
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2025) Volume 10, Issue 1
Determinants of Hepatitis B Virus Among Pregnant Women Attending Antenatal Care Visit at Comprehensive Specialized Hospital in Central Ethiopia Region
2Student in Department of Comprehensive Nursing College of Medicine and Health Sciences, Wachemo Univ, Ethiopia
3Department of Nursing College of Health Sciences, Mettu University, Mettu, Ethiopia
4Department of Pediatrics and Child Health Nursing College of Medicine and Health Sciences, Wachemo U, Ethiopia
Received Date: Nov 25, 2024 / Accepted Date: Jan 30, 2025 / Published Date: Feb 20, 2025
Copyright: ©©2025 Elias Ezo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ezo, E., Teketel, M., Teshale, L., Gezimu, W., Zekiwos, A., et al. (2025). Determinants of Hepatitis B Virus Among Pregnant Women Attending Antenatal Care Visit at Comprehensive Specialized Hospital in Central Ethiopia Region. Int J Women
Abstract
Objective: To identify the determinants of the Hepatitis B virus among pregnant women attending antenatal care visits at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023.
Methods: A hospital-based unmatched case-control study design was conducted from July 3 to December 29/2023. The total sample size was 249 (166 controls and 83 cases). A systematic random sampling technique was used. Data were entered using Epi data 3.1 version and analyzed using SPSS version 25. Multicollinearity was checked by considering a variance inflation factor of greater than 10 and a tolerance of less than 0.05. The goodness of fit test was checked by using the Hosmer- Lemeshow goodness of fit test. Binary logistic regression analysis was done, and variables with a p-value of < 0.25 in the bivariable analysis were taken into the multivariable analysis. Statistical significance was declared at a p-value of < 0.05 with an adjusted odds ratio (AOR) and 95% confidence interval (CI).
Result: In this study, being rural residence [AOR 5.74, 95%CI: 1.94-16.95] having poor knowledge about Hepatitis B virus [AOR 0.15, 95%CI: 0.07-0.34], having a history of abortion [AOR 4.56, 95%CI: 1.66-12.53], having a history of female genital mutilation [AOR 5.29, 95%CI: 2.52-11.09], having history of sexually transmitted infection [AOR 4.62, 95%CI: 1.26- 16.97], and having history of contact with a jaundice person [AOR 6.43, 95%CI: 1.53-26.94] were significantly associated.
Conclusion: In this study, residence, knowledge about Hepatitis B virus, history of abortion, history of female genital mutilation, history of sexually transmitted infection, and history of contact with a jaundiced person were found to be significant determinants of Hepatitis B virus infection. Therefore, creating awareness about the Hepatitis B virus, practicing safe abortion, avoiding female genital mutilation, preventing sexually transmitted infections, and avoiding unnecessary contact with a jaundiced person may minimize the burden of Hepatitis B virus.
Keywords
Determinants, Hepatitis B Virus, Pregnant Women, Antenatal Care Visit
Introduction
Literatures show that the HBV infection among pregnant women is associated with various factors across studies [12-17]. Studies from different settings are crucial to precisely measure the burden of the problem and to make informed decisions. However, these studies are cross sectional that assessed the prevalence at a single period of time even there was association. Identifying the determinants of HBV infection and targeting on the factors would decrease the potential impact of HBV on maternal and child health. This study focused on Therefore, this study aimed to identify the determinants of the Hepatitis B virus among pregnant women attending antenatal care visits at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023.
Methods And Materials
Study Area and Period
The study was conducted at the antenatal care clinic of Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, in Hosanna town, Central Ethiopia. It is located 230 kilometers from Addis Ababa (the capital of Ethiopia). Hosanna is the administrative center and city of Central Ethiopia's regional state and Hadiya zone. Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital is one of the comprehensive specialized hospitals in the region and it is a teaching hospital of WA chemo University. The study was conducted from July 3 to December 29, 2023
Study Design
A hospital-based unmatched case-control study design was conducted
Study Population
All selected pregnant women attended the antenatal care clinic at Comprehensive Specialized Hospital in Central Ethiopia Region during the study period.
Control Definition
All selected pregnant women attending the antenatal care clinic at Comprehensive Specialized Hospital in Central Ethiopia Region whose laboratory result of HBV antigen was negative.
