
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2022) Volume 7, Issue 1
Early Detection and Pelvic Floor Rehabilitation for Sexual Dysfunction with or Without Incontinence in the Breast Cancer
Received Date: Feb 09, 2022 / Accepted Date: Feb 14, 2022 / Published Date: Jan 22, 2022
Copyright: ©Najwa Alfarra, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Najwa Alfarra, Khulood Alrashid, Tola Akomolafe. (2022). Early Detection and Pelvic Floor Rehabilitation for Sexual Dysfunction with or Without Incontinence in the Breast Cancer. Int J Women's Health Care, 7(1), 28-41.
Abstract
Introduction: Sexual health is an important aspect of human life, and cancer should not change that. Data suggested that issues related to sexual function are quite common among women treated for cancer ranged from 30% to 100% [1]. However, clinicians often spend little to no time on the topic. However, the treatment options are available. The literature also supports the use of pelvic floor exercises and dilators to improve sexual function and urinary incontinence in women and specially those presenting with orgasm problems [2].
Objective: To explore the effectiveness of the pelvic floor rehabilitation on sexual dysfunction or sexual dysfunction combined with incontinence in the Saudi breast cancer survivors during, or post chemotherapy intervention.
Methods: Thirty breast cancer women who had either sexual dysfunction, or sexual dysfunction combined with incontinence, during or post chemotherapy were evaluated using the Oxford scale for muscle power assessment before and after the intervention. Additionally, FSFI & UDI-6 questionnaire responses were received and analyzed before and after the pelvic floor rehabilitation. The supervised pelvic floor rehabilitation (which included the pelvic floor muscle training (seven Yoga poses: Mountain pose, Tree pose, standing forward bend pose, worrier pose, bridge pose, bound angle pose, and seated twist pose), manual therapy, and dilator) were conducted for 45 minutes once a week for eight weeks (a total of 8 sessions).
Main Outcome Measures: The domain scores of the Female Sexual Function Index-Breast cancer (FSDI-BC) which included desire, arousal, lubrication, orgasm, satisfaction, and pain, were calculated. Furthermore, the domain of the Urinary Distress Inventory (UDI-6) which included frequent urination, urgency leakage, activity leakage, leakage with coughing or sneezing, difficulty emptying the bladder, and pain or discomfort in the lower abdominal or genital area were also analyzed. Muscle power (Oxford scale) was measured before and after the treatment.
Results: All subjects successfully completed the study with no adverse events. Significant improvement in sexual function as assessed by the FSFI-BC indicated that sex desire improved by 86%, sexual arousal improved by 83%, lubrication improved by 76.3%, orgasm improved by 70%, general satisfaction improved by 44-54%, 73.3% felt pain minor, and 23% free of pain during intercourse. Muscle power as measured by the Oxford scale improved from grade 1 or 2 out of 5 to3 or 3+ out of 5. Significant improvement in UDI-6 were also observed in all participants by 80%.
Conclusion: In this study, we observed the influence of chemotherapy side effects for breast cancer on women’s quality of life, sexual function and continence. The study confirmed that Pelvic floor muscle training, manual therapy and dilator use showed significant improvement in the symptoms of continence and sexual function in breast cancer patients.
Keywords
Female Sexual Dysfunction, Pelvic Floor Exercises, Dilators, Breast Cancer, and Oncology
Introduction
Medical research continues to extend the life of cancer patients beyond the initial diagnosis. One of the challenges for both cancer survivors and the healthcare professionals who care for them is to comprehensively address all the issues that impact their quality of life. Issues regarding mobility, return to work, cosmetics, and self-care are readily identified and addressed. There are other ac¬tivities of daily living that may be hidden but should be included in a compressive rehabilitation program. Continence (urinary and fecal) and the ability to engage in sexual activity have been well documented to influence the quality of life scores for individuals with various types of cancer, especially after the patient has re¬ceived chemotherapy [2,3].
Additionally, more than 7.5 million out of 14.5 million cancer sur-vivors in the United States are women and that number is expected to grow to 9.602,590 by 2024. The increase in survival rates re-flects both earlier diagnosis and improvement in treatment [4]. De-spite the data showing that most survivors have a good prognosis, current treatments can result in problems, including symptoms re¬lated to sexual health. In 2007, Beckjord and Campas documented significant disruption in sexual quality of life that was the result of treatments and of emotional distress rather than of age in women with a diagnosis of breast cancer [5]. Estimation of the incidence of sexual dysfunction range from 30% to 100% among female can¬cer survivors, depending on the population queried and on how sexual dysfunction is characterized [1].
Different type of cancer in Saudi Arabia at 2018 was 15.807. Over-all cancer was more prevalent among women than men were as it affected 7.462 (47.2%) male and 8.345 (52.8%) female. All of these patients were treated properly either by surgery, chemother¬apy, radiation therapy, and/or they were referred by the physician to physical therapy to increase mobility or treat lymphedema. Up to date, there is no study on the quality of patients with sexual dysfunction, with/without urinary incontinence among the can¬cer patient [6]. However, there are a number of physical therapy approaches for cancer patients with sexual dysfunction combined with /without urinary incontinence including pelvic floor muscle training, soft tissue mobilization, core strengthening abdominal and pelvic exercises, and vaginal dilators. Brotto LA. et al, and Eftekhar T. et al., confirmed that the pelvic floor plays a role in both continence and sexual activity. To effectively address pelvic floor dysfunction, a thorough understanding of the pelvic floor anatomy and physiology is essential. The women’s health physical therapist will incorporate this knowledge with an appreciation of the impact of surgery, and chemotherapy on the function of the pelvic floor. The therapist will evaluate the patient to determine the source of dysfunction, provide scientifically supported education regarding positioning to decrease pain, instruct the patient on spe¬cific pelvic floor exercise programs, dilator use to decrease dryness and muscle spasm, and assist alleviating the symptoms in order to achieve optimal sexual function, treat the patient’s dysfunction and improve their sexual intimacy limitations as well as incontinence. There were multiple studies in that field that revealing that pelvic floor muscles exercise, significantly improved incontinence, de¬crease pain with intercourse, improve sexual function, as well as general quality of life in women with a history of breast cancer [7,8].
