
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2023) Volume 5, Issue 1
Distribution of Cancer of the Skin and Cancer of the Urinary Bladder in Jamaica 2008
Received Date: Mar 30, 2023 / Accepted Date: Apr 20, 2023 / Published Date: Apr 24, 2023
Copyright: ©LA McLish. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mclish, L. A. (2023). Distribution of Cancer of the Skin and Cancer of the Urinary Bladder in Jamaica 2008. Adv J Uro Nephro, 5(1), 02-08.
Abstract
Objective: To examine the distribution of cancer of the skin and cancer of the urinary bladder in Jamaica 2008.
Methods: The study included all fourteen parishes. Data was obtained from the Jamaica Cancer Registry located in the Pathology Department of the University of the West Indies. Population denominators were obtained from the 2011 census taken by the Statistical Institute of Jamaica. The statistical package which was used to analyze the data was SPSS.
Results: The age distribution of cancer of the skin in Jamaica 2008 revealed that the highest frequencies occurred in the age group 45 years to 84 years when both genders were considered together. The results also showed that after age 85 years the risk of developing cancer diminishes. The crude incidence rate (CIR) of melanoma in males in Jamaica 2008 was determined to be 2.6 and in females 2.5. These crude incidence rates were comparable to Southern Africa. This present study determined the mean age for developing cancer of the skin was 60.8 years when both genders are considered. This reveals that the risk of developing melanoma increases with age. Based on the CIR the distribution of melanoma across some parishes was the following. In decreasing order Kingston and St. Andrew (6.2), St. Mary (2.6), St. Ann (2.3), St. Catherine (2.1) and St. Thomas (2.1).
In the case of urinary bladder cancer (UBC), the highest frequency occurred in the age group 60 years to 84 years. The mean age for developing UBC was 70.7 years in Jamaica 2008. The CIR of UBC in men in Jamaica 2008 was 2.8 while in the case of women it was 0.8, (male/female ratio, 3.5).The CIR ratio was comparable to the probability ratio in the United States of America in 2018. The distribution of UBC was examined across all parishes using the CIR as a means of comparing objectively. When ranked in descending order it was Kingston and St. Andrew (3.3), St. Mary (2.6), St. Catherine (2.5), Portland (2.4) and St. Ann (1.7). It should also be emphasized of the 48 persons who were diagnosed with UBC, 6 were smokers and only 1 was female. Hence in Jamaica 2008 smoking does not appear to be a primary risk factor in developing UBC.
Conclusion: The health administrators should promote primary prevention to reduce the financial burdens associated with developing cancers taking into account the age groups when these cancers become more prevalent and the geographical locations where the CIR is high. This is especially important in the case of UBC.
Introduction
Since the inception of the Jamaica Cancer Registry in 1958 the incidence of cancer in Jamaica has been monitored by reports be¬ing produced regularly [1]. These reports are based upon the inci¬dence of cancer in males and females in Kingston and St. Andrew which forms the population base of the registry [1,2]. Gibson et al. (2008), determined that in the case of males for the period 1998 to 2002 a crude incidence rate of 0.5 for melanoma of the skin [1]. They also calculated the crude incidence rate for cancer of the urinary bladder for the same time period, this was determined to be 3.1 for males. In the case of females for the same time period 1998 to 2002, the crude incidence rate of melanoma of the skin was 4.5 and for that of the urinary bladder this was 2.
This present study has been undertaken to determine the distri-bution of cancer of the skin and cancer of the urinary bladder in Jamaica 2008.
Methods
Study Population
This research project consists of persons from all parishes in Jamaica. A map of Jamaica is shown in Figure 1 [3].
Figure 1: Map of Jamaica showing all the Parishes
Data was obtained from the Jamaica Cancer Registry located in the Pathology Department of the University of the West Indies. The methodology of the registry has been previously stated [4,5]. Cases are registered from information gleaned from public and private hospitals and general practitioners in Kingston and St. An-drew then verified by pathologists at Jamaica Cancer Registry in accordance with standard techniques of registration [6].
Data Extraction
Variables that were obtained from the Jamaica Cancer Registry included cancer code, date of diagnosis, age at diagnosis, perma-nent residence, parish of birth, diagnosis, gender, smoker, source of case and date of death. The codes used for classification of the various types of cancers were cross-checked using the tenth edi¬tion of the International Statistical Classification of Diseases and Related Health Problems (ICD – 10) [7]. Population denominators were obtained from the 2011 census taken by the Statistical Insti¬tute of Jamaica, Kingston, Jamaica [8].