Case Definition
All selected pregnant women attending the antenatal care clinic at Comprehensive Specialized Hospital in Central Ethiopia Region whose laboratory result of HBV antigen was positive.
Eligibility Criteria
A pregnant woman attending the antenatal care clinic of Comprehensive Specialized Hospital in Central Ethiopia Region during the study period was included, whereas, pregnant women who visited more than one time at Comprehensive Specialized Hospital in Central Ethiopia Region excluded.
Sample Size Determination
The sample size for the study was determined by using Epi Info version 7 by considering the assumptions of 95% confidence level, 80% power, the ratio of control to case two to one (2:1), and adjusted odds ratio (AOR) from previous studies. A non-response rate of 10% was considered. (Table 1).
|
Variable |
% of control exposed |
AOR |
Sample size |
Total sample size with a 10% non-response rate |
References |
|
History of contact with liver disease patient |
5.6% |
5.6 |
135 |
149 |
(18) |
|
History of multiple sexual partners |
3.2% |
10.8 |
92 |
101 |
|
|
Tonsillectomy |
2.9% |
5.7 |
226 |
249 |
|
|
Educational status |
68.48% |
6.532 |
94 |
103 |
(19) |
Table 1: Sample Size Determination of Determinants of HBV among Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
From the calculated sample sizes above, 249 was the largest and it was the final sample size for this study.
Sampling Procedure
The average monthly flow of pregnant women to the ANC clinic was 291 and the six months flow was expected to be 1,746 (1,660 controls and 86 cases). Then, the women were selected by using a systematic random sampling technique for controls, considering a constant value of 10, which was obtained by dividing the total control population by the total control sample size (1,660/166) as there was no sampling frame. The first woman was determined by a lottery method and every tenth woman was interviewed until the required sample size of 166 was completed. However, the cases were included consecutively.
Study Variables
Dependent Variable: HBV
Independent Variable
.Sociodemographic Factors: Age, ethnicity, marital status, educational level, educational level of husbands, residence, occupation of husband, and income level.
. Maternity-Related Factors: Gravidity, parity, gestational age, history of home delivery, history of abortion, history of female genital mutilation, history of sexually transmitted infection, and HIV test result.
. Medical-Related Factors: History of jaundice, history of health facility admission, history of blood transfusion, and history of surgical procedure.
. Traditional Practice-Related Factors: Traditional means of dental extraction, history of body or ear piercing, history of tonsillectomy or vulvectomy, and history of contact with a jaundiced person.
. Personal and Familial Risky Behavior: History of sharp instrument injury, history of multiple sexual partners, history of previous marriage, and husband having another wife.
. Knowledge-Related Factor: knowledge of pregnant women about HBV.
Operational Definition
. Control: All selected pregnant women attending the antenatal care clinic at Comprehensive Specialized Hospital in Central Ethiopia Region whose laboratory result of HBV antigen was negative.
.Case: All selected pregnant women attending the antenatal care clinic at Comprehensive Specialized Hospital in Central Ethiopia Region whose laboratory result of HBV antigen was positive.
. Piercing: A type of body beautification where a sharp material punctures a hole in the body, ears, or nose parts where jewelry had been inserted [13-18,20].
.Tattoo: A form of body art that is created when ink is inserted, using a needle or other sharp materials into the dermis layer of the skin [18,20].
.Laboratory Investigation: The five milliliters of serum sample of the 249 recruited pregnant women were screened for HBV using latex rapid agglutination slide test for detecting hepatitis B surface antigen (HBsAg). Reactive samples were further confirmed for HBsAg using enzyme linked immunosorbent assay.
Data Collection Tool and Process
The tool was prepared in English containing sociodemographic factors, maternity-related factors, medical-related factors, traditional practice-related factors, personal and familial risky behavior, and knowledge-related factors adapted from various related literature [18, 20-24]. Two bachelor of sciences degree midwives were recruited for data collection. One gynecologist and one experienced epidemiologist were recruited for supervision
Data Quality Assurance
The questionnaire was translated to Amharic (the official language of Ethiopia) before data collection, and back to English after data collection to ensure consistency by language expertise. A Pre-test was done on 5% of the total sample size at Durame General Hospital and necessary modification was performed based on the pre-test. A-day training was given for data collectors and supervisors at the targets of the have a look at, how to pick out have a look at individuals, a way to preserve the confidentiality of statistics, the contents of the questionnaire, the way to interview and fill on fact’s series layout, and data exceptional management. The supervisors and investigators conducted everyday follow-ups during the whole period of data collection. Every day, after data collection, each questionnaire was reviewed and checked for completeness and the necessary feedback was given to the data collectors the next day. Cases and controls were identified by supervisors and the data collectors were blind to cases and controls.