Rationale of the Study
As a Senior Physiotherapists working with female patients at a tertiary care hospital, our main concern is to provide a high qual¬ity of care, prevent further complications after the chemotherapy treatment and introduce proper education programs to breast can¬cer patients with sexual dysfunction with/without incontinence by using “different evidence based physical rehabilitation modal-ities”. However, to date, no research has been published to ex¬plore the Impact of Physical Rehabilitation intervention on Sexual Dysfunction/Incontinence in breast cancer patients during or post chemotherapy intervention. The aim of the study is to investigate the effectiveness of pelvic floor rehabilitation program to treat sexual dysfunction with/without urinary incontinence in the Sau¬di breast cancer survivors, who received chemotherapy treatment. This program included Manual therapy, use of dilator, pelvic floor muscle training using multiple yoga poses such as Mountain pose, Tree pose, standing forward bend pose, worrier pose, bridge pose, bound angle pose, and seated twist pose.
Impact of chemotherapy on breast cancer patients
Juliane, et al. found that 77 % of the breast cancer patients upon beginning chemotherapy refrained from sexual intercourse. This was mainly due to chemotherapy side effects, which might result in sudden loss of estrogen production in the ovaries. This can lead to symptoms of menopause, such as a thinning vagina (vag¬inal atrophy) and vaginal dryness, both of which can cause pain during penetration, and can damage tissues in the body, including the vagina. This damage can cause sores and may increase risk of infection. It can also cause bleeding, that will lead to loss of desire for sex. The women in this study reported pain due to the surgery, vaginal dryness, problem with arousal, making it difficult to enjoy sexual intercourse as change of the body image became more important. Additional side effects such as fatigue, nausea, hair loss, and weight loss or gain can make the patient feel unat¬tractive. The authors confirmed that this problem is considered a neglected problem9. Thus in younger patients, the impaired sexu¬ality persists longer after completion of chemotherapy compared to postmenopausal patients [9].
Sexual Dysfunction
This term can be defined as a disturbance in the sexual response cycle or as pain with sexual intercourse. Female sexual dysfunc¬tion has traditionally included disorders of desire, arousal, pain, and inhibited orgasm.
Female Sexual Function Index-Breast Cancer (FSFI.BC) Questionnaire
This is a health tool determining the level of sexual dysfunction in breast cancer women [10].
The FSFI-BC comprises of a 19-item questionnaire focused on sexual functioning. There are six domains assessed after cancer changes. The subject is advised to consider each of the questions in the context of the last 4 weeks.
• Desire – items 1 and 2; implying the wish/ wanting to engage in a sexual experience.
• Arousal – items 3, 4, 5 and 6; signs of attention, activity and excitement.
• Lubrication – items 7, 8, 9 and 10; refers to vaginal lubrica-tion that occurs during sexual excitement, presence, quantity or absence of it.
• Orgasm – items 11, 12 and 13; ability to attain orgasms, fac-tors impairing it.
• Satisfaction – items 14, 15 and 16; level of happiness.
• Pain – items 17, 18 and 19; discomfort sensations during in-tercourse [11]. Appendix 1
Urogenital Distress Inventory (UDI-6)
The Urogenital Distress Inventory-6 (UDI-6) questionnaire is used to assess types of urinary incontinence and its effect on quality of life.UDI-6, consists of 6 items: 1—Frequent urination, 2—Leak-age related to feeling of urgency, 3—Leakage related to activity, 4—Coughing, or sneezing small amounts of leakage (drops), 5— Difficulty emptying the bladder, and 6—Pain or discomfort in the lower abdominal or genital area [12].
The Oxford Grading Scale
This system to evaluate the strength of the pelvic floor muscles by using vaginal palpation. It consists of a six-point scale: 0 = no con¬traction, 1 = flicker, 2 = weak, 3 = moderate, 4 = good (with lift) and 5 = strong. Which is then recorded as 0/5 or 2/5, sometimes with a + or - sign to indicate more or less power but not sufficient to reduce or increase the number [13].
Methodology: A prospective study.
Methods
Thirty breast cancer patients during or post chemotherapy inter-vention, with confirmed cases of sexual dysfunction with/without incontinence by using the Female Sexual Function Index-Breast Cancer (FSFI-BC) Arabic validate version by (Anis, et al.) and Urogenital Distress Inventory (UDI-6) Arabic validate version by Altaweel, et al. [14]. Participants were aged 28-65 years old, and were manually examined to assess for the pelvic floor muscles power using oxford scale. The patients were recruited from the physical therapy outpatient clinic by the lymphedema therapist by asking them to answer the (FSFI-BC) and (UDI-6) questionnaires, if the patient had sexual dysfunction with/ without incontinence, the LE therapist will book the patient with the women’s health specialist therapist to start the treatment. The patient will answer these questions again after 8 weeks of completing the treatment. Re-evaluate the pelvic floor muscle power at the end of treatment. Furthermore, the survey included a participant information sheet outlining the nature of the study. The study was done at the King Faisal Specialist Hospital and research center, physical rehabilita¬tion department.
Inclusions criteria
The participants should be married, breast cancer patients during or post chemotherapy intervention and having sexual dysfunction with/without urinary incontinence secondary to chemotherapy.
Exclusion criteria
Pregnant women, any breast cancer patients not receiving chemo¬therapy.
Pelvic floor examination was carried out in the dorsal position, with the knees semi-flexed, the examining finger is squeezed and drawn into the vaginal canal and ask the patient to squeeze around the finger. The researcher assessed the strength of the contraction of pelvic floor muscles according to the oxford scale grading. The assessment was repeated three times, with ten seconds rest be¬tween each contraction. The median score of the three squeezes was taken for analysis. The test was done pre-post pelvic floor re¬habilitation intervention.
