
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2019) Volume 1, Issue 1
Dietary Dialysis with Acacia Gum: Intestinal Dialysis Technology
2Advisor Doctor, Baghdad Medical City, Baghdad, Iraq
Received Date: Sep 30, 2019 / Accepted Date: Oct 03, 2019 / Published Date: Nov 18, 2019
Copyright: ©Aamir Jalal Al Mosawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The use of a new dietary approach used to lower urea levels in chronic renal failure, and thus simulating dialysis has been recently described. This approach has been increasingly called intestinal or dietary dialysis. The aim of this paper is to describe the treatment of nine patients with chronic renal failure associated with symptomatic uremia with intestinal dialysis.
Patients and Methods: During the period from December, 2005 to October, 2009, nine patients (5 males and 4 females) with various renal disorders associated with symptomatic uremia were referred for treatment due to their unwillingness to undergo dialysis. Ages ranged from 3.5 year to 72 years (mean 28.8).All patients considered dialysis in their circumstance to be associated with an unacceptable degree of discomfort and suffering. Five patients had severe uremic symptoms (fatigability, tachypnea, and anorexia). All of the patients were unable to walk independently. The patients were treated with the new technology of intestinal dialysis.
Results: All the patients enrolled experienced amelioration of symptoms of uremia with improved general wellbeing in association with lowering of urea levels and creatinine during the period of therapy. They patients were followed for a period ranging from 8 weeks to 8 years. It was possible to follow three patients for more than 2 years on this therapy, and one patient was followed for about 8 years. They three patients continued to experience low urea levels and didn’t develop any symptoms of uremia. No important side effect was observed. However, most patients experienced some degree of abdominal distention associated with increased passage of gases (flatulence).
Conclusion: Patients treated with intestinal dialysis experienced conspicuous lowering of urea and creatinine and improvement in the general wellbeing.
Keywords
Symptomatic uremia, intestinal dialysis, dietary dialysis, acacia gum; urea lowering effect.
Introduction
The use of a new dietary approach used to lower urea levels in chronic renal failure, and thus simulating dialysis has been recently described and was called intestinal and dietary dialysis. This approach has been increasingly called intestinal or dietary dialysis [1-4].
Chronic renal failure is associated clinically with the development of the uremic syndrome which is the complex of signs and symptoms resulting from the retention of nitrogenous waste products, imbalance in the body content and distribution of water and electrolytes, and from abnormalities of hormone functions. The most prominent features of the uremic syndrome result from nitrogen retention with associated with increase in plasma concentration of the products of protein metabolism especially urea. Retention of metabolites is associated with the adverse clinical symptoms of uremia such as nausea, anorexia, vomiting and fatigue, in addition to many other systemic manifestations such as acidosis, anemia, fluid/electrolyte imbalance, and overabundance of toxic substances especially urea and its byproducts in the blood. The uremic syndrome is also associated with an inadequate production of renal hormones including erythropoietin and 1-25 dihydroxyvitamin D and abnormal production or use of growth hormone by tissues [1, 2, and 5].
Ingested proteins are degraded into amino acids and their metabolism by the liver yield nitrogen, mainly in the form of urea. Urea has to be excreted mostly by the kidneys. Ammonia is produced from dietary amino acids and by catabolism of amino acids and amines in peripheral tissues especially skeletal muscle. 80-90% of the ammonia produced is shunted into the urea cycle, while 10-20% metabolized by peripheral tissues, including the kidney, heart, and brain. The thing in urea metabolism that is very relevant to intestinal dialysis is the enterohepatic cycle of urea. Gastrointestinal micro¬organisms (primarily coliforms and anaerobes in the colon and cecum) convert dietary amino acids and urea into ammonia in the gastrointestinal tract. The ammonia is absorbed into the portal circulation, taken up by the liver and converted in the liver into urea. Ammonia (resulting from protein degradation to amino acids and amino acids metabolism) will either pass to the portal circulation or enter the liver ornithine urea cycle for conversion to urea which is excreted by the kidneys or it is exposed in the gastrointestinal tract to bacterial hydrolysis by ureases and proteases, and excreted fecally. Approximately 25-40 % of the manufactured urea are recycled through the gastrointestinal tract and excreted fecally. This extra-renal excretion of urea remains constant at less than 3 g daily even in uremia despite the marked increases in blood urea [1, 2, 5].