Statistical Analysis
Data were entered using Epi data 3.1 version and analyzed using SPSS version 25. Data cleaning was performed to check for missed values and then descriptive analysis such as proportions, percentages, and mean were done and tables and graphs were used for presentation. Multicollinearity was checked by considering a variance inflation factor of greater than 10 and a tolerance of less than 0.05. The goodness of fit test was checked by using the Hosmer-Lemeshow goodness of fit test. Binary logistic regression analysis was done, and variables with a p-value of < 0.25 in the bivariable analysis were taken into the multivariable analysis. Statistical significance was declared at a p-value of < 0.05 with an AOR and 95% confidence interval.
Results
Socio-Demographic Characteristics
Two hundred forty-nine (166 controls and 83 cases) pregnant women were included in this study and that made the overall response rate 100%. About 68(41.0%) controls and 36(43.4%) cases were in the age group of 25-29 years old. More than half, 115(69.3%) controls and 63(75.9%) were from the ethnic group of Hadiyas. Majority, 157(94.6%) controls and 79(95.2%) cases were married. The educational status of 65(39.2%) controls and 30(36.1%) cases was grade 9-12th. Majority, 154(92.8%) controls and 70(84.3%) cases were live in urban. The occupation of 59(35.5%) controls and 30(36.1%) was house wife. The overall socio-demographic characteristics of pregnant women attending antenatal visits are described below. (Table 2).
|
Variables (n=249) |
Category |
Controls (n=166) |
Cases (n=83) |
||
|
Frequency |
Percent |
Frequency |
Percent |
||
|
The age group of women |
18-24 years old |
39 |
23.5 |
18 |
21.7 |
|
25-29 years old |
68 |
41.0 |
36 |
43.4 |
|
|
30-34 years old |
49 |
29.5 |
26 |
31.3 |
|
|
35-40 years old |
10 |
6.0 |
3 |
3.6 |
|
|
Ethnicity of women |
Hadiya |
115 |
69.3 |
63 |
75.9 |
|
Gurage |
11 |
6.6 |
3 |
3.6 |
|
|
|
Silte |
19 |
11.4 |
11 |
13.3 |
|
Kembata |
21 |
12.7 |
6 |
7.2 |
|
|
Marital status of women |
Married |
157 |
94.6 |
79 |
95.2 |
|
Single |
3 |
1.8 |
3 |
3.6 |
|
|
Divorced |
6 |
3.6 |
1 |
1.2 |
|
|
Educational status of women |
Grade 1-8th |
40 |
24.1 |
25 |
30.1 |
|
Grade 9-12th |
65 |
39.2 |
30 |
36.1 |
|
|
Diploma |
31 |
18.7 |
15 |
18.1 |
|
|
Degree and above |
30 |
18.1 |
13 |
15.7 |
|
|
Educational status of husbands (n=245) |
Grade 1-8 |
13 |
7.9 |
12 |
15.0 |
|
Grade 9-12 |
42 |
25.5 |
21 |
26.3 |
|
|
Diploma |
35 |
21.2 |
10 |
12.5 |
|
|
Degree and above |
75 |
45.5 |
37 |
46.3 |
|
|
Residence |
Urban |
154 |
92.8 |
70 |
84.3 |
|
Rural |
12 |
7.2 |
13 |
15.7 |
|
|
Occupation of women |
Housewife |
59 |
35.5 |
30 |
36.1 |
|
Student |
9 |
5.4 |
9 |
10.8 |
|
|
Gov't employee |
41 |
24.7 |
16 |
19.3 |
|
|
Private employee |
29 |
17.5 |
14 |
16.9 |