The patients were seen for 8 sessions with each session of 45 min¬utes, include 30 minutes’ pelvic floor exercise (yoga poses: Moun¬tain pose, Tree pose, standing forward bend pose, worrier pose, bridge pose, bound angle pose, and seated twist pose), 10 minutes’ of manual therapy for the pelvic floor muscles, and 5 minutes of teaching the patient how to use dilator at home once/week. (a total 8 sessions).
Proper Methods were used to teach the Patient the Proper PFM Contraction
First one, observation of correct pelvic floor muscles (PFM) con¬traction as squeeze around the urethral, vaginal, and anal openings and inward lift that is observed at the perineum using mirror as depicted in picture 1 below.

Picture 1: PFM Contraction Using Mirror First Method
Second, vaginal palpation: Kegel as a method to evaluate PFM function described this technique. By placing one finger in the dis-tal third of the vagina and asked the women to lift inward and squeeze around the finger. Kegel did not use this method to mea-sure PFM strength. He used vaginal palpation to teach women on how to contract their PFM and classified the contraction qualita¬tively as correct or not correct [15].

Picture 2: PFM Contraction Second Method
Second, vaginal palpation: Kegel as a method to evaluate PFM function described this technique. By placing one finger in the dis-tal third of the vagina and asked the women to lift inward and squeeze around the finger. Kegel did not use this method to mea-sure PFM strength. He used vaginal palpation to teach women on
The Patient Taught Hatha Yoga Poses
Mountain pose, Tree pose, standing forward bend pose, worrier pose, bridge pose, bound angle pose, and seated twist pose. The patient was instructed to perform each exercise with ten repetitions twice per day. (Picture 3)

Picture 3: Yoga Poses
Manual therapy uses internal vaginal soft tissue manipulation, or massage, to relieve pelvic pain by accessing muscles internal¬ly from the vaginal opening, therapist will hold gentle pressure and asked the patient to focus or relaxation and prober breathing, then again the therapist will hold gentle pressure while the patient performs a contract/relax of the pelvic floor muscles. Finally use sweeping stretches over the pelvic floor muscles belly.
Vaginal dilator is a plastic rod or cylinder with a rounded end. It is put in the vagina to open or stretch the tissues. This will keep the vaginal tissue healthy after having chemotherapy treatments. The therapist will apply a water-based lubricant (such as K-Y) to the dilator and the opening of the vagina. This will help the dilator slide into the vagina more easily (Picture 4).
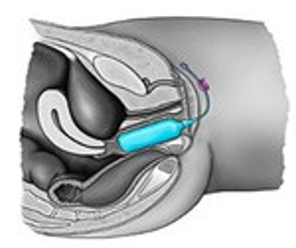
Picture 4: Dilator Insertion
Vaginal Dilators Kit
It comes in different size dilators ranging from small (about the size of a finger) to large. (See picture 5).
Therapist started using the smallest dilator in the kit and slowly increase the dilator size over time as the patient feels more com-fortable. Dilator therapy was used 3 to 4 times per week. Therapist instructed the patient to use it before bedtime, because it absorbs best with the patient lying flat and sleeping.

Picture 5: Dilators Kit
Main Outcome Measures
The Subjective Outcomes
All the participants completed the Female Sexual Function In-dex-Breast Cancer (FSFI-BC) and Urogenital Distress Inventory (UDI-6) Arabic validated version. Before commencing the treat¬ment and after eight weeks of completing the treatment, and each domain score, including desire, arousal, lubrication, orgasm, sat¬isfaction, and pain, as well as frequent urination, urgency leak¬age, activity leakage, leakage with coughing or sneezing, difficulty emptying the bladder, and pain or discomfort in the lower abdom¬inal or genital area were calculated.
Objective Outcomes
The pelvic floor muscle strength were measured using the Oxford grading scale before and after the treatment
Results
Thirty women met the inclusion criteria and gave their verbal con¬sent for the study. It was found out that 60% of the women grad¬uated from university, thirty percent graduated from secondary school and 10%, Elementary school. Sixty- five patients of them work in different field, the majority of them being teachers. The mean age of the women who participated in the study was 45.6 years (min 28, Max 65 years). All of them received Chemotherapy treatment before they started the physical rehabilitation program. The mean body mass index (BMI) was 24.5 with a statistically higher value in postmenopausal as compared to premenopausal patients (p=0.04). Of the participating women, 73% (n=22) were premenopausal at the time of therapy. A detailed description of the demographic data can be found in Table 1.
Table 1: Demographic Data and Baseline Scores
|
Features |
Elementary school |
Secondary school |
Bachelor degree |
Working |
Not working |
Under 45.6 years |
Above 45.6 years |
% |
|
Education |
10% |
30% |
60% |
|
|
|
|
|
|
Working status |
|
|
|
65% |
35% |
|
|
|
|
Age |
|
|
|
|
|
19 |
11 |
|
|
Premenopausal |
|
|
|
|
|
|
|
73% |
|
Postmenopausal |
|
|
|
|
|
|
|
17% |
Sexual Function
At the beginning of the chemotherapy treatment 40% of the par-ticipants were sexually inactive, adduced to being too tired, not interested because of the body image, pain during intercourse, with 60% of them being sexually active. However, by the end of chemotherapy course, they started to refrain from the sexual in-tercourse. This was mainly due to loss of libido and weariness, which led to vaginal dryness and causes pain during intercourse. The sexual function for those who were > 45.6 years were more problematic as compared to those who were <45.6 years. It was expected that sexual functions of those who were younger would be more affected as compared to the premenopausal with our re-sults confirming this assumption.
