
Journal of Gynecology & Reproductive Medicine(JGRM)
ISSN: 2576-2842 | DOI: 10.33140/JGRM
Impact Factor: 1.247

Research Article - (2026) Volume 10, Issue 1
Duration of Foley Catheter Cervical Ripening as A Predictor of Total Length of Labor
Received Date: Jan 04, 2026 / Accepted Date: Feb 05, 2026 / Published Date: Feb 10, 2026
Copyright: ©2026 Caroline Lau, MD, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Lau, C., Elia, J., Olson, H. (2026). Duration of Foley Catheter Cervical Ripening as A Predictor of Total Length of Labor. J Gynecol Reprod Med, 10(1), 01-07.
Abstract
Objective: To determine whether there is a difference in time to delivery following Foley catheter expulsion when comparing a shorter duration of cervical ripening to a longer duration of cervical ripening among nulliparous patients with intact membranes and unfavorable cervix.
Methods: We conducted a retrospective chart review of all term, nulliparous patients with intact membranes and an unfavorable Bishop Score admitted for labor induction who underwent cervical ripening with a Foley catheter and Misoprostol. Our primary outcome was time to delivery following Foley catheter expulsion. Duration of Foley catheter cervical ripening was stratified into 2 groups depending on the time that the Foley catheter (FB) remained in place: Group 1 (“Fast FB”): ≤4 hours and Group 2 (“Slow FB”): >4 hours.
Results: A total of 175 patients met inclusion criteria. Ninety-one patients were stratified to the “Fast FB” group and 84 patients were stratified to the “Slow FB” group. The mean time to delivery following Foley catheter expulsion was not significantly different between groups (22.84 vs 23.29 hours; P=0.77). Among the 68 patients in the “Fast FB” group and the 55 patients in the “Slow FB” group who achieved vaginal delivery, the mean time to delivery was also not significantly different (20.45 vs 21.37 hours; P=0.68).
Conclusion: Among nulliparous patients with an unfavorable Bishop Score, there is no difference in time to delivery following Foley catheter expulsion. Therefore, efforts to shorten the total duration of labor should focus on expediting the duration of Foley catheter cervical ripening.
Keywords
Labor induction, Cervical ripening, Foley catheter, Misoprostol, Nulliparous women, Unfavorable Bishop score, Time to delivery, Mechanical cervical dilators, Term pregnancy, Vaginal delivery outcomes, Parturition, Time Factors
Introduction
Induction of labor is a common obstetrical procedure performed in the United States [1]. According to the CDC, the rate of induction more than doubled from 1990 to 2012 from 9.6% to 23.8%, regardless of gestational age [2]. During this same time period, the rate for late term inductions rose nearly 90%, largely due to a better understanding of the perinatal risks associated with post- term pregnancy [3-5].
Dr. Edward Bishop first noted that the condition of the unlabored cervix determines the likelihood of successful induction of labor in 1955 [6]. In 1964, he published a paper describing his system for pelvic scoring based on 5 components of the cervical exam dilation, effacement, station, consistency, and position. Today, the Bishop Score is frequently used to assess the favorability of the cervix prior to labor induction. A Bishop Score of ≤6 describes an unfavorable cervix, which would benefit from cervical ripening prior to labor induction. However, a pre-induction score >8 is considered equivalent to the likelihood of a multipara entering spontaneous labor [7].
The American College of Obstetricians and Gynecologists considers mechanical cervical dilators and prostaglandins safe and effective for cervical ripening agents.1 Foley catheters are among the oldest mechanical methods used for cervical ripening; offering several advantages including their low cost, low risk of tachysystole, few systemic side effects, convenience of storage, and relatively low risk of complications [8,9].
At our institution, the Foley catheter is a commonly used mechanical method for pre-induction cervical ripening. A deflated Foley catheter, usually an 18-French 30-mL catheter, is passed through an unfavorable cervix, then inflated with 60 cc of sterile normal saline and retracted on tension against the cervix. In the absence of a contraindication, vaginal Misoprostol is often administered concurrently. It is anecdotally believed that the application of “gentle traction” facilitates cervical ripening and decreases time to Foley catheter expulsion. Despite the widespread use of Foley catheters, the advantages of applied traction have not been proven.
In 2013, Gibson, et al., compared the effectiveness of inner thigh “taping” to “traction” using a weighted fluid bag on Foley catheters used for cervical ripening and concluded that the application of traction shortens the time to catheter expulsion but had no effect on time to delivery [10]. Similarly, Fruhman, et al. conducted a study in 2017 comparing tension to no tension on Foley catheters for pre-induction cervical ripening and also concluded a shortened time to catheter expulsion in the tension group but no significant reduction in time to delivery [11].