In contrast to fats and carbohydrate, which are metabolized to carbon dioxide, which is easily excreted even in uremic subjects via lung and skin, the products of protein and amino acid metabolism depend largely on the kidney for excretion. Several products of protein metabolism have been identified, with urea being quantitively the most important. Urea represents 80% or more of the total nitrogen excreted into the urine in patients with chronic renal failure maintained on diets containing 40 g or more of protein.
Peritoneal dialysis actually acts by shifting the urinary excretion of urea to the peritoneal excretion with use of intraperitoneal dialysis fluids. The use of a dietary material to increase this extra renal excretion and shift the urinary excretion of urea to the intestinal excretion has been increasingly called intestinal dialysis technology [3, 4].
Management of non-terminal chronic renal failure is largely based on compensating the diminished renal functions conservatively through the traditional dietary and pharmacologic measures which include protein and phosphorus restriction, calorie and water soluble vitamins supplementation, phosphate binders, and correction of other abnormalities that may be associated with chronic renal failure such as fluid and salt retention, hypocalcaemia, hyperkalemia, and hypertension. In principle, the dietary interventions in chronic renal failure are traditionally directed mainly toward diminishing the accumulation of the products of nitrogen metabolism which are responsible for many of the symptoms and disturbances of uremia and thus preventing the development of the uremic symptomatology and complications [1, 2, 5].
The biologic value of protein is a measure of its content of essential amino acids and proteins with high biologic value protein should contain all the essential amino acids and have a concentration of each amino acid roughly proportional to its minimal daily requirement. High biologic value protein helps in reducing the accumulation of nitrogenous waste products and acid load for renal excretion and also helps in maintaining a positive nitrogen balance. Egg protein has the highest biologic value (1 large egg contains 6 g protein). It’s very difficult and not really practical to limit the intake of proteins only to the high biologic value egg protein, and preferably 50% of the protein intake should be provided as egg, and the other 50% provided with the intake of vegetables, pasta, rice, and bread. Thus, avoiding restriction of caloric intake which may lead to negative nitrogen balance, muscle wasting and growth failure in case of children [1, 2, 5, 6].
Protein restriction decreases endogenous protein catabolism and the accumulation of nitrogenous waste products. Protein restriction also reduces the phosphorus load and thus helps in preventing the onset of secondary hyperparathyroidism and renal osteodystrophy associated with chronic renal failure. Protein restriction reduces the intake of potential hydrogen ion, because every 10 g of protein provides 7 meq of hydrogen ion in the form of sulfated amino-acids. Thus. Protein restriction helps also to ameliorate the acidosis in chronic renal failure. The second necessary strategy directed toward diminishing the accumulation of the products of nitrogen metabolism in chronic renal failure is the provision of adequate caloric intake to minimize protein breakdown. Adequate intake of carbohydrate and fats is necessary to compensate for protein restriction. Glucose and other carbohydrates are protein sparing and decrease endogenous protein catabolism and the production of urea. 75 g glucose per square meter or 300 Cal daily has been considered to be effective in minimizing endogenous protein catabolism. Fats are less effective than carbohydrates in minimizing protein catabolism, but they are given to provide essential fatty acids and to enhance the palatability of the diet. In the absence of diabetes, there is no limit to the to the amount of carbohydrate and fat that can be taken. Carbohydrates can be taken as sugar, Jam, and honey. The major source of fats in the diet is oils, butter, and fresh cream [1, 2, 5, 7].
Dietary restrictions of sodium and potassium depend on the presence of oliguria, edema, hypertension, and hyperkalemia. Uremic patients who have no problem with hypertension or edema can take up to 2 g (80 meq) of sodium daily by just avoiding salty foods and add no salts at the table. If hypertension or edema develops, sodium intake is restricted to 1 meq /kg and occasionally to 0.2 meq/kg/day. When such diet is unsuccessful or too unpalatable, oral frusemide is added to the regimen (1-2mg/kg/day) [1, 2, 5, 7].
Various pharmacologic measures are also used in the treatment of chronic renal failure which are aiming at prevention or correction of abnormalities which are expected to appear during the course of chronic renal failure including iron, vitamins deficiencies, hypocalcaemia, hyperphosphatemia, hypertension, acidosis, growth retardation, renal osteodystrophy [1, 2, 5, 7].