Female sexual dysfunction is prevalent in breast cancer patients, post-chemotherapy which threaten women’s quality of life. FS-FI-BC questionnaires showed that all of the participants in the study had one or more domin of sexual dysfunction. Sexual dys-function had been classically divided into six domin instruments measuring: desire, arousal, lubrication, orgasm, global satisfac-tion, and sexual pain as proposed by Rosen et al [10].
In this study, 30 women 100%. Had desire disorder with different degree of desire as shown in figure 6, due to body image changes, stress, chronic tiredness, and lack of emotional satisfaction with the relationship. While, sexual arousal disorder was identified in twenty-nine participants with different degree in sixteen women (53.3%) reported that their arousal as low, ten women (33.3%) found it moderate, and four (13.4%) never felt aroused during sex-ual activity, due to anxiety or depression. Furthermore, lubrication disorder affected all the participants. Sixteen women (54%) found it very difficult to maintain lubricant during intercourse, 36% of them were able to keep themselves wet until the completion of sexual activity, and 10% found it extremely difficult to keep themselves wet until the end of the intercourse, due to insufficient excitement and stimulation, Orgasm disorder in eighteen women (60%) had never reach orgasm, 30% of them less than half of the time had orgasm and 10% slightly found it not difficult, multiple factors were reported as being responsible such as: Boredom in sexual activity or a relationship, lack of proper stimulation, psy¬chological issues, fatigue and stress or depression, and painful in¬tercourse.
Overall, satisfaction nineteen women (63.3%) were moderately dissatisfied, nine women (30%) about equally satisfied and dis-satisfied, and two women (6.7%) moderately satisfied, the reason being that their partner (may be) is dissatisfied with their sex life because of body dysmorphic/changes that happened to her body image. Additionally, sexual pain noted and reported with 14 wom-en (46.7%) had most of the time pain, ten women (33.3%) had sometimes pain, and six women (20%) had always pain with inter-course, due to lack of sexual arousal, dryness of the vaginal area, and loss of libido.
Urinary Incontinence
About more than half of the participants complain of urinary in¬continence after the chemotherapy intervention 56.6%, in a form of minor drops of urine leakage during activities such as walk¬ing, running, laughing, sneezing, during intercourse and coughing. While the other participants 43.4% had no complain of inconti¬nence.
Clinical Implication of the Study
The FSFI-BC and UDI-6 questionnaires completed before and after the physical rehabilitation program showed successful out¬come in all the participants. It is evident that the physical reha¬bilitation intervention is crucial in order to improve sexual desire by 86% (figure 6), sexual arousal by 83% (figure 7), lubrication by 76% (figure 8), improve orgasm by 23% no difficulty at all, and 70% they found it slightly difficult to reach orgasm (figure 9), increase general sexual relationship satisfaction by 54% very satisfied , 44% moderately satisfied (figure 10), and pain felt few times though intercourse by 73.3% as compared with the percent¬age obtained before the physical rehabilitation intervention (figure 11). Additionally, urinary incontinence leakage improved by 80% (figure 12 A-F). Muscle power in 27 participants increased from the range of 1-2/5 to 3-3+ /5 (Table 2).
