
International Internal Medicine Journal(IIMJ)
ISSN: 2837-4835 | DOI: 10.33140/IIMJ
Impact Factor: 1.02



Research Article - (2024) Volume 2, Issue 2
Dietary Practice and Associated Factors Among Type 2 Diabetic Patients on Follow-Up in Shashemene Referral Hospital, West Arsi Zone, Oromia, Ethopia, 2020
2School of public health Shashemene campus of Madda Walabu University, west Arsi zone ,Oromia, Ethiopia
3School of Nursing Goba campus of Madda Walabu University, Ethiopia
Received Date: Jan 24, 2024 / Accepted Date: Feb 15, 2024 / Published Date: Feb 28, 2024
Copyright: ©Â©2024 Kelemua lemma, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Lemma, K., Kumsa, K., Assefa, T. (2024). Dietary Practice and Associated Factors Among Type 2 Diabetic Patients on Follow-Up in Shashemene Referral Hospital, West Arsi Zone, Oromia, Ethiopia, 2020. Int Internal Med J, 2(2),01-10.
Abstract
Background: Diabetes' diet is a naturally nutrient-rich, fat-free and calorie-free diet. Dietary factors play a critical role in the management and prevention of type 2 diabetes due to their impact on weight and metabolic control.
Objective: The goal of this study was to evaluate dietary practices and associated factors among type 2 diabetic patients on follow-up at Shashemene referral hospital in West Arsi zone, Oromia, Ethiopia, in 2020.
Methods: In April 2020, a hospital-based cross-sectional study of type II diabetic patients on follow-up was conducted at Shashemene referral hospital. A sample size of 389 was used based on the prevalence of dietary practice among type II diabetic patients. Pre-test, structured face-to-face interview questionnaires were used to collect data from systematically selected samples of type II diabetic patients. Data was entered into a computer using the statistical analysis software SPSS version 25.0. Descriptive analysis was used to present the findings. Bivariate and multivariate logistic regression were used to further analyze the data. The odds ratio with a 95% confidence interval.
Result: A total of 389 patients with type II diabetes were included in the study whose mean age and standard deviation (SD) was 42+ 12.2 SD. The study revealed that 39.3% of the patients had good dietary practice. Factors significantly associated with dietary practice were patient religion (AOR=10.32 ,95% CI (1.25,85.2), having family support, (AOR=4.10 95% CI (2.05,8.18) awareness level about diet (AOR = 3.8, 95% CI (0.34,5.94) and high cost of food (AOR = 2.06 95% CI (1.08,3.89) were found independent predictors for good dietary practice.
Conclusion & Recommendations: The dietary practices of diabetic patients are not enough and they need to be improved. Training and advice on components of the proposed nutritional diabetes must be provided. The quality and scope of health education at the hospital level can be improved and the lifestyle changed. This level of self-care should be achieved through collaboration between patients and health care providers.
Keywords
Diabetes Mellitus, Dietary Practice, Associated Factor.
Introduction
Background
Diabetes is a condition in which your blood glucose, often known as blood sugar, is abnormally high. Your main source of energy is blood glucose, which comes from the food you eat. Type I diabetes occurs when the pancreas' insulin-producing cells (beta cells) are destroyed, while type II diabetes (adult- onset diabetes) happens when the pancreas produces insulin but it is insufficient or does not operate effectively. Diabetes mellitus is a serious, long term condition with a major impact on the lives and well-being of individuals ,families and societies and caused by multiple etiologies characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both [1]. Diabetes has progressively become a public health problem worldwide. In 2000, the global estimate of diabetes prevalence in the age 20–79-year age group is 151 million, alarming increases tripling to continue now a days, more than 463 million people are living with diabetes in 2019 and predicted to increase to 700 million by 2045 [2]. In Africa, particularly in urban areas intake of unhealthy diets that are richer in high -fat, high energy foods contribute directly to increased energy imbalances, and obesity and diabetes [3]. Diabetes is a complex, chronic illness requiring continuous self-care and medical care with multifactorial risk- reduction strategies beyond glycemic control [4].
The main causes of the fast-rising incidence of diabetes in emerging countries are poor dietary habits and a sedentary lifestyle. In addition to any pharmacological treatment, good eating habits are a crucial gold standard metric for managing type 2 diabetes mellitus [5]. Nutrition therapy aims to preserve or improve one's quality of life while also preventing and treating diabetes's acute and long-term consequences [6]. Unhealthy diet is one of the top risk factors for the global burden of disease such as diabetes ,heart disease, stroke and cancer [7]. In Ethiopia, the scarcity of health information and standard guideline related to diet has been posing catastrophes on long-term glycemic control in diabetes patients. At the same time, care givers often give less attention to describe dietary practice [8]. The purpose of this study is to evaluate dietary practices and associated factors in type 2 diabetic patients who are being followed up on at Shashemene referral hospital(Figure 1).