|
|
Merchant |
28 |
16.9 |
14 |
16.9 |
|
|
Occupation of husbands (n=245) |
Farmer |
13 |
7.9 |
11 |
13.8 |
|
Student |
2 |
1.2 |
34 |
42.5 |
|
|
Gov't employee |
79 |
47.9 |
13 |
16.3 |
|
|
Private employee |
32 |
19.4 |
11 |
13.8 |
|
|
Merchant |
27 |
16.4 |
11 |
13.8 |
|
|
Deriver |
12 |
7.3 |
11 |
13.8 |
|
|
Monthly income in Ethiopia birr |
<2000 birr |
16 |
9.6 |
12 |
14.5 |
|
2001-4000 birr |
45 |
27.1 |
18 |
21.7 |
|
|
4001-6000 birr |
58 |
34.9 |
28 |
33.7 |
|
|
>6000 birr |
47 |
28.3 |
25 |
30.1 |
Table 2: Socio-Demographic Characteristics of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Maternity Related Factors
More than half, 119(71.7%) controls and 59(71.1%) cases were multigravida. About 74(44.6%) controls and 38(45.8%) cases were multipara. The gestational age of 96(57.8%) controls and 42(50.6%) cases was 3rd trimester. Most, 156(94.0%) controls and 79(95.2%) cases had no history of home delivery. The majority, 154(92.8%) controls and 66(79.5%) cases had no history of abortion. More than half, 96(57.8%) controls and 31(37.3%) cases had female genital mutilation. Most of, the 161(97.0%) controls and 72(86.7%) cases had no history of sexually transmitted infection. Only 2(1.2%) controls and 3(3.6%) cases were carriers of human immune deficiency virus (HIV). (Table 3).
|
Variables (n=249) |
Category |
Controls (n=166) |
Cases (n=83) |
||
|
Frequency |
Percent |
Frequency |
Percent |
||
|
Gravidity |
Primigravida |
33 |
19.9 |
15 |
18.1 |
|
Multi gravida |
119 |
71.7 |
59 |
71.1 |
|
|
Grand multigravida |
14 |
8.4 |
9 |
10.8 |
|
|
Parity |
Null para |
32 |
19.3 |
16 |
19.3 |
|
Primipara |
54 |
32.5 |
25 |
30.1 |
|
|
Multi para |
74 |
44.6 |
38 |
45.8 |
|
|
Grand multipara |
6 |
3.6 |
4 |
4.8 |
|
|
Gestational age |
1st trimester |
17 |
10.2 |
5 |
6.0 |
|
2nd trimester |
53 |
31.9 |
36 |
43.4 |
|
|
3rd trimester |
96 |
57.8 |
42 |
50.6 |
|
|
History of home delivery |
No |
156 |
94.0 |
79 |
95.2 |
|
Yes |
10 |
6.0 |
4 |
4.8 |
|
|
History of abortion |
No |
154 |
92.8 |
66 |
79.5 |
|
Yes |
12 |
7.2 |
17 |
20.5 |
|
|
Female genital mutilation |
No |
70 |
42.2 |
52 |
62.7 |
|
Yes |
96 |
57.8 |
31 |
37.3 |
|
|
History of sexually transmitted infection |
No |
161 |
97.0 |
72 |
86.7 |
|
Yes |
5 |
3.0 |
11 |
13.3 |
|
|
HIV test result |
Negative |
164 |
98.8 |
80 |
96.4 |
|
Positive |
2 |
1.2 |
3 |
3.6 |
Table 3: Maternity-Related Characteristics of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Medically Related Factors
All controls and 69(83.1%) cases had on history of jaundice. About 77(46.4%) controls and 46(55.4%) cases had a history of health facility admission. Most, 155(93.4%) controls and 80(96.4%) cases had no history of blood transfusion. The majority, 144(86.7%) controls and 68(81.9%) cases had no history of surgical procedure. (Table 4).