Statistical Analysis
The statistical package which was used to analyze the collected data was SPSS and Microsoft excel. The data was initially stored in an excel database. The crude incidence rate (CIR) was also de-termined. It was calculated by dividing the total number of cases of cancer diagnosed in a specific population by the size of the popula¬tion and then multiplying the result by 100000 [1,2].
Results
Discussion
Table 1 shows the distribution based on age of persons diagnosed with cancer of the skin in 2008. When both genders were con¬sidered the highest frequencies occurred within the age group 45 years to 84 years. This was also apparent when the genders were considered separately. The table also shows that the risk of devel¬oping skin cancer increases with age, however after age 85 years the risk diminishes. Arnold et al. (2022), stated that the risk of developing melanoma increases with age and incidence is greater among older population [9]. Arnold et al. also provided data on the crude incidence rate of melanoma in different parts of the world in 2020. In the case of males it was 0.2 in Western Africa, 1.1 in the Caribbean, 33.8 in North America, 0.6 in China and 36.1 in Western Europe. In this present investigation the crude incidence rate (CIR) for melanoma in males in Jamaica 2008 was 2.6. Gib-son et al. (2010), obtained a CIR of 0.8 for melanoma in males [2]. They however only studied the population in Kingston and St. Andrew for the period 2003-2007. My results were align with those from Southern Africa which Arnold et al., provided. Arnold et al. (2022), also determined the CIR of melanoma in females in the year 2020 [9]. In the case of Western Africa it was 0.3, 0.8 for the Caribbean, 23.3 for North America, 0.5 for China and 30.5 for Western Europe. Based upon table 1 this present study obtained 2.5 for the CIR for melanoma in females. This aligned closely with Southern Africa as Arnold et al. (2022), obtained a CIR of 2.7 for melanoma in females in the year 2020. This present study showed that the mean age in which cancer of the skin developed was 60.8 years, which again confirms that the risk of developing skin cancer increases with age. Figure 2 shows the age distribution of mela¬noma in the year 2008 using a histogram. The normal curve high¬lighted that the data was negatively skewed.
Table 1: Frequency Table Showing Grouped Data of Persons Diagnosed with Cancer of the Skin in Jamaica 2008
|
Age/yr |
Frequency |
||
|
Both Genders |
Male |
Female |
|
|
0 – 4 |
0 |
0 |
0 |
|
5 – 9 |
0 |
0 |
0 |
|
10 – 14 |
0 |
0 |
0 |
|
15 – 19 |
0 |
0 |
0 |
|
20 – 24 |
1 |
1 |
0 |
|
25 – 29 |
2 |
0 |
2 |
|
30 – 34 |
2 |
0 |
2 |
|
35 – 39 |
1 |
0 |
1 |
|
40 – 44 |
2 |
1 |
1 |
|
45 – 49 |
8 |
2 |
6 |
|
50 – 54 |
12 |
8 |
4 |
|
55 – 59 |
5 |
3 |
2 |
|
60 – 64 |
6 |
3 |
3 |
|
65 – 69 |
6 |
4 |
2 |
|
70 – 74 |
8 |
4 |
4 |
|
75 – 79 |
6 |
4 |
2 |
|
80 – 84 |
7 |
4 |
3 |
|
85 – 89 |
2 |
1 |
1 |
|
90 – 94 |
0 |
0 |
0 |
|
95+ |
1 |
0 |
1 |
|
TOTAL (N) |
69 |
35 |
34 |
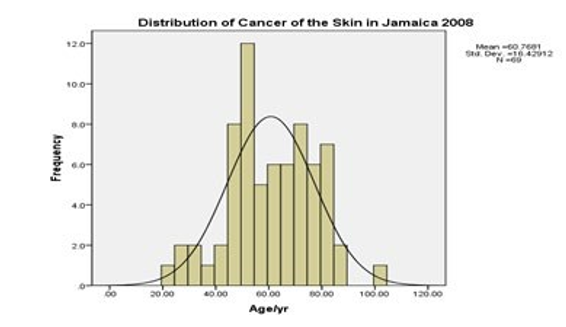
Figure 2: Histogram showing the Distribution of Cancer of the Skin in Jamaica 2008
The distribution of melanoma across all parishes was investigated by using the CIR. This is illustrated in table 2. Based upon the CIR the highest probability of developing cancer of the skin was in Kingston and St. Andrew (6.2), St. Mary (2.6), St. Ann (2.3), St. Catherine (2.1) and St. Thomas (2.1). Person would be less suscep¬tible in developing melanoma in other parishes. This highlights the importance of geographical location. The varying probability may be due to where persons of a lighter skin pigmentation reside. Ar- nold et al. (2022) stated that melanoma was largely concentrated in highly developed countries, predominantly inhabited by people of European origin [9]. Arnold et al. (2022), further stated that they would be more susceptible to the carcinogenic effects of solar ra¬diation. This therefore indicates that there may be persons of a par¬ticular genetic composition living in particular parishes. Gandini et al. (2005), declared that the risk of melanoma is also influenced by genetics [10].
