
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2020) Volume 5, Issue 2
Does the Physical Therapy Intervention Improve Female Sexual Dysfunction in Saudi Society?
Received Date: Apr 21, 2020 / Accepted Date: Apr 29, 2020 / Published Date: May 11, 2020
Copyright: ©Najwa Alfarra PhD PT, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Sexual dysfunction refers to a problem occurring during any phase of the sexual response cycle that prevents the individual or couple from experiencing satisfaction from the sexual activity. The sexual response cycle traditionally includes excitement, plateau, orgasm, and resolution. Desire and arousal are both part of the excitement phase of the sexual response. The literature review confirmed that the sexual dysfunction is common, 43 % of women and 31 % of men report some degree of difficulty, it is a topic that many people are hesitant to discuss. But the treatment options are available [1]. The literature also supports the use of pelvic floor exercise in order to improve sexual function. The health concept for women magazine reported that the Neo-control magnetic chair improved the sexual dysfunctions in women specially the orgasm problems [2].
Objective: The objective of the study is to explore the role of the physical therapy intervention for the female sexual dysfunction in Saudi Arabia.
Methods: Thirty women had sexual dysfunction, were evaluated by muscle power (Oxford scale) before and after the treatment, and FSFI questioners were answered before and after the completion of the treatment.
Main Outcome Measures: The domain scores of the female sexual function index (FSFI), included desire, arousal, lubrication, orgasm, satisfaction, and pain, were calculated. The supervised pelvic floor muscle training, core strengthening pelvic exercises were conducted for 30 minutes, and magnetic field “neocontrol chair” frequency 50HZ, 15 sec. on, 1 sec. off for 20 min. power 75-80%, twice a week for six weeks(12 sesssions). Muscle power (Oxford scale) was measured before and after the treatment.
Results: All subjects successfully completed the study with no adverse events significant improvement in sexual function as assessed by the FSFI, sex desire improved by 80%, sexual arousal improved by 86%, lubrication and orgasm improved by 80%, general satisfaction 87%, 73% pain free through intercourse. Muscle power were improved from 1-2 out of 5 to 3+ out of 5.
Conclusion: The physical therapy intervention which include pelvic floor exercise, core strengthening exercise and magnetic field had improved the sexual function in female Saudi society
Keywords
Femal Sexual Dysfunction, Magnetic Field Treatment, Pelvic Floor Exercise, Physical Therapy Intervention, Strengthening Exercises
Introduction
The promotion of sexual function with optimal satisfaction and minimal distress has become an objective of various disciplines within the field of medicine. Healthy sexual life requires mental, physical, and well-being. The problem that might limit sexual activity include the flowing: decrease in genital circulation, alterations in sensation and chronic pelvic pain. Talli Y, reported that medical treatment of sexual problems includes a multidisciplinary team such as mental health, sexual therapy, medication, lifestyle change such as diet and exercise, Herbs, and surgical intervention [3]. Physical therapy in the context of sexual health takes a holistic approach and includes treatment of the pelvic floor muscles that support the spine, pelvis, and internal organs. To effectively address pelvic floor dysfunction, a thorough understanding of pelvic floor anatomy and physiology is essential. The women’s health Physical therapist will evaluate the patient to determine the source of dysfunction, provide scientifically supported education regarding positioning to decrease pain, providing different modalities of treatment to restore function, improve mobility, and relieve pain and prevent or limit permanent physical disabilities of patients suffering from injuries and disease, instructed the patient with certain exercise program, and assist alleviating the symptoms to achieve optimal sexual function, and treat the patient’s dysfunction and improve their sexual intimacy limitations [4]. The symptoms presentations that limit optimal sexual function in our study include stress incontinence, mixed incontinence, genital pain and decrease achievement of orgasm. There were a lot of studies performed in that field, and they found the pelvic floor muscle exercise, significantly improved pain with intercourse, sexual function, and general quality of life in women [5,6]. The aim of the study to investigate the effectiveness of pelvic floor rehabilitation (which will include the pelvic floor muscle training, core strengthening pelvic exercises, and magnetic field “Neocontrol chair”) on sexual dysfunction in the Saudi Society.
Mgnetic Field (Neocontrol Chair)
The first clinical application of magnetic fields for stimulating pelvic floor muscles (PFMs) was by Galloway, et al. this study involved use of the Neocontrol pelvic floor therapy system in the treatement of incontinence [7]. This therapy system comprises a wooden chair incorporating a coil within its seat that generats a magnetic field capable of penetrating the pelvis. If the intensity is sufficient, this magnetic field-generating chair can produce a contraction of the PFMs. Transcutaneous magnetic nerve stimulation (TMNS) involves use of a magnetic field generator located outside the body to induce current within the body [8].