What makes intestinal (dietary) dialysis possible is the fact that with appropriate dietary and pharmacologic management, patients with non-terminal chronic renal failure can be maintained surprisingly well and the transition from non-terminal chronic renal failure to end-stage chronic renal failure represents a small decrement of renal function resulting in a large physiologic deterioration for the patient. Conservative (Dietary and pharmacologic) measures are only successful in non-terminal chronic renal failure patients. The addition to these effective traditional measures, a dietary agent or supplement that enhance extra-renal fecal nitrogen excretion can possibly bridge this gap resulting from this small decrement of renal function and possibly obviating the need dialysis for some period of time [1-8].
The aim of this paper is to describe the treatment of nine patients with chronic renal failure associated with symptomatic uremia with intestinal dialysis.
Patients and Methods
During the period from December, 2005 to October , 2009, nine patients (5 males and 4 females) with various renal disorders (Biopsy-proven focal segmental glomerulosclerosis (FSGS), biopsy proven membranous glomerulonephritis, diabetic nephropathy, cystinosis, bilateral renal stone disease, and infantile polycystic disease, chronic GN including familial GN) associated with symptomatic uremia were referred for treatment due to their unwillingness to undergo dialysis. Ages ranged from 3.5 year to 72 years (mean 28.8).All patients considered dialysis in their circumstance to be associated with an unacceptable degree of discomfort and suffering. Five patients had severe uremic symptoms (fatigability, tachypnea, and anorexia). All of the patients were unable to walk independently; one of them (patient-1) has undergone one session of intermittent peritoneal dialysis and was referred 3 days after dialysis, Four patients (2 , 3 and 4) refused dialysis session and were enrolled at the stage when dialysis was definitely indicated to maintain health and both patients had marked weakness. Patients (5) aged 72 years with chronic ischemic heart disease (on oral and sublingual nitrates) was considered by the dialysis team as a terminal patient and warned the family of the possibility of death during or after dialysis. Patient (2) with diabetic nephropathy was unable to stand and walk unaided. Patient 2, 3 and 4 required intramuscular pyridoxine and oral domperidone to control vomiting. Patients 3,4,5 were hospitalized before referral received therapies such as intravenous fluid, iv sodium bicarbonate, frusemide, iv calcium gluconate and cefotaxime .Patient 5 received one pint of blood because of the fall of hemoglobin below 7 g/dl.
Four patients had less severe uremic symptoms. Patient (9) presented with mild uremic symptoms, but he was referred early when he expressed his rejection to the currently available care for chronic renal failure.
None of patients had a life threatening uremic complication such gastrointestinal bleeding and encephalopathy on referral.
All patients were educated regarding the risks of uremia in the absence of maintenance dialysis. They were followed for a period ranging from 8 weeks to 7 years. Table-1 shows the patients characteristics
Table 1: Patients characteristics
|
Patients |
Age (yr) |
Sex |
Diagnosis |
Other Note |
|
1 |
63 |
M |
Bilateral renal stone disease |
|
|
2 |
28 |
F |
Insulin dependent diabetes and(diabetic nephropathy) |
|
|
3 |
9 |
F |
Cystinosis |
|
|
4 |
3.5 |
M |
Infantile polycystic kidney disease with hepatomegaly |
|
|
5 |
72 |
|
Chronic non specific Glomerulonephritis |
Known to have ischemic heart disease |
|
6 |
23 |
M |
Biopsy proven membranous Glomerulonephritis diagnosed at the age of 17 |
Receiving losartan 50 mg daily |
|
7 |
3.7 |
F |
Chronic Glomerulonephritis presented initially with steroid sensitive nephritic syndrome. |
Father died from uremia before the age of 40. Received prednisone and cyclosporine before the onset of chronic renal failure.Receiving losartan and enalapril |
|
8 |
5 |
M |
Chronic Glomerulonephritis presented initially with steroid sensitive nephritic syndrome. |
His brother with steroid resistant nephrotic syndrome died from uremia 1 week before referral. |
|
9 |
52 |
M |
Biopsy proven FSGS |
Receiving losartan and enalapril |
The patients were already on a low protein diet and other pharmacological measures of chronic renal failure, such as iron, and calcium carbonate, one-alfacalcidol supplementation, erythropoietin, antihypertensive drugs and diuretics. These dietary and pharmacological measures were reviewed and adjusted as necessary according to the clinical findings and blood levels of hemoglobin, calcium and potassium. Three patients (patients 2, 3 and 4) required intramuscular iron to maintain hemoglobin. Patient (1) was switched to weekly intra-muscular iron to reduce the number of orally administered medications. Only one patients (with cystinosis) received erythropoietin because of shortage of erythropoietin during the period of the study. Patient (2) with diabetic nephropathy was on low calorie diet and was receiving insulin.