In summary, the physical rehabilitation intervention significantly reduced sexual dysfunction and urinary incontinence that induced by chemotherapy treatment and increased patient’s sexual satis¬faction as well as decrease pain through intercourse, without any adverse events.
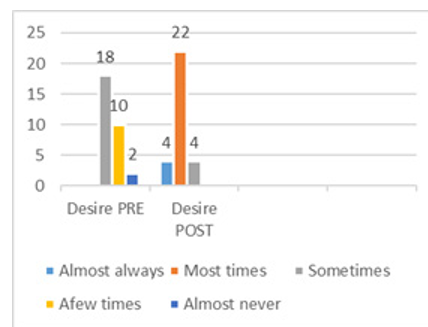
Figure 6: Sexual desire Pre-Post Physical Therapy Intervention

Figure 7: Sexual arousal Pre-Post Physical Rehabilitation Intervention
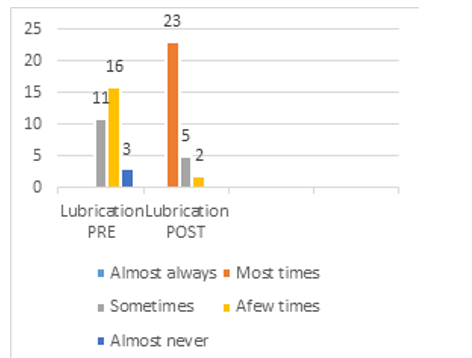
Figure 8: Sexual Lubrication Pre- Post Physical Rehabilitation Intervention

Figure 9: Sexual orgasm Pre-Post Physical Rehabilitation Intervention
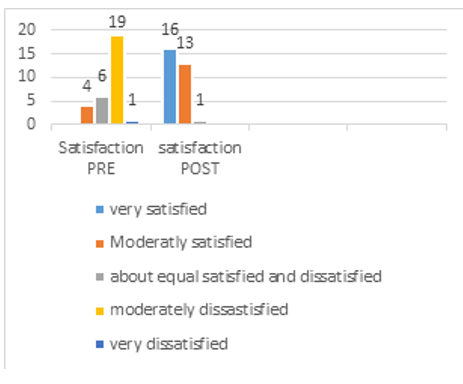
Figure 10: Sexual Satisfaction Pre- Post Physical Rehabilitation Intervention

Figure 11: Sexual pain Pre-Post Physical Rehabilitation Intervention
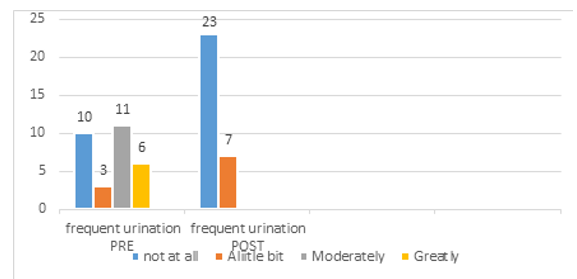
Figure 12: Urinary Distress Inventory (UDI-6), Pre-Post Physical Rehabilitation Intervention
A-Frequent Urination
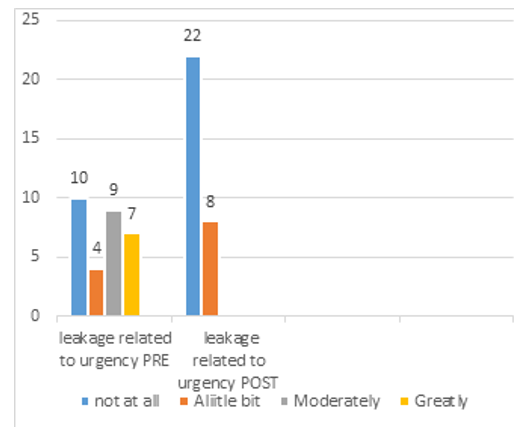
B- Urinary Leakage Related To Urgency
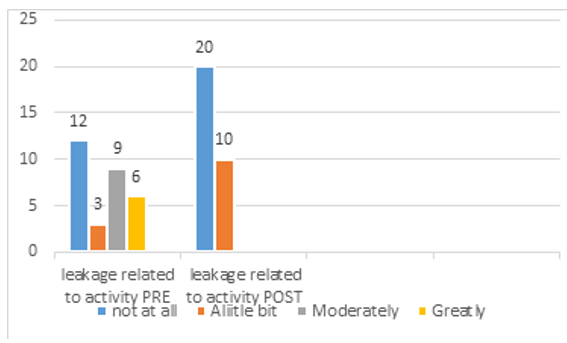
C-Leakage Related To Activity
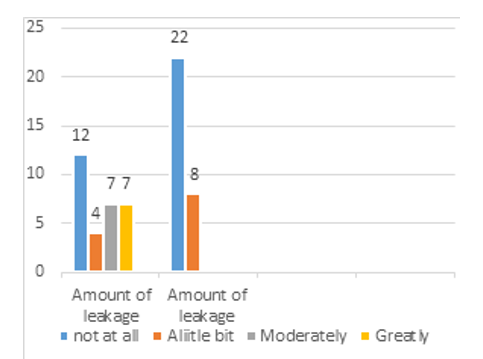
D-Amount of Leakage

E-Difficulty Emptying Bladder
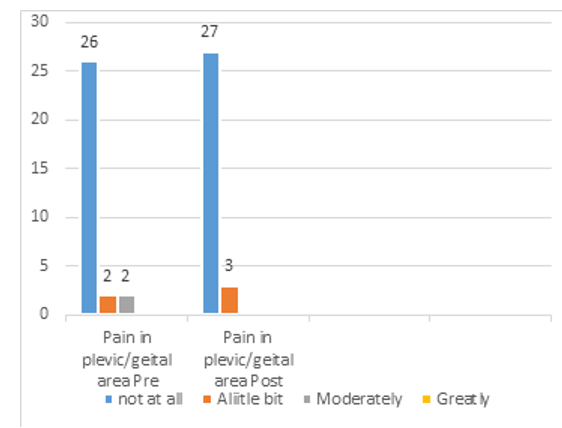
F- Pain in Pelvic/Genital Area
Muscle Power
Muscle power of the pelvic floor muscles were measured before and after the treatment with significant improvement as shown in (Table 2).
Table 2: A Comparison of the Pelvic Floor Muscle Power before and After the Physical Rehabilitation Intervention
|
Case # |
MP. Before the treatment |
MP. After the treatment |
|
Case 1 |
1+/5 |
3/5 |
|
Case 2 |
2/5 |
3+/5 |
|
Case 3 |
2/5 |
3+/5 |
|
Case 4 |
2/5 |
3/5 |
|
Case 5 |
1/5 |
3/5 |
|
Case 6 |
2/5 |
3/5 |
|
Case 7 |
2-/5 |
3/5 |
|
Case 8 |
2/5 |
3+/5 |
|
Case 9 |
2/5 |
3+/5 |
|
Case 10 |
2-/5 |
3/5 |
|
Case 11 |
1+/5 |
3/5 |
|
Case 12 |
2/5 |
3/5 |
|
Case 13 |
2/5 |
3+/5 |
|
Case 14 |
2-/5 |
3+/5 |
|
Case 15 |
1/5 |
2/5 |
|
Case 16 |
1/5 |
3-/5 |
|
Case 17 |
3-/5 |
3+/5 |
|
Case 18 |
2/5 |
3-/5 |
|
Case 19 |
2+/5 |
3+/5 |
|
Case 20 |
2-/5 |
3-/5 |
|
Case 21 |
1/5 |
2/5 |
|
Case 22 |
2/5 |
3/5 |
|
Case 23 |
3/5 |
3+/5 |
|
Case 24 |
2/5 |
3/5 |
|
Case 25 |
2+/5 |
3+/5 |
|
Case 26 |
3/5 |
3+/5 |
|
Case 27 |
1/5 |
2/5 |
|
Case 28 |
2+/5 |
3/5 |
|
Case 29 |
2-/5 |
3/5 |
|
Case 30 |
2/5 |
3/5 |
Discussion
The aim of this study was to analyze the effectiveness of pelvic floor rehabilitation program to treat sexual dysfunction with/with-out urinary incontinence in the breast cancer survivors, during and shortly after chemotherapy intervention. In this time, significant changes in quality of life, sexual function, and urinary incontinence were observed. This effect was more distinctive in premenopausal compared to postmenopausal patients. In premenopausal women, the diagnosis of cancer represents possibly an even greater change in daily life compared to older patients. Concerns regarding the sexual life, having more children may be considered more import¬ant in younger patients. Whereas premenopausal women in our study suffered more from side effects of chemotherapy treatment than postmenopausal patients, they seemed to recover faster and resulting in a higher score on the quality of life index.