The Mechanism of Electrical Stimulation and Magnetic Stimulation
The mechanism for both of them had the same physiological effects by enhancing the membrane gases exchanges and enhancing the metabolic rate of the tissue causes muscle contraction. When the electrical stimulation is used to stimulate the pelvic floor musles the part to be treated must be exposed, and the vaginal or rectal tissue must be sufficiently healthy to tolerat the electrode application. Furthermore, the insertion of electric probes is often uncomfortable; electrical current induced by ES weaken due to the impedance of the tissues between the electrodes ; the pedundule nerve, strong ES is required during therapy that will lead to discomfort and pain of the skin, vagina and/or anus. In contrast to electric current, magnetic field therapy does not require exposure of the part, has no direct coupling of magnetic applicator to the patient, and involves penetrates all tissues. Therefore, a lower intensity of the stimulation can be used leading to fewer complaints [9].
Methods
This is a prospective study done in a primary care setting within a tertiary referral hospital. The prospective cohort study was meant to assess 30 women, who were aged 20-60 years old with sexual dysfunction in Saudi Arabia society. Confirmed by patient history and by answering the Female Sexual Function Index (FSFI) Arabic Validated version by Anis, et al. The participants included married, non-pregnant, no mental or health problem [10]. Excluded any neurological or oncology cases. The study took exactly one year.
All patients had physically interviewed at the physical therapy department outpatient waiting area by one of our junior therapist asked them to answer the Female Sexual Function Index (FSFI) Arabic Validated version questionnaires, if the patient had a problem with sexual dysfunction, the therapist will contact the referring physician to complete the automated physical therapy referral through ICIS and will take the verbal approval from the patient to be involved in the study and will take the first appointment for the evaluation, which will include history, physical examination, PFM strength examination by Oxford grading scale 0-1 if patients were not able to contract their PFM, Grade 2 if patients performed only an insufficient contraction, and grades 3-4 if patients were able to contract their PFMs properly. All muscles of the pelvic floor were investigated, education will be given in the first session about the anatomy of the pelvic floor muscles by using mirror and the patient will be teaching about the sexual different position in order to decrease pain.
The patient were seen 12 sessions each session 50 min which will include 15 min pelvic floor exercise and another 15 min core strengthening pelvic exercises, 20 min magnetic field frequency 50HZ, 15 sec. on, 1 sec. off for 20 min. power 75-80 % twice/ week. (total 12 sessions).
Proper methods were used to teach the patient the proper PFM contraction such as: First one, observation of correct PFM contraction as squeeze around the urethral, vaginal, and anal openings and inward lift that could be observed at the perineum by using mirror. Second, vaginal palpation: this technique was described by Kegel as a method to evaluate PFM function. By placing one finger in the distal third of the vagina and asked the women to lift inward and squeeze around the finger. Kegel did not use this method to measure PFM strength. He used vaginal palpation to teach women how to contract their PFM and classified the contraction qualitatively as correct or not correct [11]. The patient taught Isometric adductors strengthening exercises, Straight leg raising with PFM muscles activation, pelvic curling with Pelvic floor muscles training, lower limbs cycling exercises, happy baby stretching, butterfly stretching exercise, and garland stretching exercise. The patient instructed to do each exercise ten repetition twice per day.
Main Outcome Measures
The Subjective Outcomes: All the participants completed the Female Sexual Function Index (FSFI) Arabic validated version by Anis. Before commencing the treatment and after six weeks of completing the treatment, and each domain score, including desire, arousal, lubrication, orgasm, satisfaction, and pain was calculated.
Objective Outcomes: The pelvic floor muscle strength were measured by Oxford grading scale before and after the treatment.
Results
Distribution of the participant women according to some of their descriptive was presented in Table 1. It was found out that 80% of the women graduated from secondary school and higher, 76.7% of them work, it was seen that 50% of the partcipant women were aged > 44 years, and 50% < 44years, 77% of them had their last birth as vaginal delivery and 87% had episiotomy, average age was 44 years, and average number of pregnancies was 4 (Table 1).