Dietary proteins were restricted to 1 g/kg/day for patients under the age of 10 years, and 0.5 g/kg for patients over the age of 10 years with at least 50% of the total intake given as egg albumin. Protein and phosphorus restriction was primarily achieved by restricting meat, poultry, fish, milk, cheese and yogurt. Additional restrictions were made on potassium-rich foods during elevation of serum potassium above 5 mmol/l. Powder acacia 1 g/kg/day (maximum 75 g) was supplied in 2-3 divided doses (diluted with the desired amount of water).
The efficacy of treatment was primarily measured by clinical improvement with amelioration of the symptoms of uremia (anorexia, vomiting, and fatigability) and biochemical improvements, primarily measured by lowering of blood urea and serum creatinine .The protocol for this research was approved by the scientific committee of the University Hospital in Al Kadhimiyia (Iraq) and the scientific committee if Iraq headquarter of Copernicus Scientists International Panel , and it conforms to the provisions laid out in the Declaration of Helsinki (as revised in Edinburgh 2000)
Results
All the patients enrolled experienced amelioration of symptoms of uremia with improved general wellbeing in association with lowering of urea levels and creatinine during the period of therapy. The effect of acacia supplementation was more dramatic in patients (2&3) as they were enrolled with severe uremic symptoms, at the stage when dialysis was definitely indicated to maintain health and both patients had marked weakness. Patient (2) who was unable to stand and walk unaided before the start of therapy was able to climb more than 10 steps upstairs unaided after 3 weeks of therapy.
Table-2 summarized the effects of intestinal dialysis (acacia gum supplementation of low protein diet) on serum creatinine, blood urea, and Blood urea nitrogen.
Table 2: The effects of intestinal dialysis (acacia gum supplementation of low protein diet) on serum creatinine, blood urea, and Blood urea nitrogen
|
Patient |
Time |
Serum creatinine mg/dl |
Blood urea mg/dl |
Blood urea nitrogen mg/dl |
|
1 |
Start of therapy (Post-dialysis) After 2 weeks After 6 weeks After 10 weeks |
6.2 3 1.1 1 |
120 75 47 46 |
53.3 33.3 21 21 |
|
2 |
Start of therapy After 3 weeks After 5 weeks After 9 weeks |
9 6 4.3 3.7 |
219 136 130 114 |
97.3 60.4 57.7 50.7 |
|
3 |
Start of therapy After 2 weeks After 5 weeks After 8 weeks |
6.7 1.9 ----- |
200 69 68 60 |
90 30.6 30.2 26.6 |
|
4 |
Start of therapy After 4 weeks (11/8/070 After 7 weeks |
4.7 2.8 (received blood). 1.6 |
157 112 59 (PCV 29) |
69.7 49.7 26.2 |
|
5 |
Start of therapy After 4 weeks |
4.8 mg/dl 1 mg |
162 mg 53 mg |
72 23.5 |
|
6 |
Start of therapy [2-5-2008] After 2 week [10-5-2008] After 4 weeks [4-6-2008] After 9 weeks |
4 1.8 1.6 1. 6 |
100 75 67 60 |
44.4 33.3 29.8 26.7 |
|
7 |
Start of therapy After 4 weeks After 8 weeks |
8.4 2.8 2 |
96 35 35 |
42.7 15.5 15.5 |
|
8 |
Start of therapy After 4 weeks After 8 weeks |
0.6 |
89 68 36 |
39.5 30.2 16 |
|
9 |
Start of therapy After 2 weeks After 6 weeks After 10 weeks After 18 weeks |
3.1 2.1 2 1 0.9 |
94 84 70 52 43 |
41.7 37.3 31 23 19 |
After 2-4 weeks of therapy, the mean blood urea level was reduced from 137.45 mg/dl (Mean BUN 61 mg/dl) before the start of therapy to 78.5 mg/dl (Mean BUN 34.5 mg/dl). Within 5-10 weeks of therapy, mean blood urea level was 60 mg/dl (Mean BUN 25.7 mg/dl). Figure-1 shows the mean blood urea and BUN during the period of therapy.