Following treatment, the physical recovery is more promising in younger patients, which will contribute to better quality of life. This is in line with other published results such as Juliane, et al. which confirmed that premenopausal women showed less depres¬sion disorders and improvement in quality of life compared to the older patient’s group [9].
The reason for sexual inactivity were adduced to being too tired, not interested because of the body image, and pain during inter-course. These findings are supported by similar findings by Sergin et al. [15] which also implied that women felt less attractive than before therapy, due to their body image changes [16].
Regarding sexual function, we observed significant changes in all categories to include pleasure, discomfort, and orgasm in all of the participants. In premenopausal women, all the scores were im¬proved following pelvic floor rehabilitation as compared to some of the postmenopausal women, who still experienced pain with intercourse. This study concluded that sexuality is an important topic for younger patients and should be addressed by the consul¬tant physician.
Weiss, et al reported that regular pelvic floor exercises training in-clinic and at home augments the supportive function of the pelvic floor, enhances blood flow, and stimulates PFM proprio-ception, contributing to more intense orgasm [17]. Brotto et al in longitudinal prospective study; Sadownik et al in a qualitative ret¬rospective study; along with Bok et al. in a RCT agreed that pelvic floor exercise improves sexual function [7,18,19]. Goldenfinger et al. in another RCT; emphasized the efficacy of pelvic floor muscle training for sexual dysfunction, in support of earlier findings by Brotto et al and Bok et al. [20].
Furthermore, in a Turkish study by Beji et al. [21] improvement in sexual desire, and achievement of orgasm were reported in wom-en who received pelvic floor rehabilitation. Graber and Kline also observed that there is a positive correlation between the strength of women’s pelvic muscles and the intensity of her orgasmic re-sponse, in agreement with the findings of these confirmed that strong pelvic floor muscles were crucial for the attainment of or-gasm [22]. Chambless et al. Wurn at al. noted that physical ther-apy administered for the pelvic floor muscles improved sexual function in women [23,24]. Furthermore, Sayıl I and Berman et al. found that Pelvic floor muscles play important roles in sexual arousal, sexual response and sexual satisfaction in women [25,26]. The presence of hypertonic or hypotonic in pelvic floor muscles may result in problems during sexual intercourse or orgasm and urinary incontinence.
In this study, we closely monitored the impact of urinary inconti-nence on the participant’s life, during and after the chemotherapy intervention. We observed that more than half of the participants (56.6%) complained of urinary incontinence, however, following pelvic floor rehabilitation, most of the participants showed signif¬icant improvement in their incontinence. In agreement with other studies, Ireneusz & ChrzÄ?szczyk, found that regular pelvic floor muscle training resulted in a 90% reduction in the frequency of women need to use the toilet during the day, and 93% of respon¬dents did not use the toilet at night [27]. Thirty percent of respon¬dents reported reduction in the outflow of urine during physical activity, and 17% during sneezing. Marzieh et al. also confirmed that pelvic muscle exercises were an empowerment mechanism for incontinent women in improv-ing their quality of life and self-esteem, thus affirming and recom¬mended that these exercise programs be used for women in order to improve urinary incontinence [28].
The literature review by RadzimiÅ?ska A, et al. Demonstrated that PFMT is an effective treatment for UI in women. It could also be recommended as the first-line conservative treatment for elderly women. PFMT significantly improves the QoL of women with UI, with a duration no less than 6 weeks [29].
Significant progress has been made in breast cancer therapy es¬pecially in the management of the side effects of the disease and its treatment. However, this study strongly suggest the need for further research in the use and benefits of the PFM , management of chemotherapy induced side effect and other ways of addressing QoL of women with sexual dysfunction with /without urinary in¬continence and body dysmorphic following breast cancer surgery.
Conclusion
We observed that chemotherapy has different side effects that can influence breast cancer women such as fatigue, mouth soreness, quality of life, sexual function and incontinence, due to chang¬es at the hormonal levels, which play an important role in sexual arousal and orgasm, and that, can lead to decreased libido, vaginal dryness, and painful intercourse. Unfortunately, issues related to sexual health continue to be underappreciated, and consultations are not widely available in most communities. In this study, we provided background information on female sexual health; exam¬ine the impact of chemotherapy treatment on sexual function, and continence. The study concluded that the pelvic floor rehabilita¬tion (exercises, manual therapy, and dilator) showed significant improvement in the symptoms of sexual function and continence in breast cancer patients who received chemotherapy treatment. The authors however, observed that the sexuality is an important topic that is often neglected in this category of patients, therefore it is suggested that sexuality should be addressed by the consulting physician, and advising patients prior to, during, and after onco-logical treatment.
References
- DeSimone, M., Spriggs, E., Gass, J. S., Carson, S. A., Krych-man, M. L., & Dizon, D. S. (2014). Sexual dysfunction in female cancer survivors. American journal of clinical oncology, 37(1), 101-106.
- Health concept for women & men https://www.prostata-ther-apie.de/en/the-health-concept-for- men/prostate-inflamma-tion-and-urinary-incontinence/neocontrol/
- Anis, T. H., Gheit, S. A., Saied, H. S., & Al_kherbash, S. A. (2011). Arabic translation of Female Sexual Function Index and validation in an Egyptian population. The journal of sexual medicine, 8(12), 3370-3378.
- American Academy of Family Physicians/American Family Physician-Female Sexual Dysfunction: Evaluation and Treatment (2015).
- Beckjord, E., & Compas, B. E. (2007). Sexual quality of life in women with newly diagnosed breast cancer. Journal of psychosocial oncology, 25(2), 19-36.
- Cancer Facts & Figures, 2015.
- Brotto, L. A., Yong, P., Smith, K. B., & Sadownik, L. A. (2015). Impact of a multidisciplinary vulvodynia program on sexual functioning and dyspareunia. The journal of sexual medicine, 12(1), 238-247.