Table 1: Distribution of the Women According to their Descriptive Characteristics
|
Features |
n |
% |
|
Education |
|
|
|
Elementary school |
6 |
20 |
|
Secondary and higher |
24 |
80 |
|
Working status |
|
|
|
Working |
23 |
76.7 |
|
Not working |
7 |
23.3 |
|
Age |
|
|
|
44 and under |
15 |
50 |
|
44 and higher |
15 |
50 |
|
Last delivery method |
|
|
|
Vaginal |
23 |
77 |
|
Cesarean |
7 |
23 |
|
Episiotomy |
|
|
|
Yes |
26 |
87 |
|
No |
4 |
13 |
|
Number of pregnancy |
4 +/- 2 |
|
When urinary incontinence causes of the participant women were examined; it was seen in 70% of them, about half of those women abstained from sexual intercourse due to urinary incontinence. The sexual functions of those who were > 44 years and had >4 pregnancies and had their last birth as vaginal delivery were more problematic as compared to those who were <44 years, had <3 pregnacies and had their last birth as cesarean delivery. It was expected that sexual functions of those who had episiotomy during delivery would be more problemic as compared to those who did not have episiotomy during delivery and the result confiremed that.
Female sexual dysfunction are prevalent in Kingdom of Saudi Arabia which threaten women’s quality of life, FSFI questionnaire showed that all of the participants in the study had one or more domin of sexual dysfunction. Sexual dysfunction had been classically divided into six domin instrument measuring: desire, arousal, lubrication, orgasm, global satisfaction, and sexual pain as propsed by Rosen, et al. [12].
In this study, sexual desire disorder was diagnosed in the thirty women 100%. Twenty two women 7% had desire disorder due to Interpersonal relationship issues, 20 women 66% due to partner performance problems, lack of emotional satisfaction with the relationship, and 8 women 27% due to birth trauma and had episiotomy. While, sexual arousal disorder was identified in thirty participants with different degree eighteen women 60% the arosal is moderate, ten women 33% found it low, and two 6% never felt aroused during sexual activity, due to the following factors anxiety or depression. Stress, such as work stress and poor body image.
Furthermore, lubrication disorder affected all the participants, fifteen women 50% found it very difficult to maintain lubricant during intercourse due to insufficient excitement and stimulation, 50% of them are able to keep themselves wet until the completion of sexual activity. Orgasm disorder in four women 13% had never reach orgasm, 50% of them less than half of the time had orgasm, and eleven 37% about have of the time had orgasm. Due to many factors such as: Boredom in sexual activity or a relationship, Fatigue and stress or depression,painful intercourse, and Lack of knowledge about sexual function.
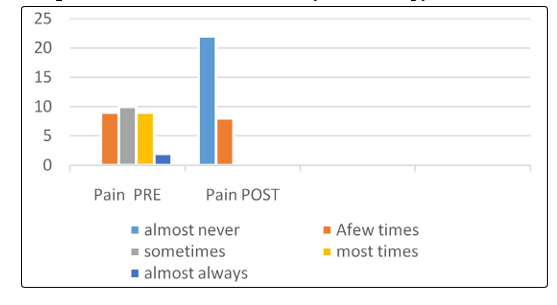
Overall satisfaction four women 13% moderately disatisfied, eighteen women 60% about equally satisfied and dissatisfied, and eight women 27% moderately satisfied, the reason behind that most of them reported that their partner is dissatisfied with their sex life because of pelvic floor muscles weakness post-natal. Additional, sexual pain about three women 10% had always pain, fourteen women 47% most of the time complain of pain, tweeleve women 40% had moderate pain, and one women 3% had very low or no pain at all during intercourse, due to lack of sexual arousal, injury to the pelvic floor muscles, connective tissue, or fascia as a result of a birth trauma, or episiotomy during vaginal delivery. This can lead to shorten and weak PFM, with muscle trigger points and restrication of connective tissue.
The FSFI questionnaiers completed before and after the treatment showed successful outcome in all the participants. It is evident that the physical therapy intervention is crucial to improve sexual desire by 80%, sexual arousal by 86%, improve both lubrication and orgasm by 80%, increase general satisfaction by 87%, and 73% pain free though intercourse as compared with the percentage obtained before the physical therapy intervention. In summary, the physical therapy intervention increased women’s sexual satisfaction as it shown in Figure 1 to 6.