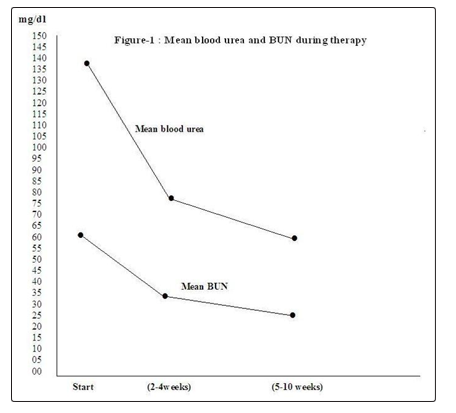
Figure 1: The mean blood urea and BUN during therapy.
It was possible to follow three patients (7, 8 and 9) for more than 2 years on this therapy, and one patient, patient (8) was followed for about 8 years. They three patients continued to experience low urea levels and didn’t develop any symptoms of uremia. No important side effect was observed. However, most patients experienced some degree of abdominal distention associated with increased passage of gases (flatulence).
Discussion
In 1980, Yazidis et al showed that dietary fiber (locust bean gum) supplementation of chronic renal failure patients on low-protein diet reduced serum urea and creatinine by 11-23% over 5 days of administration. Improvement of clinical symptoms was observed during administration and deterioration when supplementation was withheld. In 1984, Rampton et al reported that six and eight weeks of is paghula and arabinogalactan reduced meaning plasma urea level in uremic patients 19% and 11% respectively. However, the use of locust bean gum and is paghula were not considered to have practical value for clinical use because of the development of side effects. The use of locust bean gum was associated with two to three soft voluminous stools per day that had an unusual bad smell, and more important it the low palatability was considered a serious disadvantage. Similarly patient’s ingested is paghula found it unpalatable, felt unwell, or had diarrhea. In 1996, Tetens et al showed in an experimental study on rat that dietary fiber (maize bran) supplementation caused a dose dependent significant increase in fecal nitrogen excretion in association with reduction in nitrogen retention. The shift in nitrogen excretion from urine to feces was explained largely by the degree of microbial fermentation in the large intestine caused by dietary fiber supplementation that have modifying role on the enterohepatic cycle of nitrogen. In 1996, Bliss et al reported a study included 16 adult patients with asymptomatic non-terminal chronic renal failure on low protein diet, they were randomly assigned to receive a supplement of acacia gum (50 g daily) or oral placebo (1 g daily). Acacia gum supplementation was associated with lower serum urea, and the patients had greater fecal masses and greater fecal nitrogen excretion in comparison with period there were on low protein diet alone and in comparison with a control patients on pectin supplementation instead of acacia. In contrast to locust bean gum and is paghula, patients ingesting acacia gum found it palatable and the clinical use of acacia gum was considered applicable [1,2,3].
Early during the 2000s, children with chronic renal failure in Baghdad and Iraq were mostly treated with intermittent peritoneal dialysis using temporary peritoneal catheters, and treatment was associated was associated with a significant and an acceptable risk of morbidity and mortality, and many parents were taking their children to die at home without subjecting them to dialysis. During these years, Al-Mosawi was left with no choice other than trying something new to improve the management of children with chronic renal failure [9, 10]. Despite the significant lowering of urea levels associated with intestinal dialysis, the process of urea lowering is slow and its effectiveness remains less than the traditional dialysis especially in the more advanced stages of chronic renal failure. Therefore, the combined use of intestinal dialysis with intermittent peritoneal dialysis was the first reported use of intestinal dialysis in symptomatic urea. Early during the 2000s, Al-Mosawi started adopting the practices of evidence-based medicine to deal with the therapeutic challenges and improve the patients care, and he developed the strategy of intestinal dialysis accordingly. Al-Mosawi tried to share my early experiences in the practice of evidence-based medicine with world scientific leaders in the fields of pediatrics and nephrology. Therefore, Al-Mosawi wrote to Ira Greifer, a pioneer of pediatric nephrology (Figure-2) who was the secretary general of the International Association of Pediatric Nephrology during that time.