- Eftekhar, T., Sohrabi, M., Haghollahi, F., Shariat, M., & Miri,E. (2014). Comparison effect of physiotherapy with surgery on sexual function in patients with pelvic floor disorder: A randomized clinical trial. Iranian journal of reproductive medicine, 12(1), 7.
- Farthmann, J., Hanjalic-Beck, A., Veit, J., Rautenberg, B., Stickeler, E., Erbes, T., & Hasenburg, A. (2016). The impact of chemotherapy for breast cancer on sexual function and health-related quality of life. Supportive Care in Cancer, 24(6), 2603-2609.
- Rosen, C. Brown, J. Heiman, S. Leiblum, C. Meston, R. Shab-sigh, D. Ferguson, R. D’Agostino, R. (2000). The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. Journal of sex & marital therapy, 26(2), 191-208.
- Meston, C. M. (2003). Validation of the Female Sexual Function Index (FSFI) in women with female orgasmic disorder and in women with hypoactive sexual desire disorder. Journal of Sex &Marital Therapy, 29(1), 39-46.
- Uebersax, J. S., Wyman, J. F., Shumaker, S. A., & McClish,D. K. (1995). Short forms to assess life quality and symptom distress for urinary incontinence in women: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Neurourology and urodynamics, 14(2), 131-139.
- Laycock, J. O., & Jerwood, D. (2001). Pelvic floor muscle assessment: the PERFECT scheme. Physiotherapy, 87(12), 631-642.
- Altaweel, W., Seyam, R., Mokhtar, A., Kumar, P., & Hanash,K. (2009). Arabic validation of the short form of Urogenital Distress Inventory (UDIâ?6) questionnaire. Neurourology and Urodynamics: Official Journal of the International Continence Society, 28(4), 330-334.
- Mørkved, S., & Bø, K. (2014). Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. British Journal of Sports Medicine, 48(4), 299-310.
- Segrin, C., & Badger, T. A. (2014). Psychological and physical distress are interdependent in breast cancer survivors and their partners. Psychology, health & medicine, 19(6), 716-723.
- Weiss, P. M., Rich, J., & Swisher, E. (2012). Pelvic floor spasm: the missing link in chronic pelvic pain. Contemporary OB/GYN.
- Sadownik, L. A., Seal, B. N., & Brotto, L. A. (2012). Provoked vestibulodynia—Women’s experience of participating in a multidisciplinary vulvodynia program. The journal of sexual medicine, 9(4), 1086-1093.
- Bø, K., Talseth, T., & Vinsnes, A. (2000). Randomized controlled trial on the effect of pelvic floor muscle training on quality of life and sexual problems in genuine stress incontinent women. Acta obstetricia et gynecologica Scandinavica, 79(7), 598-603.
- Goldfinger, C., Pukall, C. F., Thibault-Gagnon, S., McLean, L., & Chamberlain, S. (2016). Effectiveness of cognitive-be-havioral therapy and physical therapy for provoked vestibulo-dynia: a randomized pilot study. The journal of sexual medicine, 13(1), 88-94.
- Graber, B., & Kline-Graber, G. (1979). Female orgasm: role of pubococcygeus muscle. The Journal of clinical psychiatry, 40(8), 348-351.
- Chambless, D. L., Sultan, F. E., Stern, T. E., O’Neill, C., Garrison, S., & Jackson, A. (1984). Effect of pubococcygeal exercise on coital orgasm in women. Journal of consulting and clinical psychology, 52(1), 114.
- Wurn, L. J., Wurn, B. F., Roscow, A. S., King, C. R., Scharf,E. S., & Shuster, J. J. (2004). Increasing orgasm and decreasing dyspareunia by a manual physical therapy technique. Medscape General Medicine, 6(4).
- Wurn, L. J., Wurn, B. F., Roscow, A. S., King, C. R., Scharf,E. S., & Shuster, J. J. (2004). Increasing orgasm and decreasing dyspareunia by a manual physical therapy technique. Medscape General Medicine, 6(4).
- Sayıl I. (1996). Mental health and disease textbook. Ankara: Antıp Corporation. 257-263.
- Berman, J. R., Adhikari, S. P., & Goldstein, I. (2000). Anatomy and physiology of female sexual function and dysfunction. European urology, 38(1), 20-29.
- Jurczak, I., & ChrzÄ?szczyk, M. (2016). The impact assessment of pelvic floor exercises to reduce symptoms and quality of life of women with stress urinary incontinence. Polski merkuriusz lekarski: organ Polskiego Towarzystwa Lekar-skiego, 40(237), 168-172.
- Jahromi, M. K., Talebizadeh, M., & Mirzaei, M. (2015). The effect of pelvic muscle exercises on urinary incontinency and self-esteem of elderly females with stress urinary incontinency, 2013. Global journal of health science, 7(2), 71.
- RadzimiÅ?ska, A., StrÄ?czyÅ?ska, A., Weber-Rajek, M., Sty-czyÅ?ska, H., Strojek, K., & Piekorz, Z. (2018). The impact of pelvic floor muscle training on the quality of life of women with urinary incontinence: a systematic literature review. Clinical interventions in aging, 13, 957.
Appendix 1: Female Sexual Dysfunction Index-Breast Cancer
1. Changes after Cancer-Desire
Over the past 4 weeks, how often did you feel sexual desire or interest?
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
2. Level (Degree) Of Desire/Interest
Over the past 4 weeks, how would you rate your level (degree) of sexual desire or interest?
Very high (+5 points)
High (+4 points)
Moderate (+3 points)
Low (+2 points)
Very low or none at all (+1 point)
3. Changes after Cancer-Frequency of Arousal
Over the past 4 weeks, how often did you feel sexually aroused
(“turned on”) during sexual activity or intercourse?
No sexual activity (0 points)
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
4. Change after Cancer-Level of Arousal
Over the past 4 weeks, how would you rate your level of sexual arousal (“turn on”) during sexual activity or intercourse?