Figure 1: Sexual Desire Pre-Post Physical Therapy Intervention
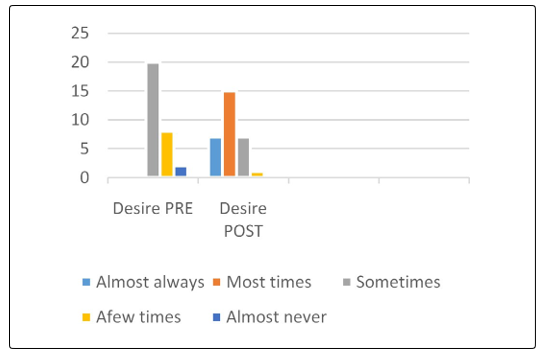
Figure 2: Sexual Arousal Pre-Post Physical Therapy Intervention
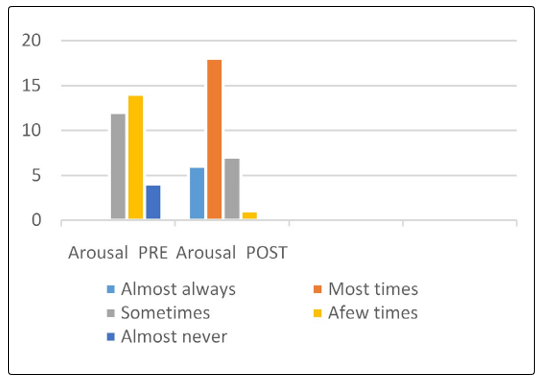
Figure 3: Sexual Lubrication Pre-Post Physical Therapy Intervention
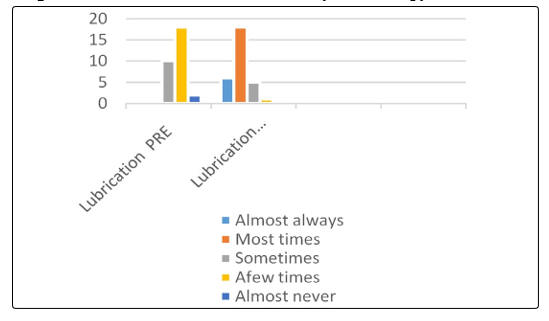
Figure 4: Sexual Orgasm Pre-Post Physical Therapy Intervention
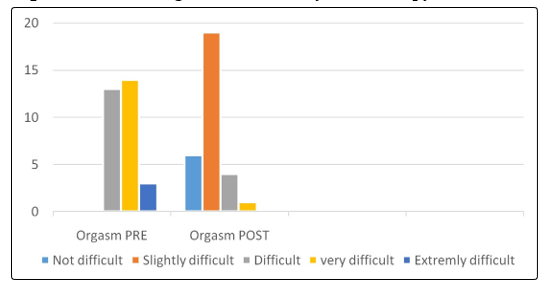
Figure 5: Sexual Satisfaction Pre-Post Physical Therapy intervention
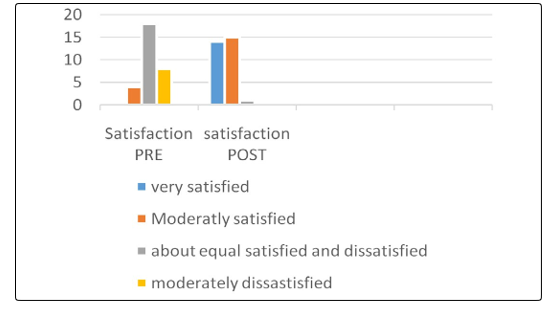
Figure 6: Sexual Pain Pre-Post Physical Therapy Intervention
Muscle power of the pelvic floor muscles were measured before and after the treatment and there are huge improvement as shown in Table 2.