|
Variables (n=249) |
Category |
Controls (n=166) |
Cases (n=83) |
||
|
Frequency |
Percent |
Frequency |
Percent |
||
|
History of jaundice |
No |
166 |
100.0 |
69 |
83.1 |
|
Yes |
0 |
0.0 |
14 |
16.9 |
|
|
History of health facility admission |
No |
89 |
53.6 |
37 |
44.6 |
|
Yes |
77 |
46.4 |
46 |
55.4 |
|
|
History of blood transfusion |
No |
155 |
93.4 |
80 |
96.4 |
|
Yes |
11 |
6.6 |
3 |
3.6 |
|
|
History of surgical procedure |
No |
144 |
86.7 |
68 |
81.9 |
|
Yes |
22 |
13.3 |
15 |
18.1 |
|
Table 4: Medical-Related Characteristics of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Traditional Practice-Related Factors
More than half, 143(86.1%) controls and 60(72.3%) cases had no traditional means of dental extraction. The majority, 101(60.8%) controls and 59(71.1%) cases had a history of body or ear piercing. About 120(72.3%) controls and 42(50.6%) cases had no history of tonsillectomy or uvuloctomy. The majority, 162(97.6%) controls and 74(89.2%) cases had no history of contact with a jaundiced person. (Table 5).
|
Variables (n=249) |
Category |
Controls (n=166) |
Cases (n=83) |
||
|
Frequency |
Percent |
Frequency |
Percent |
||
|
Traditional means of dental extraction |
No |
143 |
86.1 |
60 |
72.3 |
|
Yes |
23 |
13.9 |
23 |
27.7 |
|
|
History body or ear piercing |
No |
65 |
39.2 |
24 |
28.9 |
|
Yes |
101 |
60.8 |
59 |
71.1 |
|
|
History tonsillectomy or vulvectomy |
No |
120 |
72.3 |
42 |
50.6 |
|
Yes |
46 |
27.7 |
41 |
49.4 |
|
|
History of contact with a jaundiced person |
No |
162 |
97.6 |
74 |
89.2 |
|
Yes |
4 |
2.4 |
9 |
10.8 |
|
Table 5: Traditional Practice-Related Characteristics of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Personal and Familial Risky Behavior
More than half, 92(55.4%) controls, and 50(60.2%) cases had a history of sharp instrument injury. All study participants reported no history of multiple sexual partners. Only 2(1.3%) controls and 1(1.2%) cases had previous marriage. Also, in 3(1.8%) controls and 2(2.4%) cases, the woman's husband had another wife. (Table 6).
|
Variables (n=249) |
Category |
Controls (n=166) |
Cases (n=83) |
||
|
Frequency |
Percent |
Frequency |
Percent |
||
|
History of sharp instrument injury |
No |
74 |
44.6 |
33 |
39.8 |
|
Yes |
92 |
55.4 |
50 |
60.2 |
|
|
History of multiple sexual partners |
No |
166 |
100.0 |
83 |
100.0 |
|
Yes |
0 |
0.0 |
0 |
0.0 |
|
|
History previous marriage |
No |
164 |
98.8 |
82 |
98.8 |
|
Yes |
2 |
1.2 |
1 |
1.2 |
|
|
The husband had another wife |
No |
163 |
98.2 |
81 |
97.6 |
|
Yes |
3 |
1.8 |
2 |
2.4 |
|
Table 6: Personal and Familial Risky Behavior of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Knowledge of Pregnant Women About HBV
Out of 166 controls, 77(46%) and from 83 cases 10(12.0%) had good knowledge about Hepatitis B virus infection (Figure).
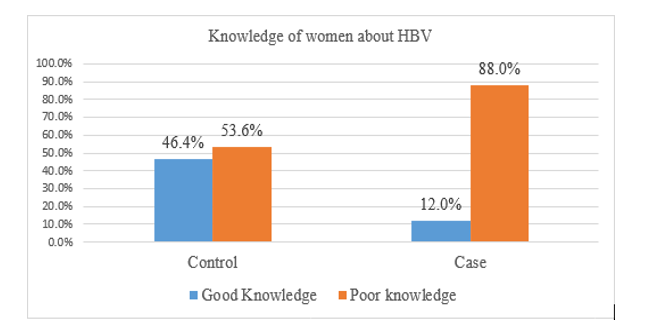
Figure : Knowledge of Women about HBV of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Factors Associated with the HBV
In bivariable logistic regression analysis; residence, knowledge about HBV, history of abortion, history of female genital mutilation, history of sexually transmitted infection, traditional means of dental extraction, history of tonsillectomy or vulvectomy, and history of contact with a jaundice person were statistically associated with HBV. (Table 7). Whereas; in multivariable analysis; residence [AOR 5.74, 95%CI: 1.94-16.95] knowledge about HBV [AOR 0.15, 95%CI: 0.07- 0.34], history of abortion [AOR 4.56, 95%CI: 1.66-12.53], history of female genital mutilation [AOR 5.29, 95%CI: 2.52-11.09], history of sexually transmitted infection [AOR 4.62, 95%CI: 1.26-16.97], and history of contact with a jaundiced person [AOR 6.43, 95%CI: 1.53-26.94] were significantly associated with HBV. (Table 7).