Table 2: Comparing the Crude Incidence Rate of Cancer of the Skin for all Parishes in Jamaica 2008
|
Parish |
Cancer Cases |
Population Size |
Crude Incidence Rate |
|
Kingston and St. Andrew |
41 |
662426 |
6.2 |
|
St. Mary |
3 |
113615 |
2.6 |
|
St. Ann |
4 |
172362 |
2.3 |
|
St. Catherine |
11 |
516218 |
2.1 |
|
St. Thomas |
2 |
93902 |
2.1 |
|
St. Elizabeth |
2 |
150205 |
1.3 |
|
Clarendon |
3 |
245103 |
1.2 |
|
Portland |
1 |
81744 |
1.2 |
|
Westmoreland |
1 |
144103 |
0.7 |
|
St. James |
1 |
183811 |
0.5 |
|
Manchester |
0 |
189797 |
0 |
|
Trelawny |
0 |
75164 |
0 |
|
Hanover |
0 |
69533 |
0 |
In Table 3, when both genders were considered, the frequency of cancer of the urinary bladder (UBC) was high within the age group 60 years to 84 years. The mean age at which UBC was diagnosed in 2008 was 70.7 years. Richters et al. (2020), stated that in the United States of America, the majority of patients are diagnosed with UBC at 60 years and older [13]. In Jamaica 2008 the CIR of UBC in men was 2.8 while in the case of women it was 0.8 (male/ female ratio, 3.5). Hence men had more than three times the prob¬ability of developing UBC than women.
Table 3: Frequency Table Showing Grouped Data of Persons Diagnosed with Cancer of the Urinary Bladder in Jamaica 2008
|
Age/yr |
Frequency |
||
|
Both Genders |
Male |
Female |
|
|
0 – 4 |
0 |
0 |
0 |
|
5 – 9 |
0 |
0 |
0 |
|
10 – 14 |
0 |
0 |
0 |
|
15 – 19 |
0 |
0 |
0 |
|
20 – 24 |
0 |
0 |
0 |
|
25 – 29 |
0 |
0 |
0 |
|
30 – 34 |
0 |
0 |
0 |
|
35 – 39 |
0 |
0 |
0 |
|
40 – 44 |
1 |
1 |
0 |
|
45 – 49 |
3 |
3 |
0 |
|
50 – 54 |
2 |
2 |
0 |
|
55 – 59 |
1 |
1 |
0 |
|
60 – 64 |
6 |
5 |
1 |
|
65 – 69 |
6 |
5 |
1 |
|
70 – 74 |
10 |
5 |
5 |
|
75 – 79 |
6 |
5 |
1 |
|
80 – 84 |
9 |
7 |
2 |
|
85 – 89 |
4 |
3 |
1 |
|
90 – 94 |
0 |
0 |
0 |
|
95+ |
0 |
0 |
0 |
|
TOTAL (N) |
48 |
37 |
11 |
Gibson et al. (2010), determined the CIR by investigating UBC in Kingston and St. Andrew for the period 2003 – 2007 [2]. They obtained a CIR of 3.6 for males and 1.5 for females. Ferlay et al. (2018),stated that worldwide the lifetime risk of getting UBC is 1.1% in men and 0.27% in women (male/female ratio, 4.1) [11]. This comparison in probability aligns in a favourable manner with what was obtained when the CIR for UBC was determined in Ja- maica 2008. Noone et al. (2018), stated that UBC life-time risk in men and women in the United States of America were 3.9% and 1.2% respectively [12]. This probability ratio (male/female, 3.3) matches closely with the CIR ratio (male/female, 3.5) obtained in Jamaica 2008 for UBC where values of 2.8 and 0.8 were obtained for men and women respectively. The histogram, shown in figure 3 shows that the age distribution of UBC is negatively skewed.