Table 2: A Comparison of the Pelvic Floor Muscle Power Before and After the Treatment
|
Case # |
MP. Before the treatment |
MP. After the treatment |
|
Case 1 |
2/5 |
3/5 |
|
Case 2 |
2/5 |
3/5 |
|
Case 3 |
2/5 |
3/5 |
|
Case 4 |
2/5 |
3/5 |
|
Case 5 |
1/5 |
3/5 |
|
Case 6 |
2/5 |
3/5 |
|
Case 7 |
2-/5 |
3/5 |
|
Case 8 |
2/5 |
3/5 |
|
Case 9 |
2/5 |
3/5 |
|
Case 10 |
2-/5 |
3/5 |
|
Case 11 |
2/5 |
3/5 |
|
Case 12 |
2/5 |
3/5 |
|
Case 13 |
2/5 |
3/5 |
|
Case 14 |
2-/5 |
3/5 |
|
Case 15 |
1/5 |
3-/5 |
|
Case 16 |
1/5 |
3-/5 |
|
Case 17 |
3-/5 |
3+/5 |
|
Case 18 |
2/5 |
3/5 |
|
Case 19 |
2+/5 |
3+/5 |
|
Case 20 |
2-/5 |
3/5 |
|
Case 21 |
1/5 |
3-/5 |
|
Case 22 |
2/5 |
3/5 |
|
Case 23 |
3/5 |
3+/5 |
|
Case 24 |
2/5 |
3/5 |
|
Case 25 |
2+/5 |
3/5 |
|
Case 26 |
3/5 |
3+/5 |
|
Case 27 |
1/5 |
3-/5 |
|
Case 28 |
2+/5 |
3/5 |
|
Case 29 |
2-/5 |
3/5 |
|
Case 30 |
2/5 |
3/5 |
Discussion
In the current study ; it was noted that 70% of the partcipant women had urinary incontinence and this problem affected women’s sexual lives negatively; that goes with Salonia, et al. found that 46% of the women who had urinary incontinence complain of certain type of sexual dysfunction, 34% of them experienced decreased sexual desire, 23% of them underwent sexual arousal dysfunction, 11% of them could not achieve orgasm and 44% of them had pain as compared with those healthy women [13]. The study of Ozerdogan, et al. pointed out that sexual dysfunction occurred more among those who gave birth with vaginal delivery than those who gave birth with cesarean delivery, which is confirmed in the current study [14].
All the participants treated with PFMT, core strengthening pelvic exercises and magnetic field “neocontrol chair” showed major improvement in their sexual function, that goes in contrast with Weiss, et al. reported that regular pelvic floor exercises training in-clinic and at home augments the support function of the pelvic floor, enhances blood flow, and stimulates PFM proprioception, contributing to more intense orgasm [15]. Brotto, et al. in longitudinal prospective study [5]. Sadownik, et al. in a qualitative retrospective study [16]. Bo K, et al. RCT supported that the use of pelvic floor exercise improves sexual function; and Goldenfinger, et al. in an RCT; emphasize the efficacy of pelvic floor muscle training for sexual dysfunction [17,18]. Furthermore, Aydin, et al. found that vaginal electrical stimulation improved the sexual experience of women who scored low on FSFI, That goes inconsitant with Guiseppe, et al. reported that pelvic muscle electrical stimulation, a form of strengthening used regularly in muscle rehabilitation, improved sexual function and urinary incontinence [19,20].
Additionally, in Turkish study by Beji, et al. improvement in sexual desire, and achievement of orgasm were reported in women who received pelvic floor rehabilitation; Graber and Kline reported that there are a positive correlations between the strength of women’s pelvic muscles and the intensity of her orgasmic response, in conjuction with that Chambless et al. suggested that strong pelvic floor muscles were crucial for the attainment of orgasm [21-23].
Finally, Wurn et al. reported that physical therapy administered for the pelvic floor muscles improved sexual function in women [24]. Giuseppe, et al. reported that electrical stimulation for the pelvic floor muscles improved sexual dysfunction [25]. Nappi, et al. found that the use of electrical stimulation (ES) on the vestibular area and vaginal introits in women with sexual pain disorders [26]. It is effective in the management of sexual pain disorders. Furthermore, Sayıl I and Berman et al. found that Pelvic floor muscles play important roles in sexual arousal, sexual response and sexual satisfaction of women [27,28]. Hypertonic or hypotonic structure of these muscles may lead to problems during sexual intercourse or orgasm and urinary incontinence.
Conclusion
The physical therapy intervention is beneficial to improve sexual function and have no adverse effects. Further study is required with bigger sample size and randomized control trial.
References
- American Academy of Family Physicians/American Family Physician-Female Sexual Dysfunction: Evaluation and Treatment.
- Health concept for women & men https://www.prostata-therapie.de/en/the-health-concept-for-men/prostate-inflammation-and-urinary-incontinence/neocontrol/
- Rosenboum, TY (2008) Physical therapy in female sexual dysfunction. Current sexual health reports 5: 97-101.
- US Department of Labor, Bureau of Statistics: Occupational Outlook Handbook, 2004-2005 Edition. Washington, DC: US Department of Labor; 2004. Bulletin 2540.
- Brotto LA, Yong P, Smith KB, Sadownik LA (2015) Impact of a multidisciplinary vulvodynia program on sexual functioning and dyspareunia. J Sex Med 12: 238-247.