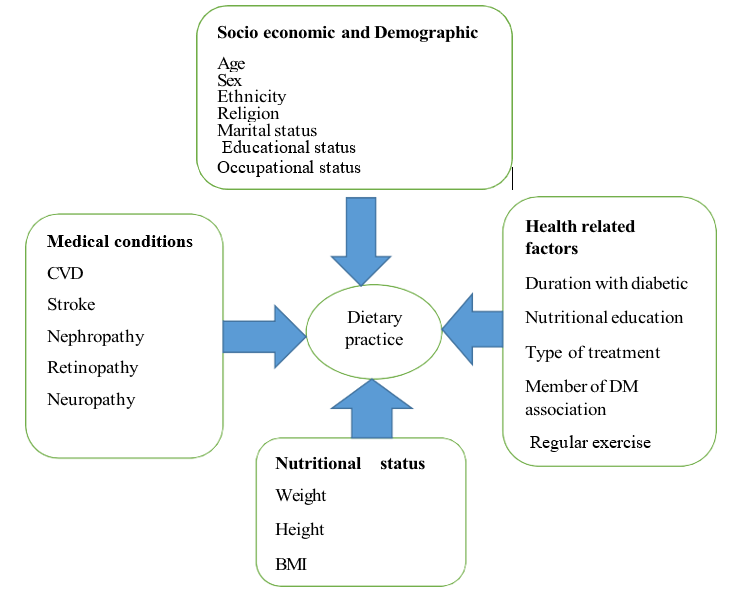
Figure 1: Conceptual Frame Work Showing Dietary Practice and Associated Factors of Type II Diabetic Patient on Follow up at Shashemene Referral Hospital West Arsi, Zone, Oromia Ethiopia,2020. Adapted by Reviewing Different Literatures (Mulugeta .Y et al ,2018, Worku. H et al ,2015.
Material and Method
Study Settings and Period
The study was conducted in Shashemene referral hospital. Shashemene referral hospital is situated in West Arsi zone, Oromia region, Southeast, Ethiopia. Shashemene town is 250km far from Addis Ababa. Shashemene referral hospital is situated on Ethio-Kenya main road, 7 km to the north of Shashemene town in specific place known as kuyera. The Hospital has 232 beds and 325 technical and administrative staffs. The outpatient department for chronic illness follow-up and diabetic treatment has been providing treatment 2 days a week. Report of Shashemene referral hospital showed that there is a total of, 3264 type II diabetic patient attending the hospital follow-up clinic. The study was conducted from April 1 to 30, 2020 at Shashemene referral hospital diabetic follow-up clinic. The aim of selecting Shashemene referral hospital among those West Arsi zone public hospitals is the hospital well experienced and high client number on flow -up care than others hospitals.
Study Design
Hospital –based cross-sectional study was conducted at Shashemene referral hospital chronic follow -up clinic
Source Population
All type II diabetic patient who attended their follow up at Shashemene referral hospital chronic follow -up care clinic in 2020. 2.3 Study Population Randomly selected type II DM patients who had follow-up visit in the diabetes referral clinic during the study period were the study population in 2020.
Sample Size Determination
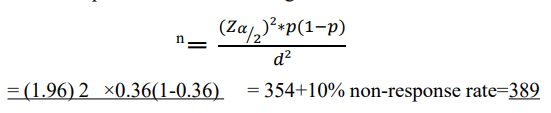
The sample size was calculated using the single population proportion formula with the following assumptions in mind. The proportion of type II diabetic patients who follow a healthy diet (36%) , 5 95 percent confidence level, 5% margin of error, and 10% non-response rate [5].
Sample Size for the First Objective
Total Sample size calculated using the formula indicated as:
Where:
n is implying the final sample size
Zα⁄2= 95%confidence level which is 1.96
P = proportion of good dietary practice of type II diabetic patient = 0.36
d = margin of error(d)5% by adding 10% none response rate then the final sample size was 389 type II DM patients.
Sampling Procedure
In Shashemene referral follow-up clinic there are 3,264 registered diabetic patients under follow up care. Every patient had follow- up at list every 3 month. Systematic sampling technique was used to select the study participants. The K-value (the interval) was calculated by dividing total number of type II DM patients (1088) who have appointment during the study period from diabetes referral clinic registration log book to the calculate sample size. Accordingly, every 3 patients were selected, with the first sample chosen by lottery method (Figure 2). K is calculated as K =N/n , 3264÷ Q3month follow up =1088 monthly follow up 1088÷389 =2.7(3).