|
Variables (n=249) |
Category |
HBV |
COR (95% CI) |
AOR (95% CI) |
p-value |
|
|
Control(n=166) |
Case(n=83) |
|||||
|
Residence |
Urban |
154(61.9%) |
70(28.1%) |
1 |
1 |
|
|
Rural |
12(4.8%) |
13(5.2%) |
2.38(1.04-5.49) |
5.74(1.94-16.95) |
0.002* |
|
|
Knowledge about HBV |
Poor |
89(35.7%) |
73(29.3%) |
1 |
1 |
|
|
Good |
77(30.9%) |
10(4.1%) |
0.16(0.08-0.33) |
0.15(0.07-0.34) |
0.000* |
|
|
History of abortion |
No |
154(61.9%) |
66(26.5%) |
1 |
1 |
|
|
Yes |
12(4.8%) |
17(6.8%) |
3.31(1.49-7.31) |
4.56(1.66-12.53) |
0.003* |
|
|
History of female genital mutilation |
No |
52(20.9%) |
70(28.1%) |
1 |
1 |
|
|
Yes |
31(12.4%) |
96(38.6%) |
2.30(1.34-3.95) |
5.29(2.52-11.09) |
0.000* |
|
|
History of sexually transmitted infection |
No |
161(64.7%) |
72(28.9%) |
1 |
1 |
|
|
Yes |
5(2.0%) |
11(4.4%) |
4.92(1.65-14.68) |
4.62(1.26-16.97) |
0.021* |
|
|
Traditional means dental extraction |
No |
143(57.4%) |
60(24.1%) |
1 |
1 |
|
|
Yes |
23(9.2%) |
23(9.2%) |
2.38(1.24-4.57) |
1.77(0.75-4.19) |
0.196 |
|
|
History of tonsillectomy or vulvectomy |
No |
120(48.2%) |
42(16.9%) |
1 |
1 |
|
|
Yes |
46(18.5%) |
41(16.4%) |
2.55(1.47-4.41) |
1.91(0.93-3.95) |
0.078 |
|
|
History of contact with a jaundiced person |
No |
162(65.1%) |
74(29.7%) |
1 |
1 |
|
|
Yes |
4(1.6%) |
9(3.6%) |
4.93(1.47-16.51) |
6.43(1.53-26.94) |
0.011* |
|
|
Hint: AOR: Adjusted Odds Ratio; COR: Crude Odds Ratio; HBV: Hepatitis B Virus; *: p-value less than 0.05; 1: reference group |
||||||
Table 7: Bivariable and Multivariable Regression Analysis of HBV of Pregnant Women Attending Antenatal Visit at Comprehensive Specialized Hospital in Central Ethiopia Region, 2023
Discussion
This study revealed that residence was significantly associated with the HBV. Pregnant women who live in rural settings were 5.74 times more likely to acquire the HBV compared to pregnant women who live in urban settings. It was similar to some other studies done in Ethiopia [15-25]. This might be related to the way of living in which the rural women are engaged, the living standard in the rural setting, and less exposure to media about infection prevention. Additionally, in a rural setting, there is cross- contamination due to a lack of knowledge in prevention, and social definition of the diseases.
In this study, knowledge about the HBV was found to be a significant determinant of HBV among pregnant women. Pregnant women who had good knowledge about HBV were 85% less likely to acquire HBV compared to pregnant women who had poor knowledge. The possible explanation for this might be that knowledgeable women might take care of themselves to prevent infection. In addition, the knowledgeable women were aware of the transmission ways and might combat the spread of the infection. Previous studies indicate that the knowledge of HBV in the community was low [18-26,27].
In this study, the history of abortion was identified as a significant determinant of the HBV among pregnant women. Pregnant women who had a history of abortion were 4.56 times more likely to acquire the HBV compared to pregnant women who did not have a history of abortion. It was similar to other studies [13-28]. This might be related to unskilled and/or traditional personnel and the use of unsterile instruments for the procedure.