No sexual activity (0 points)
Very high (+5 points)
High (+4 points)
Moderate (+3 points)
Low (+2 points)
Very low or none at all (+1 point)
5. Changes after Cancer-Confidence in Ability to Get Aroused
Over the past 4 weeks, how confident were you about becoming sexually aroused during sexual activity or intercourse?
No sexual activity (0 points)
Very high confidence (+5 points)
High confidence (+4 points)
Moderate confidence (+3 points)
Low confidence (+2 points)
Very low or no confidence (+1 point)
6. Changes after Cancer-Satisfactions about the Level of Arousal
Over the past 4 weeks, how often have you been satisfied with your arousal (excitement) during sexual activity or intercourse?
No sexual activity (0 points)
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
7. Changes after Cancer-Frequency of Lubrication
Over the past 4 weeks, how often did you become lubricated (“wet”) during sexual activity or intercourse?
No sexual activity (0 points)
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
8. Changes after Cancer-Difficulty in Becoming Lubricated
Over the past 4 weeks, how difficult was it to become lubricated (“wet”) during sexual activity or intercourse?
No sexual activity (0 points)
Extremely difficult or impossible (+1 point)
Very difficult (+2 points)
Difficult (+3 points)
Slightly difficult (+4 points)
Not difficult (+5 points)
9. Changes after Cancer-Did Not Maintain Lubrication
Over the past 4 weeks, how often did you maintain your lubrica¬tion (“wetness”) until completion of sexual activity or intercourse?
No sexual activity (0 points)
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
10. Changes after Cancer-Difficulty-Maintaining Lubrication
Over the past 4 weeks, how difficult was it to maintain your lu¬brication (“wetness”) until completion of sexual activity or inter¬course?
No sexual activity (0 points)
Extremely difficult or impossible (+1 point)
Very difficult (+2 points)
Difficult (+3 points)
Slightly difficult (+4 points)
Not difficult (+5 points)
11. Changes after Cancer-Frequency of Orgasms
Over the past 4 weeks, when you had sexual stimulation or inter¬course, how often did you reach orgasm (climax)?
No sexual activity (0 points)
Almost always or always (+5 points)
Most times (more than half the time) (+4 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+2 points)
Almost never or never (+1 point)
12.Changes after Cancer-Difficulty Achieving Orgasms
Over the past 4 weeks, when you had sexual stimulation or inter- course, how difficult was it for you to reach orgasm (climax)?
No sexual activity (0 points)
Extremely difficult or impossible (+1 point)
Very difficult (+2 points)
Difficult (+3 points)
Slightly difficult (+4 points)
Not difficult (+5 points)
13. Changes after Cancer-Satisfaction with Orgasms
Over the past 4 weeks, how satisfied were you with your ability to reach orgasm (climax) during sexual activity or intercourse?
No sexual activity (0 points)
Very satisfied (+5 points)
Moderately satisfied (+4 points)
About equally satisfied and dissatisfied (+3 points)
Moderately dissatisfied (+2 points)
Very dissatisfied (+1 point)
14. Changes after Cancer-Satisfaction with Emotional Close-ness
Over the past 4 weeks, how satisfied have you been with the amount of emotional closeness during sexual activity between you and your partner?
No sexual activity (0 points)
Very satisfied (+5 points)
Moderately satisfied (+4 points)
About equally satisfied and dissatisfied (+3 points)
Moderately dissatisfied (+2 points)
Very dissatisfied (+1 point)
15. Changes after Cancer-Satisfaction with Sexual Relation-ship
Over the past 4 weeks, how satisfied have you been with your sex-ual relationship with your partner?
Very satisfied (+5 points)
Moderately satisfied (+4 points)
About equally satisfied and dissatisfied (+3 points)
Moderately dissatisfied (+2 points)
Very dissatisfied (+1 point)
16. Changes after Cancer-Satisfaction with Overall Sexual Life
Over the past 4 weeks, how satisfied have you been with your overall sexual life?
Very satisfied (+5 points)
Moderately satisfied (+4 points)
About equally satisfied and dissatisfied (+3 points)
Moderately dissatisfied (+2 points)
Very dissatisfied (+1 point)
17. Changes after Cancer-Pain during Intercourse
Over the past 4 weeks, how often did you experience discomfort or pain during vaginal penetration?
Did not attempt intercourse (0 points)
Almost always or always (+1 point)
Most times (more than half the time) (+2 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+4 points)
Almost never or never (+5 points)
18. Changes after Cancer-Pain Following Intercourse
Over the past 4 weeks, how often did you experience discomfort or pain following vaginal penetration?
Did not attempt intercourse (0 points)
Almost always or always (+1 point)
Most times (more than half the time) (+2 points)
Sometimes (about half the time) (+3 points)
A few times (less than half the time) (+4 points)
Almost never or never (+5 points)
19. Changes after Cancer-Intense and Severe Pain
Over the past 4 weeks, how would you rate your level (degree) of discomfort or pain during or following vaginal penetration?
Did not attempt intercourse (0 points)
Very high (+1 point)
High (+2 points)
Moderate (+3 points)
Low (+4 points)
Very low or none at all (+5 points)
Appendix 2: UDI-6 ENGLISH VERSION QUESTION-NAIERS
1. Do you usually experience frequent urination? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |
2. Do you usually experience urine leakage associated with a feel¬ing of urgency; that is, a strong sensation of needing to go to the bathroom? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |
3. Do you usually experience urine leakage related to coughing, sneezing, or laughing? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |
4. Do you experience small amounts of urine leakage (that is, drops)? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |
5. Do you experience difficulty emptying your bladder? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |
6. Do you usually experience pain or discomfort in the lower abdominal or genital region? If yes, how much does this bother you?
|
Not at all |
Somewhat |
Moderately |
Quite a bit |
|
1 |
2 |
3 |
4 |