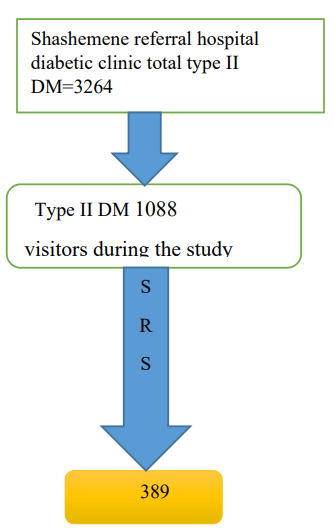
Figure 2: Schematic Presentation of Showing the Procedure Used to Select Type II Diabetic Patient from Shashemene Referral Hospital 2020
Operational Definitions
Dietary Practice refers to patients' choices in food consumption based on diabetes nutrition education that gives emphasis to intake of food with lower fat, higher fiber, and lower sodium [9].
• Good Dietary Practice: Study participants who scored above median value for response yes were classified as having good dietary practice from the listed 15 dietary practice measuring questions.
• Poor Dietary Practice: Study participants who scored below median value for response yes were classified as having poor dietary practice from the listed 15 dietary practice measuring questions.
Inclusion and Exclusion Criteria
All adult type II diabetic patients who were on regular follow-up and aged ≥ 18 years were included in the study. Those adult type II DM patients who are critically ill, have severe mental illness and patients who are unable to communicate were excluded from the study.
Independent and Dependent Variables
Socio demographic characteristics (age, sex, marital status, monthly income, Educational status, Family support, Occupational status,), Nutritional status (weight in kg, height in meter, BMI) Medical conditions: HPN, CVD, Stroke, Amputation, Nephropathy, Retinopathy. Health related factors: Duration Diabetic, Nutritional education, type of treatment, member of DM association, Regular exercise, Nutritional knowledge, and FBS Level.
Data processing and analysis
Data was coded and entered in to the statistical software SPSS version 25 for data entry and analysis. The entered data was then checked for outliers, missing values, and cleaned before being analyzed. To summarize data, descriptive statistics such as frequency and cross tabulation were used. A binary logistic regression analysis was performed to examine the relationship between the independent variables and the outcome variable. The variables with p0.25 in the binary logistic regression analysis were entered into the multiple logistic regressions model to control the effect of confounders based on the results of the binary logistic regression analysis. The statistical association was assured or tested with 95 percent confidence interval and P-value <0.05 through odds ratio. In order to examine the statistical link between the independent result and selection of variables, a multivariate analysis was used. Tables, figures and texts were presented with the results. Finally, the p-value variables < 0.05 were considered statistically important in multivariate analysis.
Ethical Considerations
Ethical clearance was secured from the ethical review board of Madda Walabu University Ref.01/2/11497. Then, ethical clearance letter was submitted to the public hospital to obtain permission from respective health facility. Finally, verbal consent was taken from the study participants. In addition, to assure the privacy and confidentiality of the information participants name or address was not recorded.
Results
Socio Demographic Characteristics of Study Subjects.
The study was completed by a total of 389 participants in a 100% Type II diabetic survey. Participants had a mean age of 42±12,2 SD years and were between 31 and 40. Almost half of the female population was 213 (54.8 percent). The majority of those interviewed 305(78.4%) were married and 217(55.8%) were Muslim religious followers. Of the total of interviewees, 339(87.1%) were urban residents and 217(55.8%) were ethnically Oromo ,(Table 1).
|
Variable |
Frequency |
% |
|
Age |
||
|
20-30 |
76 |
19.5 |
|
31-40 |
126 |
32.4 |
|
41-50 |
106 |
27.2 |
|
>50 |
81 |
20.8 |
|
Mean age |
42.2(SD+12.2) years |
|
|
Sex of the patient |
||
|
Male |
176 |
45.2 |
|
Female |
213 |
54.8 |
|
Religion |
||
|
Orthodox |
134 |
34.4 |
|
Muslim |
172 |
44.2 |
|
Catholic |
13 |
3.3 |
|
Protestant |
70 |
18 |
|
Ethnicity |
||
|
Amhara |
50 |
12.9 |
|
Oromo |
217 |
55.8 |
|
Tigre |
21 |
5.4 |
|
Wolita |
80 |
20.6 |
|
Silxe |
5 |
1.3 |
|
Kembata |
16 |
4.1 |
|
Occupational status |
||
|
House wife |
77 |
19.8 |
|
Farmer |
21 |
8 |
|
Retired |
27 |
6.9 |
|
Government employee |
112 |
28.9 |
|
Student |
22 |
5.7 |
|
Marchant |
96 |
24.7 |
|
Daily laborer |
24 |
6.2 |
|
Educational status |
||
|
Illiterate |
71 |
18.3 |
|
Read and write |
109 |
28.0 |
|
Primary school |
8 |
2.1 |
|
Secondary school |
96 |
24.7 |
|
College and above |
105 |
27.0 |
|
Marital statues |
||
|
Single |
71 |
18.3 |
|
Married |
305 |
78.4 |
|
Widowed |
5 |
1.3 |
|
Divorced |
8 |
2.1 |
|
Family size |
||
|
<5 family size |
271 |
69.7 |
|
>5 family size |
118 |
30.3 |
|
Place of residence |
||
|
Urban |
339 |
87.1 |
|
Rural |
50 |
12.9 |
|
Monthly income |
||
|
1000-2000 |
252 |
64.8 |
|
3000-4000 |
100 |
25.7 |
|
>5000 |
37 |
6.5 |
Table 1. Socio demographic characteristics of respondents, shashemene Shashemene referral hospital, west Arsi zone,Oromia, Ethiopia, 2020. (N=389)
Health and Nutritional Status History
The majority of the study participants had a follow-up duration of 244 (62.7%) over a period of five years. Half of the year, 201 (51.7%) of participants have hypertension, with 124 co-morbidities (31.6 percent). There are also 287 (59.9%) responders who have no DM family history. 260 (66.8%) of the 260 patients diagnosed with diabetes did not change their eating habits. Doctors have given nutritional recommendations to the vast majority of the patients in this study 332. (84. 7 percent). However, the nurse had only given dietary guidance to a few patients 42 (10.7 percent).