However, it remains unclear whether the duration of cervical ripening plays a significant role in shortening the total duration of labor. The aforementioned studies include multiparous patients, patients admitted with spontaneous rupture of membranes, and patients whom underwent concomitant cervical ripening with multiple types of pharmacologic methods, conditions that could inadvertently shorten the duration of cervical ripening and the total duration of labor [6,12].
Therefore, the objective of this study is to determine whether there is a difference in time to delivery following Foley catheter expulsion when comparing a shorter duration of cervical ripening to a longer duration of cervical ripening among term, nulliparous patients with intact membranes and unfavorable cervix.
Materials and Methods
We conducted a retrospective medical chart review at a single urban tertiary care hospital. The institutional review board for Kapiolani Medical Center for Women and Children in Honolulu, Hawaii approved this study. Because this was a retrospective study, it did not require approval from an ethics committee. The primary author reviewed all charts to ensure accurate and consistent data collection and documentation.
Records of patients admitted from January 2016 to January 2018 for induction of labor were reviewed. Eligible patients were term, nulliparas with a singleton intrauterine gestation who underwent cervical ripening with a Foley catheter and Misoprostol.
Additional inclusion criteria included gestational age ≥37 weeks, cephalic presentation and an unfavorable cervix defined as a Bishop score ≤6. Exclusion criteria were any medical conditions precluding vaginal delivery, age less than 18 years old, multiparas, multiple gestations, prior cervical or uterine surgery, fetal membrane rupture or the application of cervical ripening agents prior to Foley catheter insertion.
All patients included in this study underwent concurrent cervical ripening with an 18-French, 30 cc FB inflated with 60 cc of normal saline and Misoprostol 25 mcg placed vaginally every 4 hours until Foley catheter expulsion. The primary outcome was time to delivery of the neonate following expulsion of the Foley catheter. Duration of Foley catheter cervical ripening was stratified into 2 groups depending on the time that the Foley catheter (FB) remained in place: Group 1 (“Fast FB”): ≤4 hours and Group 2 (“Slow FB”): >4 hours. Secondary outcomes included mode of delivery, indication for cesarean delivery, postpartum hemorrhage, and maternal intrauterine infection. Postpartum hemorrhage was defined as estimated blood loss of over 1000 mL. Intrauterine infection was identified by the presence of an acceptable antibiotic regimen for the treatment of chorioamnionitis or endomyometritis in the patient’s medication administration record.
Sample size was calculated based on a mean time to delivery of 24.0±9.6 hours in the “Slow FB” group, and a hypothesized 20% reduction to 19.2±9.6 hours in the “Fast FB group, with an alpha level of 0.05, and a power of 80%. These assumptions required a sample size of 63 patients per group, for a total of 126 patients. Mean time to delivery and standard deviation estimations were based on previously published data [11]. Continuous outcomes were compared using the two-sided Student’s t test, or when not normally distributed, the Mann-Whitney U test. Categorical data were compared using the Fisher exact test. Statistical significance was set at P <0.05.
Results
A total of 209 charts of patients admitted for labor induction requiring cervical ripening with a Foley catheter and Misoprostol were abstracted. Thirty-four patients were excluded from analysis; 21 patients received Misoprostol for cervical ripening prior to Foley catheter placement, 1 patient received pitocin along with the Foley catheter and Misoprostol for cervical ripening, 9 patients received 50 mcg of Misoprostol for cervical ripening, 2 patients received a second Foley catheter following initial incorrect placement, and 1 patient was found to have a malpresenting fetus following Foley catheter expulsion. In total, 175 patients met inclusion criteria. Ninety-one patients were stratified to the “Fast FB” group and 84 patients were stratified to the “Slow FB” group.
Baseline maternal characteristics and pregnancy data are summarized in Table 1. There were no significant differences in maternal age, race, or BMI between study groups. There were no significant differences in gestational age upon admission and indication for labor induction. The median gestational age upon admission was 40 weeks.