Figure 3: Histogram showing the Distribution of Cancer of the Urinary Bladder in Jamaica 2008
Table 4 shows how UBC was distributed across all parishes in Ja-maica 2008. The CIR was used to obtain an objective comparison. The parishes in which an individual was most likely to develop UBC were Kingston and St. Andrew (3.3), St. Mary (2.6), St. Catherine (2.5), Portland (2.4) and St. Ann (1.7). In 2008 of the 48 persons diagnosed with UBC, 6 were smokers and only 1 was female. Richters et al. (2020), listed the following risk factors for developing UBC. These were cigarette smoking, chemical carcin¬ogens in certain occupations, arsenic in drinking water and endem¬ic chronic urinary infections caused by Schistosoma haematobium [13]. Richters et al. (2020) stated that cigarette smoking is by far the number one risk factor. Ferris et al. (2013) stated that frequent and prolonged use of hair dyes increases the risk of UBC [14]. Fer¬ris et al. (2013) also stated that patients treated with cyclophospha-mide, ifosfamide and ionizing radiation have an increased risk of developing UBC. Risk have also been associated with high intakes of meat, especially red meat, animal fats, cholesterol, fish, animal food cooked at high temperatures, smoked and salted [15-17]. Sci¬entific evidence has shown that high consumption of fruits and vegetables have protective effects [17,18]. Richters et al. (2020), declared that UBC has the highest life-time treatment costs per patient of all cancers.
Table 4: Comparing the Crude Incidence Rate of Cancer of the Urinary Bladder for all Parishes in Jamaica 2008
|
Parish |
Cancer Cases |
Population Size |
Crude Incidence Rate |
|
Kingston and St. Andrew |
22 |
662426 |
3.3 |
|
St. Mary |
3 |
113615 |
2.6 |
|
St. Catherine |
13 |
516218 |
2.5 |
|
Portland |
2 |
81744 |
2.4 |
|
St. Ann |
3 |
172362 |
1.7 |
|
Clarendon |
3 |
245103 |
1.2 |
|
St. Elizabeth |
1 |
150205 |
0.7 |
|
Manchester |
1 |
189797 |
0.5 |
|
St. Thomas |
0 |
93902 |
0 |
|
Westmoreland |
0 |
144103 |
0 |
|
St. James |
0 |
183811 |
0 |
|
Hanover |
0 |
69533 |
0 |
|
Trelawny |
0 |
75164 |
0 |
Limitations
Limitations In 2008 and earlier there were two major cancer treatment centres in Jamaica for the public. These were Kingston Public hospital in Kingston and Cornwall Regional hospital in St. James. The ma¬chines they had at that time were cobalt machines. Hence many cases would be referred to Kingston Public hospital from other parishes or to Cornwall Regional hospital. This would depend on the proximity and the accessibility, meaning the length of the wait¬ing list. Staff at the Jamaica Cancer Registry only gets data from hospitals and private sources in Kingston and St. Andrew Jamaica. Hence some patients from the western end of the island such as the parishes of St. James, Westmoreland, Trelawny and Hanover would not be recorded based upon the present practise. Hence these would contribute to errors in the data from parishes in those regions of the island. In Kingston at that period there was the Radi¬ation Oncology Centre of Jamaica which was established in 2001. This is a private centre for the treatment of cancer. Hence the lim¬itation here would be your socioeconomic status. There would also be persons who would seek alternative ways to treat their cancer.
Conclusion
This present study further confirms that melanoma and UBC are cancers which are more pervasive in the population as individuals get older. This study also reveals the importance of geographical location since persons are more prone to developing these cancers in certain regions. It is therefore important that health adminis¬trators promote primary health care to mitigate against the finan¬cial burden associated with these cancers. Genetic predisposition should always be considered when developing any such primary health care plan.
Data Availability Statement
The data used were not available online and permission granted is in the document attached.