The expense of healthy goods (173 (44.5%) was the leading reason for not implementing diabetic dietary habits, followed by a lack of dietary knowledge154 (39.6 percent). 273 (70.2%) of the total respondents did not participate in regular exercise, 339 (87.1%) of the participants had FBS >126mgdl, and 244 (62.7%) of the participants were overweight( Table 2).
|
Variables |
frequency |
% |
|
How long diagnosed with DM |
||
|
1-5 years |
244 |
62.7 |
|
6-10 |
119 |
30.6 |
|
>10 years |
26 |
6.7 |
|
Duration on DM follow up |
||
|
1-5 |
248 |
63.7 |
|
6-10 |
115 |
29.6 |
|
>10 |
26 |
6.7 |
|
Having complications? |
||
|
Yes |
201 |
51.7 |
|
No |
188 |
48.3 |
|
If yes what type of comorbidity |
||
|
HPN |
124 |
31.6 |
|
Nephropathy |
37 |
9.4 |
|
CVD |
6 |
1.5 |
|
Neuropathy |
9 |
2.3 |
|
Retinopathy |
25 |
6.4 |
|
Do you have family history of DM? |
||
|
Yes |
102 |
41.1 |
|
No |
287 |
59.9 |
|
By what do you control your DM? |
||
|
Insulin |
160 |
41.1 |
|
Tablet |
229 |
59.9 |
|
Have you made a complete change of your dietary habit after you know you are diabetic? |
||
|
Yes |
129 |
33.2 |
|
No |
260 |
66.8 |
|
source of information about diabetic diet? |
||
|
TV/radio |
11 |
2.8 |
|
Doctors |
332 |
84.7 |
|
Nurses |
42 |
10.7 |
|
Diabetic patient |
4 |
1.0 |
|
Does doctors give advice about diabetic patient diet? |
||
|
Yes |
149 |
38.3 |
|
No |
240 |
61.7 |
|
What does your doctor give dietary advice recommend that you should be eating more? |
||
|
To eat the whole grain |
9 |
2.3 |
|
To eat more vegetable |
33 |
8.5 |
|
To avoid sweets |
95 |
24.4 |
|
Reduce salt |
12 |
3.1 |
|
Have you Participated in regular exercise |
||
|
Yes |
116 |
29.8 |
|
No |
273 |
70.2 |
|
If yes mention type of exercise |
||
|
Regular walking |
76 |
58.5 |
|
Regular running |
40 |
41.5 |
|
Factors affect your dietary habit |
||
|
Cost of healthy foods |
173 |
44.5 |
|
unavailability of fruit and vegetables |
4 |
1.0 |
|
Poor dietary knowledge |
154 |
39.6 |
|
Cost of heathy food unavailability of food |
40 |
10.3 |
|
Others |
18 |
4.6 |
|
Are you a member of diabetic associations? |
||
|
Yes |
14 |
3.6 |
|
No |
375 |
96.4 |
|
Fast blood glucose level |
||
|
>126 |
339 |
87.1 |
|
<126 |
50 |
12.9 |
|
BMI |
||
|
18.5-24.9kgm2 |
133 |
34.2 |
|
25-29.9kgm2 |
244 |
62.7 |
|
>30kgm2 |
12 |
3.1 |
Tabel 2: Health and nutritional related characteristics of type II diabetes patients in Shashemene referral hospital, West Arsi Zone, Oromia, Ethiopia, 2020
Dietary Practice of Type II DM Patient
In this study 39.3% of type II DM patients had good dietary practice whereas 60.7% respondents’ poor dietary practice. Most of 258 (66.3%) type II diabetic respondents were not plan their meal based on 311(79.9%) and 238(61.8%) recommended diabetic diet and not follow always regular meal time respectively (Figure 3).