|
Characteristic |
Cervical ripening ≤4 hours (N = 91) |
Cervical ripening >4 hours (N = 84) |
P value |
|
Maternal age, ya |
26 (22, 32) |
29 (23.3, 32) |
0.15 |
|
|
|
|
|
|
Race, n (%) |
|
|
0.05 |
|
Caucasian |
13 (14.3) |
18 (21.4) |
|
|
African American |
0 (0.0) |
4 (4.8) |
|
|
Hispanic |
2 (2.2) |
2 (2.4) |
|
|
Pacific Islander |
33 (36.3) |
15 (17.9) |
|
|
Asian |
39 (42.9) |
37 (44.0) |
|
|
Other |
2 (2.2) |
5 (6.0) |
|
|
Declined to answer |
2 (2.2) |
3 (3.6) |
|
|
|
|
|
|
|
Body mass index, kg/m2a |
33.7 (28.7, 39.0) |
32.0 (28.0, 37.6) |
0.16 |
|
|
|
|
|
|
Gestational age at admission, wka |
40 (38, 41) |
40 (39, 41) |
0.48 |
|
|
|
|
|
|
Indication for induction, n (%) |
|
|
0.83 |
|
Late term/post term |
25 (27.5) |
23 (27.4) |
|
|
Elective |
12 (13.2) |
14 (16.7) |
|
|
Gestational diabetes & Diabetes mellitus |
17 (18.7) |
10 (11.9) |
|
|
Gestational hypertension & preeclampsia |
23 (25.3) |
18 (21.4) |
|
|
Severe gestational hypertension & preeclampsia |
6 (6.6) |
5 (6.0) |
|
|
Chronic hypertension |
1 (1.1) |
3 (3.6) |
|
|
Oligohydramnios |
2 (2.2) |
5 (6.0) |
|
|
Fetal growth restriction |
1 (1.1) |
2 (2.4) |
|
|
Cholestasis of pregnancy |
1 (1.1) |
1 (1.2) |
|
|
Other: Category 2 tracing Hyperthyroidism Polyhydramnios |
3 (3.3) |
3 (3.6) |
|
a Data are shown as median (interquartile range).
Table 1- Baseline demographic and current pregnancy data
Table 2 describes outcomes related to Foley catheter duration and time to delivery. As determined by design of this study, there was a statistically significant difference in time to catheter expulsion between the “Fast FB” and “Slow FB” groups (2.70±1.0 vs 6.8±2.4 hours, P<0.001). In regards to our primary outcome, we found no statistically significant difference in time to delivery following Foley catheter expulsion between groups. Patients in the “Fast FB” group delivered, on average, in 22.8±12.1 hours following Foley catheter expulsion while the “Slow FB” group delivery in 23.4±12.6 hours on average (P=0.77).
|
Characteristic |
Cervical ripening ≤4 hours (N= 91) |
Cervical ripening >4 hours (N = 84) |
P value |
|
FB duration |
|
|
|
|
Time to catheter expulsion, hrb |
2.70 +/- 0.96 |
6.77 +/- 2.40 |
<0.001 |
|
Bishop score at time of catheter insertiona |
3 (2, 4) |
2.5 (0, 3.8) |
0.01 |
|
Bishop score at time of catheter expulsiona |
6 (5, 8) |
7 (5, 8) |
0.87 |
|
|
|
|
|
|
Delivery |
|
|
|
|
Mean time to delivery after catheter expulsion, hrb |
22.84 +/- 12.10 |
23.39 +/- 12.64 |
0.77 |
|
Delivery within 24 hrs, n (%) |
51 (56.0) |
33 (39.3) |
0.03 |
|
Mean time to vaginal delivery after catheter expulsion, hrb |
20.45 +/- 11.36 |
21.37 +/- 12.39 |
0.68 |
|
Vaginal delivery within 24 hr, n (%) |
41 (66.1) |
25 (48.1) |
0.05 |
|
|
|
|
|
|
Mode of delivery, n (%) |
|
|
0.52 |
|
Vaginal delivery |
62 (68.1) |
52 (61.9) |
|
|
Vacuum assisted vaginal delivery |
2 (2.2) |
1 (1.2) |
|
|
Forceps assisted vaginal delivery |
4 (4.4) |
2 (2.4) |
|
|
Cesarean delivery |
23 (25.3) |
29 (34.5) |
|
|
|
|
|
|
|
Primary Indication for cesarean delivery, n (%) |
|
|
0.84 |
|
Failed induction |
6 (27.3) |
9 (31.0) |
|
|
Arrest of dilation |
7 (31.8) |
6 (20.7) |
|
|
Arrest of descent |
5 (22.7) |
8 (27.6) |
|
|
Fetal intolerance of labor |
5 (18.2) |
6 (20.7) |
|
a Data are shown as median (interquartile range).
b Data are shown as mean ± standard deviation.