Figure 2: Ira Greifer, a pioneer of pediatric nephrology
It was not long time when Al-Mosawi received a reply from Ira Griefer. He wrote “ I was very pleased to receive your letter and know that you are working very hard to bring the benefit of modern knowledge, techniques and treatment to children in your country with Kidney and Urologic problems.” Figures 3A and B show the 2-page letter of Ira Greifer.
Ira Greifer also wrote “I was most fascinated by your use of gum Arabic in children with chronic renal failure, in attempt to promote low protein diet. With this experience and your general experience with acute glomerular nephritis in Iraqi children, should be considered for publication in our journal “Pediatric Nephrology”, if it was presented for review to our editors.”
Thereafter, the first clinical use of intestinal dialysis in symptomatic uremia was published during May, 2002, in Pediatric Nephrology” [9]. Al-Mosawi described the use of intestinal dialysis (acacia gum supplementation and low protein diet) with intermittent peritoneal dialysis to treat a seven year old boy with the most extreme form of end-stage renal disease (anuric with no renal function).
The patient was treated initially with intermittent peritoneal dialysis and conservative medical treatment (low protein diet and fluid restriction). He was treated with peritoneal dialysis sessions intermittently whenever became symptomatic with marked nausea, tachypnea (acidotic breathing), and generalized edema from fluid overload.
When the patient described by Al-Mosawi was symptomatic, blood urea usually ranged from 37.4 to53.9 mmol/l. After each 24-72 hour peritoneal dialysis session, blood urea usually fell to below 16.6 mmol/l. During 108 days of anuria, he was treated with 12 sessions of intermittent peritoneal dialysis (average frequency: one session of dialysis/ 9 days).
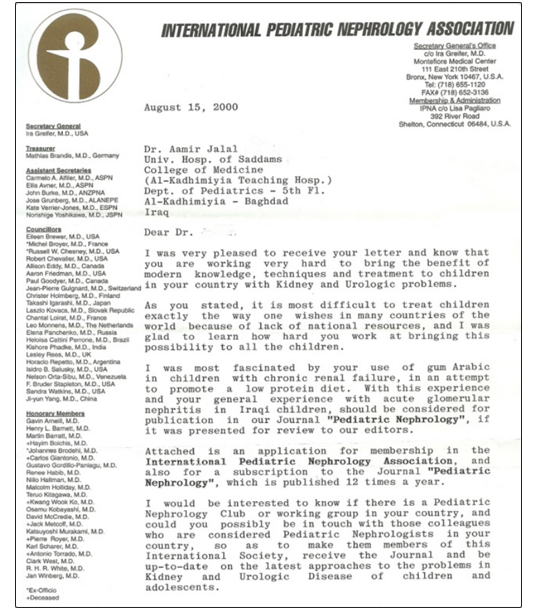
Figure 3A: The 2-page letter of Ira Greifer
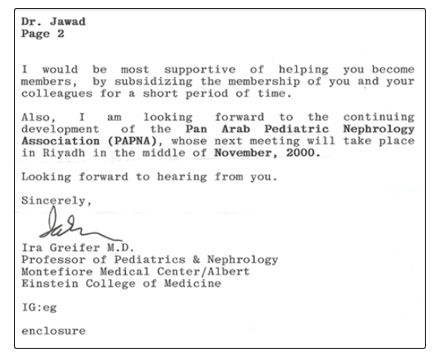
Figure 3B: The 2-page letter of Ira Greifer
Despite earlier institution of low-protein diet and fluid restriction, the required 12 sessions of peritoneal dialysis and was receiving nifedipine 2 mg/kg daily to control hypertension. His diastolic blood pressure was reduced to 100 mmHg. He was also given frusemide for 3 days, but the effect was almost negligible. Propranolol was added at a dose of 2 mg/kg daily and lowered blood pressure to 120/80 mmHg. Intestinal dialysis was initiated and continued for 48 days. Dietary protein was restricted to 0.5 g/kg per day given largely in the form of egg albumin. Fluid and salt were also restricted. A high-caloric diet was encouraged, together with supplements of water-soluble vitamins, calcium, and iron. Acacia gum powder was given at a dose of 0.5 g/kg per day in 2-3 divided doses. Acacia gum was diluted with the minimal amount of water to make it acceptable. The patient became symptomatic with anorexia, tachypnea (acidotic breathing), and edema 27 days after the initiation of intestinal dialysis. His blood urea was 49.8 mmol/l and he required a dialysis session. The child became symptomatic and needed the second session of intermittent peritoneal dialysis after another 21 days. Compliance with all of the components of intestinal dialysis was better during the first 27 days of therapy. After two weeks of the initiation of intestinal dialysis, it was necessary to stop antihypertensive medications (nifedipine and propranolol) because the diastolic blood pressure dropped to 45–50 mmHg for no obvious reason (such as gastrointestinal bleeding). Although the parents noticed the beneficial effect of intestinal dialysis, they couldn’t ensure the child’s compliance with treatment. The child and his parents were overwhelmed by the illness. Non adherence to intestinal dialysis therapeutic components led to severe hypertension (blood pressure 160/140 mmHg) and the uremic symptoms reappeared, and the child died shortly after an intermittent peritoneal dialysis session. The child found acacia gum ingestion acceptable (palatable), but taking it was associated with one or two voluminous stools per day that had an unusual smell (similar to the