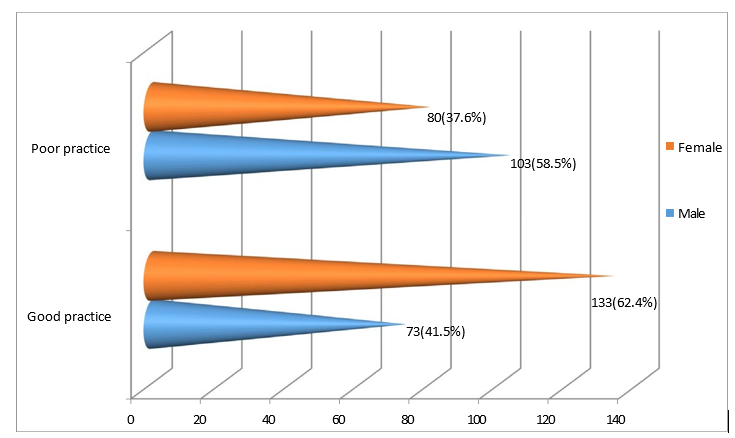
Figure 3: Dietary Practice of Type II DM Patients Classified by Sex Category in Shashemene Referral Hospital, West Arsizone, Ethiopia, 2020.
Factors Associated with Dietary Practice of Type II Diabetic Patients
In this study, the factors associated with dietary practice of type II diabetic patients were identified as having family support has217(55.8 percent) and not having access to fruit has the highest frequency rate of no response 285 (73 percent ) (Figure 4) .
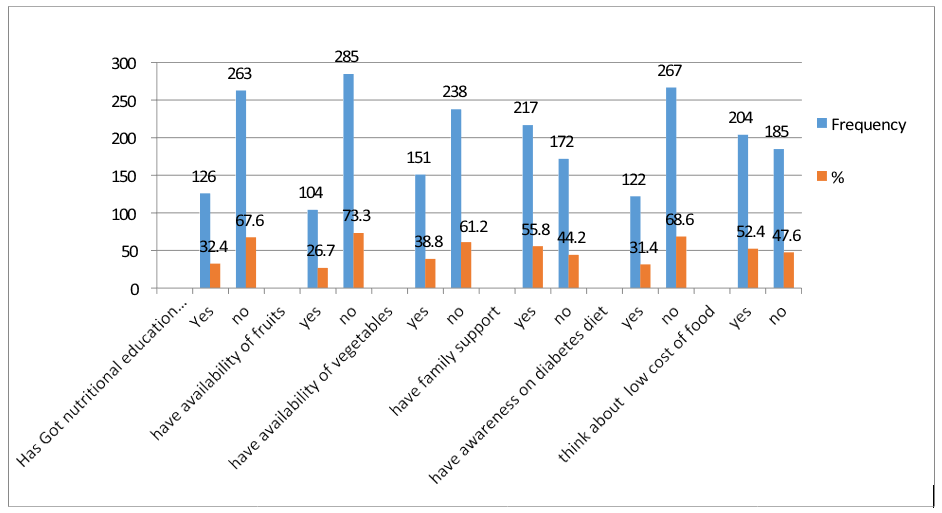
Figure 4: Dietary Practice Related Variables of type II Diabetic Patients on Follow Up in Shashemene Referral Hospital West Arsi zone, Ethiopia, 2020
Factors Associated with Dietary Practice of Type II Diabetic Patients at Shashemene Referral Hospital, West Arsi zone, Ethiopia, 2020.
The factors associated with type II diabetic patients were identified using binary and multivariable logistic regression. Using binary logistic regression, the first sixteen factors were examined. Catholic religion (COR=8.30,95 percent CI=(1.77,8.29), no family history of diabetes (COR=5.21,95 percent CI=(3.27,38.9), and not receiving nutrition education on diabetes diet (COR=5.32,95 percent CI=(3.27,38.9) were among these (3.36,8.41), unavailability of vegetables COR=3.54 (2.30,95% CI=(2.30,5.44), not having family support COR=5.21,95% CI=(3.27,8.28).
not having awareness on diabetes diet COR=9.10,95% CI=(5.56,14.9) and thinking about high cost of food COR=4.74,95% CI=(3.02,7.26) had p value < 0.25 and were found selected for multivariate logistic analysis. Among these, eight predictors were found significantly associated with dietary practice of type II diabetic patients.