- Eftekhar T, Sohrabi M, Haghollahi F, Mamak Shariat, Elahe Miri (2014) Comparison effect of physiotherapy with surgery on sexual function in patients with pelvic floor disorder: a randomized clinical trial. Iran J Reprod Med 12: 7-14.
- Galloway NT, El-Galley RE, Sand PK, Appell RA, Russell HW, et al. (1999) Extracorporeal magnetic innervation therapy for stress urinary incontinence. Urology 53: 1108-1111.
- Neotonus Corporation (2006) Neocontrol®. Internet site: http://www.neotonus.com/urology_gynecology/index.htm Accessed 15 April 2005.
- Chandi DD, Groenendijk PM, Venema PL (2004) FMS. BJU Int 93: 539-542.
- Anis T, Gheit SA, Saied HS, Alkherbas SA, (2011).Arabic translation of female sexual dysfunction index validation in an Egyption population. J sex Med 8: 3370-3378.
- Morkved S, Bo K (2014) . Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinency: a systematic review. Br J Sports Med 48: 299-310.
- Rosen, Brown, Heiman, Leiblum, Meston, et al. (2000) The Female Sexual Function Index (FSFI): Amultidimensional self-report instrument for the assessment of female sexual function. Journal of sex & marital therapy 26: 191-208.
- Salonia A, Briganti A, Gallina A, Giuseppe Zanni MD, Federico Dehò et al. (2007) Lower urinary tract symptoms and sexual dysfunction in women. Curr Sex Health Rep 4: 85-90.
- Ozerdogan N, Beji NK, Yalcin O (2004) Urinary incontince: its prevalence, risk factors and effects on the quality of life of women living in a region of Tureky. Gynecology obstet invest 58: 145-150.
- Weiss PM, Rich J, Swisher E (2012) Pelvic floor spasm: the missing link in chronic pelvic pain. Contemporary OB/GYN October 1, http://contemporaryobgyn.modernmedicine.com.
- Sadwnik LA, Seal BN, Brotto LA, Provoked Vesitibulodynia (2012) Women’s experience of participanting in a multidisciplinary vulvodynia program. J Sex Med 9: 1086-1093.
- Bo K, Talseth T, Vinsnes A (2000) Randomized controlled trial on the effect of pelvic floor muscle training on quality of life and sexual problems in genuine stress incontinent women. Acta Obstet Gynecol Scand 79: 598-603.
- Goldenfinger C, Pukall CF, Thibault-Gagnon S, Mc Lean L, Chamberlain S (2016) Effectiveness of cognative-behavieral therapy and physical for provoked vestibulodynia: a randomized pilot study. J sex Med 13: 88-94.
- Ayden S, Arioglu Aydin C, Batmaz G, Dansuk R (2016) Effect of vaginal electrical stimulation on female sexual functions: a randomized study. J Sex Med 13: 88-94.
- Giuseppe PG, Pace G, Vicentini C (2007) Sexual function in women with urinary incontinence treated by pelvic floor transvaginal electrical stimulation. J Sex Med 4:702-707.
- Beji NK, Yalcin O, Erkan HA (2003) The effect of pelvic floor training on sexual function of treated patients. Int Urogynecol J Pelvic Floor Dysfunct 14: 234-2348.
- Graber G, Kline-Graber G (1979) Female orgasm: role of the pubococcygeus muscle. J Clin Psychiatry 40: 348-351.
- Chambless DL, Sultan FE, Stern TE, O’Neill C, O’Neill C, Garrison S et al. (1984) Effect of pubococcygeal exercise on coital orgasm in women. J Consult Clin Psychol 52: 114-118.
- Wurn LJ, Wurn BF, King CR, Roscow AS, Scharf ES et al. (2004) Increasing orgasm and decreasing dyspareunia by a manual physical therapy technique. MedGenMed 6: 47.
- Giuseppe PG, Pace G, Vicentini C (2007) Sexual function in women with urinary incontinence treated by pelvic floor transvaginal electrical stimulation. J Sex Med 4: 702-707.
- Nappi RE, Ferdeghini F, Abbiati I, Vercesi C, Farina C et al. (2003) Electrical stimulation (ES) in the management of sexual pain disorders. J Sex Marital Ther 29: 103-110.
- Sayıl I (1996) Mental health and disease textbook. Ankara: Antıp Corporation 257-263.
- Berman JR, Adhikari S, Goldstein I (2000) Anatomy and physiology of female sexual function and dysfunction: Classifıcation, evaluation, and treatment options. Eur Urol 38: 20-29.