Ethical Approval
Ethical approval was not requested because data was treated anon¬ymously.
Acknowledgement
I wish to thank Professor Mitko Voutchkov for his continued guid-ance. I also wish to express posthumous thanks to Professor Barrie Hanchard who provided insightful suggestions and access to the Jamaica Cancer Registry located in the Pathology Department of the University of the West Indies.
Synopsis
This study investigated the distribution of cancer of the skin and cancer of the urinary bladder in Jamaica 2008.
References
- Gibson, T. N., Blake, G., Hanchard, B., Waugh, N., & Mc-Naughton, D. (2008). Age-specific incidence of cancer in Kingston and St Andrew, Jamaica, 1998–2002. West Indian Med J, 57(2), 81-89.
- Gibson, T. N., Hanchard, B., Waugh, N., & McNaughton, D. (2010). Age-Specific Incidence of Cancer in Kingston and St Andrew, Jamaica, 2003-2007. West Indian Medical Journal, 59(5), 456 - 64.
- https://maps-jamaica.com/map-of-jamaica-parishes-and-cap-itals
- Bras, G. (1966). Cancer incidence in Jamaica, Kingston and St Andrew 1958–1963. Cancer incidence in five continents, 1, 84-9.
- Brooks, S. E., & Wolff, C. (1991). Age-specific incidence of cancer in Kingston and St. Andrew, Jamaica. Part I: 1978-1982. The West Indian Medical Journal, 40(3), 127-128.
- Jensen, O. M. (Ed.). (1991). Cancer registration: principles and methods (Vol. 95). IARC.
- World Health Organization. (2004). International Statistical Classification of Diseases and related health problems: Alphabetical index (Vol. 3). World Health Organization.
- http://statinja.gov.jm/Census/PopCensus/Populationbyfive-yearsagegroup.aspx
- Arnold, M., Singh, D., Laversanne, M., Vignat, J., Vaccarella, S., Meheus, F., ... & Bray, F. (2022). Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA dermatology, 158(5), 495-503.
- Gandini, S., Sera, F., Cattaruzza, M. S., Pasquini, P., Zanet-ti, R., Masini, C., ... & Melchi, C. F. (2005). Meta-analysis of risk factors for cutaneous melanoma: III. Family history, actinic damage and phenotypic factors. European journal of cancer, 41(14), 2040-2059.
- Ferlay, J., Ervik, M., Lam, F., Colombet, M., Mery, L., Piñeros, M., ... & Bray, F. (2018). Global cancer observatory: cancer today. Lyon, France: international agency for research on cancer, 3(20), 2019.
- Noone, A. M., Howlader, N., Krapcho, M. A., Miller, D.,Brest, A., Yu, M., ... & Cronin, K. A. (2018). SEER Can-cer Statistics Review, 1975-2015, National Cancer Institute. Bethesda, MD.
- Richters, A., Aben, K. K., & Kiemeney, L. A. (2020). The global burden of urinary bladder cancer: an update. World journal of urology, 38, 1895-1904.
- Ferrís, J., Berbel, O., Alonso-López, J., Garcia, J., & Ortega, JA (2013). Environmental non-occupational risk factors associated with bladder cancer. Actas Urológicas Españolas (English Edition) , 37 (9), 579-586.
- Silverman DT, Devesa SS, Moore LE, Rothman N. Bladder Cancer. In: Schottenfeld D, Fraumeni J, editors Cancer epidemiology and prevention. 3rd.New York: Oxford University Press: 2006. P. 1101 – 1127.
- Kogevinas M, Garcia-Closas M, Trichopoulos D. Urinary bladder cancer In: Adami HO, Hunter D, Trichopoulos D. editors. Textbook of cancer epidemiology. 2nd. New York: Oxford University Press: 2008. p. 573 – 596.
- Silberstein, J. L., & Parsons, J. K. (2010). Evidence-based principles of bladder cancer and diet. Urology, 75(2), 340-346.
- Brinkman, M. T., Buntinx, F., Kellen, E., Dagnelie, P. C., Van Dongen, M. C., Muls, E., & Zeegers, M. P. (2011). Dietary intake of micronutrients and the risk of developing bladder cancer: results from the Belgian case–control study on bladder cancer risk. Cancer Causes & Control, 22, 469-478.