A significant association was found in multivariate logistic regression analysis between patients' dietary practices and religion, not having a family history of diabetes, not receiving nutrition education in the hospital, not having family support, and thinking about high-cost food (p-value 0.05). There was no significant relationship between diabetic patients' dietary practices and their age, gender, marital status, educational status, ethnicity, or place of residence (p-value > 0.05) (Table 3).
|
Variable |
Dietary practice of type II DM patient |
COR (95%CI) |
AOR (95%CI) |
p-value |
|
|
Good |
Poor |
||||
|
Age of the patient |
|||||
|
20-30 |
30(39.5%) |
46(60.5%) |
0.77(0.41, 1.46) |
0.67(0.31,0.53) |
|
|
31-40 |
45(35.7) |
81(64.3) |
0.66(0.37, 1.16) |
1.28(0.53,3.10) |
|
|
41-50 |
41(38.7) |
65(61.3) |
0.75(0.41, 1.34) |
1.94(0.67,5.57) |
|
|
>50 |
44(54.3) |
37(45.7) |
1 |
1 |
|
|
Religion Of the patient |
|||||
|
Orthodox |
53(39.8%) |
80(60.2%) |
1 |
1 |
|
|
Muslim |
66(38.4%) |
106(61.6%) |
0.94(0.59,1.49) |
0.94(0.59,1.49) |
|
|
Catholic |
11(84.6%) |
2(15.4%) |
8.30(1.77,38.9) * |
8.28(1.70,40.35) * |
0.009 |
|
Protestant |
23(32.4%) |
48(67.6%) |
0.72(0.39,1.33) |
0.72(0.36,1.43) |
|
|
Family history of DM |
|||||
|
Yes |
75(74.3%) |
26(25.7%) |
1 |
1 |
|
|
No |
78(27.1%) |
210(72.9%) |
5.21(3.27,8.29) * |
4.10(2.05,8.18) ** |
0.000 |
|
FBS |
|||||
|
<126 |
10(20%) |
40(80%) |
1 |
1 |
|
|
>126 |
143(42.2%) |
196(57.8%) |
2.91(1.41,6.03) * |
0.39(0.15,0.98) |
0.045 |
|
Do you get nutrition education at hospital |
|||||
|
Yes |
83(65.9%) |
43(34.1%) |
1 |
1 |
|
|
No |
70(26.6%) |
193(73.4%) |
5.32(3.36,8.41) * |
0.45(0.23,0.88) * |
0.021 |
|
Do you have availability of fruit |
|||||
|
Yes |
67(64.4%) |
37(35.6%) |
1 |
1 |
|
|
No |
86(30.2%) |
199(69.8%) |
4.19(2.60,6.73) * |
1.19(0.55,2.56) |
|
|
Do you have availability of vegetable |
|||||
|
Yes |
87(57.6%) |
64(42.4% |
1 |
1 |
|
|
No |
66(27.7%) |
172(72.3%) |
3.54(2.30,5.44) * |
1.39(0.73,2.62) |
|
|
Have family support |
|||||
|
Yes |
120(55.3%) |
97(44.7%) |
1 |
1 |
|
|
No |
33(19.2%) |
139(80.8%) |
5.21(3.27,8.29) * |
3.78(2.07,6.89) ** |
0.000 |
|
Awareness on diabetes diet |
|||||
|
Yes |
90(73.8%) |
32(26.2%) |
1 |
1 |
|
|
No |
60(23.6%) |
204(76.4%) |
0.11(0.067,0.18) |
0.15(0.09,0.26) ** |
0.000 |
|
Think about high cost of food |
|||||
|
Yes |
114(55.9%) |
90(40.1%) |
1 |
1 |
|
|
No |
39(21.1%) |
146(78.9%) |
4.74(3.028,7.26) * |
2.06(1.08,3.89) * |
0.027 |
Table 3: Bivariate and Multivariate logistic regression done for factors associated with dietary practice of type II diabetes patient on follow up at Shashemene referral Hospital, West Arsi zone, Oromia, Ethiopia, 2020
Discussion
The goal of this study was to evaluate the dietary habits of type II diabetic patients on the recommended diet who were being followed up on at Shashemene referral hospital. Diabetic patients' poor dietary habits have a significant impact on their health. Similarly, a good nutritional status on a diabetic diet is recommended for maintaining health and preventing complications. Dietary practices of type II diabetes patients are regarded as a key indicator in assessing individuals' access, utilization, and diet quality. According to this study, 39.3 percent of type II diabetic patients follow a healthy diet. According to the findings of this study, a large proportion of type II diabetic patients had insufficient dietary practice (60.7 percent). The result was lower than the 62.8 percent found in a Botswana study [10]. This finding, however, was higher than the 19 percent found in a study conducted at Pakistan University of Lahore [11]. This finding was also slightly higher than the 35.9 percent found in a study conducted in Bahir Dar Felege Hiwot hospital in North West Ethiopia [5]. While it was lower than the 48.6 percent reported in a study conducted in Yekatit 12 hospital in Addis Abeba, Ethiopia.12 The difference could be due to differences in geographical area, economic status, nutrition awareness level and specific culture of a community, an individual's dietary preference, and seasonal variation in food production and consumption.
According to this study, the patient's religion, family history of diabetes, nutrition education at the hospital, family support, high food costs, and FBS level were all significantly associated with dietary practice.