Table 2- Foley Balloon cervical ripening duration and delivery outcomes
There was a marginally significant difference in the incidence of vaginal delivery within 24 hours (66.1% vs 48.1%, P=0.05). We noted a significant difference in Bishop score at time of insertion (median, 3; range, 2-4 vs median, 2.5; range, 0-3.75; P=0.01) but no difference in Bishop score at time of expulsion (median, 6; range 5-8 vs median, 7; range 5-8; P=0.87).
We noted no differences in mode of delivery, indication for cesarean delivery (Table 2), as well as no difference in the incidence of postpartum hemorrhage (Table 3). However, we did find a significant difference in the incidence of intrauterine infection between groups (38.5% vs 22.6%, P=0.02).
There were no differences in methods for membrane rupture, methods for labor augmentation, or use of analgesia (Table 3). Lastly, there were no differences in neonatal outcomes (Table 4).
|
Characteristic |
Cervical ripening ≤4 hours (N= 91) |
Cervical ripening >4 hours (N = 84) |
P value |
|
Rupture of membranes before delivery, n (%) |
|
|
0.16 |
|
Artificial |
50 (54.9) |
55 (65.5) |
|
|
Spontaneous |
41 (45.1) |
29 (34.5) |
|
|
|
|
|
|
|
Labor augmentation, n (%) |
|
|
0.12 |
|
Amniotomy |
2 (2.2) |
5 (6.0) |
|
|
Pitocin |
39 (42.9) |
24 (28.6) |
|
|
Both |
48 (52.7) |
50 (59.5) |
|
|
None |
2 (2.2) |
5 (6.0) |
|
|
|
|
|
|
|
Analgesia used during labor, n (%) |
|
|
0.40 |
|
None |
1 (1.1) |
0 (0.0) |
|
|
Epidural |
89 (97.8) |
84 (100.0) |
|
|
Pudendal block |
1 (1.1) |
0 (0.0) |
|
|
|
|
|
|
|
Intrauterine infection, n (%) |
35 (38.5) |
19 (22.6) |
0.02 |
|
|
|
|
|
|
EBLa |
|
|
|
|
Vaginal delivery |
Median 350 (300, 450) |
Median 300 (300, 400) |
0.08 |
|
Cesarean delivery |
Median 700 (500, 800) |
Median 650 (500, 800) |
0.99 |
|
|
|
|
|
|
PPH, n (%) |
7 (7.7) |
7 (8.3) |
0.88 |
|
|
|
|
|
|
Total Length of Staya |
3 (3, 4) |
3 (3, 4) |
0.21 |
a Data are shown as median (interquartile range).
Table 3- Labor outcomes
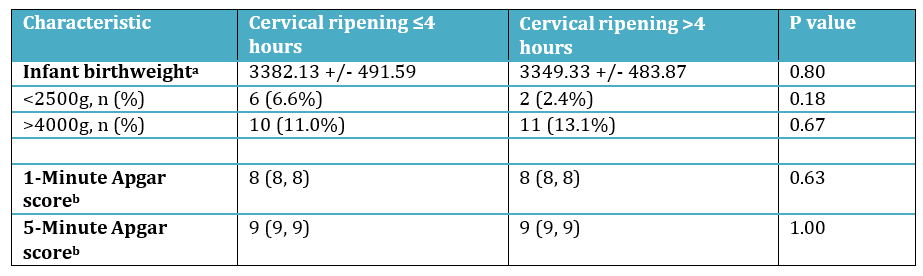
a Data are shown as median (interquartile range).
b Data are shown as mean ± standard deviation
Table 4- Neonatal outcomes
Discussion
We found no significant difference in time to delivery following Foley catheter expulsion when comparing a longer duration of cervical ripening to a shorter duration of cervical ripening. In addition, the duration of Foley catheter for cervical ripening does not affect the rate of cesarean delivery or incidence of postpartum hemorrhage. We also noted a marginally significant difference in the incidence of vaginal deliveries within 24 hours (66.1% vs 48.1%, P=0.05). These findings suggest that the total duration of labor may be shortened if the duration of Foley catheter cervical ripening is expedited.
An anecdotal belief is that the application of tension on Foley catheters during cervical ripening facilitates quicker expulsion. Published reports suggest that the application of tension results in a shorter time to expulsion with no effect on the total duration of labor [10,11]. However, the time to Foley catheter expulsion, even in their control groups, was shorter than the parameters set by our study [mean 2.6 hours [10]; median 4.6 hours [11]. Therefore, differences in total duration of labor may exist when comparing longer durations of Foley cervical ripening to shorter durations, as suggested by our study.