smell of urine). This effect of acacia on stool did not interfere with compliance. A suitable dose of acacia gum powder was 0.5 g/kg per day. A trial of a higher dose of 1 g/kg per day in this patient was performed in an attempt to increase the efficiency of intestinal dialysis. However, this increase resulted in abdominal distention and discomfort that interfered with sleep at night. The dose of acacia gum powder was reduced again to 0.5 g/kg per day. In this child, intestinal dialysis was associated with a beneficial antihypertensive effect. Before the initiation of intestinal dialysis, diastolic blood pressure was maintained at 80 mmHg with nifedipine and propranolol. Diastolic blood pressure was maintained at 80 mmHg with intestinal dialysis alone for 3 weeks. During the first three weeks after the initiation of intestinal dialysis therapy, blood urea was maintained below 33.2 mmol/l. The child remained relatively well without being significantly symptomatic. His appetite was good and he was not clinically acidotic. The child became symptomatic 27 days after the initiation of intestinal dialysis and required a second intermittent peritoneal dialysis session after another 21 days [9].
The second paper reporting the use on intestinal dialysis in symptomatic uremia described the long-term achievement of peritoneal dialysis freedom in few patients who have less severe disease than the first patient with symptomatic uremia treated with this method, and they had excellent compliances with the therapy. Six patients with end-stage renal disease and significant uremia that required at least one dialysis session to maintain life were studied. Intestinal dialysis was initiated in three of the six patients with the aim of improving wellbeing and reducing the need for dialysis. The other three patients were treated with intermittent peritoneal dialysis; all died with in less than 6 months.The three patients treated with intestinal dialysis aged between 11-13 years (each with, oxalosis, cystinosis, and end-stage renal disease of undetermined etiology), and had symptomatic uremia required at least one session of intermittent peritoneal dialysis despite low-protein diet and other conservative measures of chronic renal failure. They had no reductions in urine output or edema and were normotensive. Their pre -dialysis creatinine clearance was less than 5 ml/min when by a formula developed by Cock and Gault. One of the patients complied with intestinal dialysis therapy for only 10 days and died after 6 months despite treating him with intermittent peritoneal dialysis. Two of the three patients were treated for one year with intestinal dialysis. Both patients reported improved wellbeing. Neither became acidotic or uremic, and neither required dialysis during the one year of the study period. Both patients maintained serum creatinine and urea levels not previously achieved without dialysis.
Of the 2 surviving patients treated with intestinal dialysis, one patient couldn’t comply with therapy and stopped most of the components of intestinal dialysis after one year and died within one month despite treatment with intermittent peritoneal dialysis. The other patient continued to be treated with intestinal dialysis and continued to experience improved wellbeing and dialysis freedom during 6 completed years [11, 12, and 13].
The patient who achieved six-year dialysis freedom was an 11-year-old girl with End-renal failure who initially required four sessions of intermittent peritoneal dialysis to control uremic symptoms despite conservative measures. The parents refused further treatment by dialysis .Thereafter; she was managed with intestinal dialysis. During 6 years of therapy the girl continued in experiencing improved well-being and good participation in outdoor activities. Mild uremic symptoms occurred only during periods of noncompliance. Periods of decreased compliance with pharmacologic therapies were associated with anemia and renal osteodystrophy and some degree genue vulgum has resulted. The chronicity of her illness was confirmed by the presence of small contracted kidneys, a finding that has not changed during the subsequent follow-up [13].