In the current study, there was a statistically significant positive association between type II diabetic patients who did not receive health education about diabetic diet at the hospital level being 55% (AOR: 0.45 CI (0.23,0.88) less likely to practice good dietary practice when compared to those who had received nutrition education in the hospital. This result was lower than that of a previous study in Addis Abeba, Ethiopia (AOR= 4.47 CI) (1.92,10.40).Exposure to information obtained from health professionals and other people may result in changes in eating behavior, which could explain the disparity.
There were also other linked factors: respondents without a family history of diabetes were 4 times more likely to have good dietary practices than those with a family history (AOR =4.10, 95 percent CI) than those with a family history (AOR =4.10, 95 percent CI) than those with a family history (AOR =4.10, 95 percent CI) than those with a family history (AOR =4.10, 95 percent CI) than those with a family history (AOR = (2.05,8.18). A clinically significant finding, on the other hand, does not automatically imply a statistically significant finding. Because research shows that cultural, social, economic, and environmental factors influence food preferences, the disparity could also be related to socioeconomic and cultural differences, literacy levels, and the quality of service received. According to this study, respondents who had family participation or support for type 2 diabetic treatment were 4 times more likely to have good dietary practices than those who did not (AOR =3.8, 95 percent CI (2.05,8.18). This finding was statistically different from that of a study conducted at Bhair Dar Felege Hiwot Hospital (AOR = 2.6, 95 percent CI (1.6, 4.2) [5].
This study found that overall diabetes diet awareness was an important predictor of good dietary practice. Respondents with good dietary practice awareness were 84 percent less likely to have good dietary practice than respondents with no awareness of diabetic diet (AOR = 0.159, 95 percent CI, 0.15(0.09, 0.26)). This finding is consistent with studies conducted in Bahir dar felege hiwot hospital, Ethiopia (AOR = 2.6, 95 percent CI (1.5, 4.6)) [5]. The overall level of diabetes diet awareness was found to be an important predictor of good dietary practice in this study. Respondents with good dietary practice awareness were 84 percent less likely to have good dietary practice than respondents with no awareness of diabetic diet (AOR = 0.159, 95 percent CI, 0.15(0.09,0.26)). This finding is consistent with studies conducted in Bahir dar felege hiwot hospital, Ethiopia (AOR = 2.6, 95 percent CI (1.5, 4.6)) [5]. One possible explanation is that they could receive nutrition counseling and better information from their providers. When people are aware of the benefits of a diabetes diet plan, they stick to the newly promoted diet. The study also discovered that factors associated with type II DM patients who did not consider high food costs were two times more likely to have good dietary practices than those who did consider high food costs (AOR = 2.06, 95 percent CI) (1.08,3.89).
This finding was consistent with the findings of a study conducted at Yekatit 12 Hospital in Addis Ababa, Ethiopia (AOR = 2.3, 95 percent CI (1.18, 4.70)) [12]. This could be explained by respondents' economic status, culture, social status, or service quality. A low income can make it difficult to obtain the foods necessary for a healthy diet and nutritional status. Inability to pay for food and other aspects of diabetes care can be an impediment to optimal dietary practice.
Personal perception and culture of patients may influence diabetes self-management. A significant proportion of diabetes patients did not follow dietary recommendations.
This could be due to the fact that having a good dietary practice to understand the benefit for type II diabetic patient prevention and management.
Conclusion
The findings of this study indicate that type II diabetic patients' dietary practices regarding the recommended diabetes diet were insufficient. More than half of the patients had poor dietary practices, which may indicate that poor practices, not attending diabetic nutrition education, not having family support, thinking about high-cost foods, and having a higher level of FBS need to be improved. Furthermore, this study found that type II diabetic patients were not following good dietary practices at the hospital level. Diabetes is a difficult disease to manage, and patients must participate actively in their own care. This can be accomplished by improving the quality and scope of health care.
Declarations
Ethics Approval and Consent to Participate
• Ethical approval was received from institutional review board of Madda walabu University college of health science.
• Methods were carried out in accordance with relevant guidelines and regulations.
• Informed consent was obtained from all subjects. Informed consent has been obtained from the participants, their parents and legally authorized representatives in this study
Consent for Publication
Consent was taken from the patient verbally before data collection. Informed consent has been obtained from the participants, their parents and legally authorized representatives in this study.
Availability of Data and Material
All the data were included in the manuscript and the SPSS data is also uploaded in the supplementary material
Competing Interests
No conflicts of interest prevail among researchers.
Funding
No fund
Author Contributions
Formal analysis:Kelemua lemma,kebede kumsa.
Investigation: Kelemua lemma.
Methodology: Kelemua lemma, kebede Kumsa.
Supervision: Kelemua lemma.
