, Starcevic V. (2019). Psychotic symptoms in borderline personality disorder: an update. Curr Opin Psychiatry. 32(1):22-26.
- Garza-Guerrero C. (1988). Ego and superego alterations in borderline structures: their effect on the process and outcome of treatment. Int J Psychoanal. 1988;69 ( Pt 2):205-20. PMID: 3403162.
- Zanarini MC, Weingeroff JL, Frankenburg FR. (2009). Defense mechanisms associated with borderline personality disorder. J Pers Disord. 23(2):113-21.
- Lopes LM, Matias M, Marques M, Lopes IM, Reis J. (2023). Bipolar Disorder and Borderline Personality Disorder: A Diagnostic Challenge. Eur Psychiatry. 19;66(Suppl 1):S701.