In addition, in the previously referenced studies, heterogeneity exists with regards to the patients included in their studies. The inclusion of multiparous patients, patients admitted with spontaneous rupture of membranes, and patients undergoing concomitant cervical ripening with multiple types of pharmacologic methods are conditions that could inadvertently shorten the duration of cervical ripening and the total duration of labor [6,12].
Our study only included nulliparous patients with intact membranes 253 to exclude this possibility. We found significantly more intrauterine infections in the “Fast FB” group compared to the “Slow FB” group (38.5% vs 22.6%, P=0.02). This finding may represent a Type 1 error. In this study, the presence of an intrauterine infection was inferred by noting the presence of standard antibiotic treatment regimens for endomyometritis in the medication administration record. A systematic review published by Heinemann, et al., 2008 suggests that Foley catheters alone for cervical ripening are associated with an increased rate of maternal infection when compared to patients who received prostaglandins (OR, 1.38; 95% CI 1.12-1.68) [13]. Regardless, this subset of patients in our study warrants further investigation.
A major strength of this study was our ability to access the complete medical records of our study population. However, our ability to abstract data depended on accurate documentation. Another strength of our study is the inclusion of only nulliparous patients with intact membranes and unfavorable Bishop Score who only received a Foley catheter and Misoprostol for cervical ripening. This allowed us to limit the heterogeneity of our study population while studying a clinically relevant protocol for pre-induction cervical ripening. A limitation of our study is the significant difference in pre-induction Bishop Score between “Fast FB” and “Slow FB” groups (median, 3; range, 2-4 vs median, 2.5; range, 0-3.75; P=0.01). This finding may not be clinically significant but could account for the difference in duration of cervical ripening as the “Slow FB” group required more time to achieve the same post- expulsion Bishop Score as the “Fast FB” group.
In conclusion, this study demonstrated no significant difference in time to delivery following Foley catheter cervical ripening when comparing a longer duration of cervical ripening to a shorter duration of cervical ripening. Therefore, efforts to shorten the total duration of labor should focus on expediting the duration of Foley catheter cervical ripening.
Conflicts of Interest
The authors have no financial disclosures or conflicts of interest.
References
- American College of Obstetricians and Gynecologists. (2009). ACOG practice bulletin no. 107: induction of labor. Obstet Gynecol, 114, 386-397.
- Osterman, M. J., & Martin, J. A. (2014). Recent declines in induction of labor by gestational age (No. 2014). US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
- Clausson, B., Cnattingius, S., & Axelsson, O. (1999). Outcomes of post-term births: the role of fetal growth restriction and malformations. Obstetrics & Gynecology, 94(5 Part 1), 758-762.
- Yudkin, P. L., Wood, L., & Redman, C. W. G. (1987). Risk of unexplained stillbirth at different gestational ages. The Lancet, 329(8543), 1192-1194.
- FELDMAN, G. B. (1992). Prospective risk of stillbirth.Obstetrics & Gynecology, 79(4), 547-553.
- Bishop, E. H. (1955). Elective induction of labor. Obstetrics & Gynecology, 5(4), 519-527.
- Bishop, E. H. (1964). Pelvic scoring for elective induction(Doctoral dissertation).
- Boulvain, M., Kelly, A., Lohse, C., Stan, C., & Irion, O. (2001). Mechanical methods for induction of labour. The Cochrane database of systematic reviews, (4), CD001233- CD001233.
- Gelber, S., & Sciscione, A. (2006). Mechanical methods of cervical ripening and labor induction. Clinical obstetrics and gynecology, 49(3), 642-657.
- Gibson, K. S., Mercer, B. M., & Louis, J. M. (2013). Inner thigh taping vs traction for cervical ripening with a Foley catheter: a randomized controlled trial. American journal of obstetrics and gynecology, 209(3), 272-e1.
- Fruhman, G., Gavard, J. A., Amon, E., Flick, K. V., Miller, C., & Gross, G. A. (2017). Tension compared to no tensionon a Foley transcervical catheter for cervical ripening: a randomized controlled trial. American journal of obstetrics and gynecology, 216(1), 67-e1.
- Amorosa, J. M., Stone, J., Factor, S. H., Booker, W., Newland, M., & Bianco, A. (2017). A randomized trial of Foley bulb for labor induction in premature rupture of membranesin nulliparas (FLIP). American Journal of Obstetrics and Gynecology, 217(3), 360-e1.
- Heinemann, J., Gillen, G., Sanchez-Ramos, L., & Kaunitz,A. M. (2008). Do mechanical methods of cervical ripening increase infectious morbidity? A systematic review. American journal of obstetrics and gynecology, 199(2), 177-188.