Writing : Original draft: kelemua lemma
Acknowledgements
First and foremost, we would like to express our gratitude to Madda Walabu University, Bale Goba Campus, for allowing us to conduct this research project aimed at determining to assess the dietary practices of type 2 diabetic patients.
Finally, we would like to thank the data collectors and study participants for their assistance throughout the data collection period.
References
- American Diabetes Association. (2014). Diagnosis and classification of diabetes mellitus. Diabetes care, 37(Supplement_1), S81-S90.
- Yahaya, T. O., Sifau, M. O., Oladele, E. O., Bashar, D.M., Abubakar, A. L., Salisu, N., ... & Koko, J. D. (2022). HYPERGLYCEMIA PREVALENCE AMONG ARTISANS AND WORKERS IN SELECTED FACTORIES IN LAGOS, SOUTHWEST, NIGERIA. Folia MedicaIndonesiana, 58(2), 168-177.
- Peer, N., Kengne, A. P., Motala, A. A., & Mbanya, J. C. (2014). Diabetes in the Africa Region: an update. Diabetes research and clinical practice, 103(2), 197-205.
- American Diabetes Association. 6. Glycemic targets: standards of medical care in diabetes—2020. Diabetes care. 2020 Jan 1;43(Supplement_1):S66-76.
- Demilew, Y. M., Alem, A. T., & Emiru, A. A. (2018). Dietary practice and associated factors among type 2 diabetic patients in Felege Hiwot Regional Referral Hospital, Bahir Dar, Ethiopia. BMC research notes, 11, 1-7.
- Ouyang, C. M. (2017). Dietary education for patients with type 2 diabetes: failure or success. Diabetes Manag, 7(5), 377-82.
- World Health Organization. (2018). A healthy diet sustainably produced: information sheet (No. WHO/NMH/ NHD/18.12). World Health Organization.
- Abebe, N., Kebede, T., & Addise, D. (2017). Diabetes in Ethiopia 2000–2016 prevalence and related acute and chronic complications; a systematic review. Afr J Diabetes Med, 25(2), 7-12.
- Shamsi, N., Shehab, Z., AlNahash, Z., AlMuhanadi, S., &Al-Nasir, F. (2013). Factors Influencing Dietary Practiceamong Type 2 Diabetics. Bahrain medical bulletin, 35(3).
- Ganiyu, A. B., Mabuza, L. H., Malete, N. H., Govender, I., & Ogunbanjo, G. A. (2013). Non-adherence to diet and exercise recommendations amongst patients with type 2 diabetes mellitus attending Extension II Clinic in Botswana. African Journal of Primary Health Care and Family Medicine, 5(1), 1-6.
- Bano, A., Afzal, M., Sarwar, H., Waqas, A., Kousar, S., & Gulzar, S. (2017). Dietary knowledge, attitude and practices of diabetes patients at services hospital Lahore. International Journal of Applied Sciences and Biotechnology, 5(2), 227- 236.
- Worku, A., Mekonnen Abebe, S., & Wassie, M. M. (2015). Dietary practice and associated factors among type 2 diabetic patients: a cross sectional hospital based study, Addis Ababa, Ethiopia. SpringerPlus, 4, 1-8.
- Abejew, A. A., Belay, A. Z., & Kerie, M. W. (2015). Diabetic complications among adult diabetic patients of a tertiary hospital in northeast Ethiopia. Advances in Public Health, 2015.
- Sami, W., Ansari, T., Butt, N. S., & Ab Hamid, M. R. (2017). Effect of diet on type 2 diabetes mellitus: A review. International journal of health sciences, 11(2), 65.
- ADA.,. A brief overview of diabetes and the american diabetes association ,2014.
- Hallberg, S. J., Dockter, N. E., Kushner, J. A., & Athinarayanan, S. J. (2019). Improving the scientific rigour of nutritional recommendations for adults with type 2 diabetes: A comprehensive review of the American Diabetes Association guidelineâ?recommended eating patterns. Diabetes, Obesity and Metabolism, 21(8), 1769-1779.
- Al-Bayyari, N. S. (2017). Assessment of Dietary and Life- Style Behaviors of Diabetic and Non-Diabetic Jordanian Atorvastatin Users.
- Sun, H., Saeedi, P., Karuranga, S., Pinkepank, M., Ogurtsova, K., Duncan, B. B., ... & Magliano, D. J. (2022). IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes research and clinical practice, 183, 109119.
- Aschalew, A. Y., Yitayal, M., Minyihun, A., & Bisetegn, T.A. (2019). Self-care practice and associated factors among patients with diabetes mellitus on follow up at University of Gondar Referral Hospital, Gondar, Northwest Ethiopia. BMC research notes, 12, 1-6.
- Wahome, E. M., Makau, W. K., & Kiboi, W. K. (2018). Predictors of dietary practices and nutritional status among diabetic type II patients in Kiambu County, Kenya. International Journal of Community Medicine and Public Health, 5(7), 2726-2734.