In 2006, Al-Mosaw published a research paper describing the use of intestinal dialysis in 11 adult patients with symptomatic uremia. Their ages ranged from 14 to 65 years (Mean 41.45 year). Two of them were on hemodialysis. The remaining patients were on low protein diet combined with other medical treatments of chronic renal failure, including one patient has undergone one peritoneal dialysis session before referral. The intestinal dialysis therapeutic regimen included dietary proteins restriction to 0.5 g/kg with at least 50% of the total intake given as egg albumin. Protein and phosphorus restriction was primarily achieved by restriction of meat, poultry, fish, milk, cheese, yogurt, and legumes. Additional restriction of potassium rich foods was made during elevation of serum potassium above 5 mmol /L. Powder acacia gum 1g/kg/day (Maximum 75 g) in 2-3 divided doses diluted with desired amounts of water. The use of intestinal dialysis in this study was associated with amelioration of the uremic symptoms and improved general wellbeing as long as the patients were compliant with the therapeutic protocol. The patients were followed for 2-16 weeks. However, the most significant finding in this study was the achievement of hemodialysis freedom in 2 of these patients, both of them has a vascular access, but they considered hemodialysis to be associated with a significant amount of discomfort and suffering, and they were not satisfied with the quality of life associated with hemodialysis. Two patients who didn’t comply with the therapeutic protocol died, one during treatment with intermittent peritoneal dialysis and one within one month after renal transplantation [14].
Conclusion
Patients treated with intestinal dialysis experienced conspicuous lowering of urea and creatinine and improvement in the general wellbeing.
References
- Al-Mosawi AJ (2011) Intestinal dialysis: A new therapy for chronic renal failure. LAP LAMBERT Academic Publishing GmbH &Co.KG (ISBN: 9783847304470).
- Al-Mosawi AJ (2013) A new dietary therapy for chronic renal failure. LAP LAMBERT Academic Publishing GmbH& Co. KG (ISBN: 978-3-659-51436-4).
- Al-Mosawi AJ (2017) Advances of Peritoneal Dialysis in the Developing World: Combined Intermittent Peritoneal Dialysis and Intestinal Dialysis (Chapter 3). In Marcia Bell Ed. Nova Science Publisher (ISBN: 978-1-53610-535-3).
- Mosawi AJ (2010) Advances in Peritoneal Dialysis (Chapter 2). In Anil K. Agarwal, Loay Salman, Arif Asif Ed. Nova Science Publisher, New York, pp. 17-68.
- Al-Mosawi AJ (2006) Acacia gum therapeutic potential: possible role in the management of uremia: a new potential medicine. Therapy 3: 301-321.
- Al-Mosawi AJ (2006) Principles: clinical pathophysiology of uremia and relevant urea metabolism Therapy (Clinical practice) 3: 303-304.
- Al-Mosawi AJ (2006) The conservative management of non-terminal chronic renal failure (Clinical practice) Therapy (Clinical practice) 3: 305-306.
- AJ-Al-Mosawi (2008) Childhood chronic renal failure (CRF): An extraordinary experience Arch. Dis. Child 93: 384.
- Al-Mosawi AJ (2002) The challenge of chronic renal failure in the developing world: possible use of acacia gum. Pediatr Nephrol 17: 390-1.
- Al-Mosawi AJ (2019) Scientific productivity of Iraqi pediatricians in pediatric nephrology .1st ed., Saarbrücken; LAP Lambert Academic Publishing (ISBN: 978-620-0-32300-2).
- Al-Mosawi AJ (2004) Acacia gum supplementation of a low-protein diet in children with end-stage renal disease. Pediatr Nephrol 19: 1156-9.
- Al-Mosawi AJ (2007) The use of acacia gum in end stage renal failure. J Trop Pediatr 53: 362-5.
- Al-Mosawi AJ (2009) Six-year dialysis freedom in end-stage renal disease. Clin Exp Nephrol 13: 494-500.
- Al-Mosawi AJ (2006) Continuous renal replacement in the developing world: Is there any alternative. Therapy (London) 3: 265-272.