This study showed that a history of female genital mutilation was found to be a significant determinant of the HBV among pregnant women. Pregnant women who had a history of female genital mutilation were 5.29 times more likely to acquire the HBV compared to pregnant women who did not have a history of female genital mutilation. This might be due shared use of genital mutilating sharp materials and body fluid contamination from the girl at the time and wound healing stages. However, in another study done at Adigrat General Hospital, Northern Ethiopia, a history of surgical and dental procedures was a protective mechanism for acquiring HBV infection [28]. This might be related to following strict sterile techniques to prevent infection transmission during procedures. In addition, it might be due to differences in study design, sample size, and socio-cultural risk behaviors of the study participants.
In this study, a history of sexually transmitted infection was found to be a determinant factor of the HBV among pregnant women. Pregnant women who had a history of sexually transmitted infection were 4.62 times more likely to acquire the HBV compared to pregnant women who did not have a history of sexually transmitted infection. This is obvious that the HBV itself is sexually transmitted. As a result, those pregnant women having sexually transmitted infections were vulnerable to similarly acquiring HBV.
This study showed that a history of contact with a jaundiced person was found to be a significant determinant of the HBV among pregnant women. Pregnant women who had a history of contact with a jaundiced person were 6.43 times more likely to acquire the HBV compared to pregnant women who did not have a history of contact with a jaundiced person. This finding is supported by other studies [18-21,22]. Works of literature indicate that the risk of HBV transmission is high in people who are in contact with chronically infected HBV participants [18-29]. The possible explanation for this might be due to having a wide chance of contact with the body fluids of the chronic carriers. In addition, the transmission of the virus through contact with a jaundiced person is secondary to HBV infection.
However, in another studies, age (10), tattoos, and tonsillectomy were found to be a significant risk factor of HBV among pregnant women, unlike this study [18-21,22]. This might be due to differences in sociodemographic characteristics of women, differences in study design, differences in sample size, and time variation of the studies.
Conclusion
In this study, residence, knowledge about HBV, history of abortion, history of female genital mutilation, history of sexually transmitted infection, and history of contact with a jaundiced person were found to be significant determinants of HBV infection. Therefore, creating awareness about the HBV, practicing safe abortion, avoiding female genital mutilation, preventing sexually transmitted infections, and avoiding unnecessary contact with a jaundiced person may minimize the burden of the HBV.
Limitations of the Study
The chronicity of the virus was not analyzed.
Ethical Consideration
Ethical clearance was obtained from the Wachemo University department of Comprehensive Nursing Ethical Review Committee (CN/ERC/92/15). A letter of permission was obtained from the Medical Directors of the hospital and a permission letter was provided to the maternity and child health case team coordinator.
Informed Consent
Written informed consent was obtained from each participant woman and the information obtained from them would not have been disclosed. Coding was used to eliminate names and other personal identifications of respondents. The respondents` right to refuse, or stop at any time, confidentiality, and the purpose of the information was only for a research was clearly stated. Thoroughly, the research fulfills the required principles of the declaration of the Helsinki General Assembly, Seoul, Korea, and October 2008.
Acknowledgement
We would like to thank the study participants for the scarification of their valuable time spent during the interview.
Authors Contribution
All authors have made substantial contributions to the work. Participated in the conception, design, and acquisition, conducted the data analysis and interpretation; took part in drafting, revising, and critically reviewing the article. All authors gave final approvalof the version to be published and all authors have agreed on the journal to which the article has been submitted; and agreed to be personally accountable for all aspects of the work.
Availability of data
The data used for this study are available on secured and reasonable request.
References
- World Health Organization. Hepatitis B fact sheet (2016).
- WHO. Hepatitis B. 2020, Available at
- World Health Organization. Global health sector strategy on viral hepatitis towards ending viral hepatitis (2016).
- World Health Organization. Global hepatitis report 2017: web annex A: estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2017 (2018).
- Liu, J., Liang, W., Jing, W., & Liu, M. (2019). Countdown to 2030: eliminating hepatitis B disease, China. Bulletin of the World Health Organization, 97(3), 230.
- World Health Organization. (2020). Prevention of mother- to-child transmission of hepatitis B virus (HBV): Guidelines on antiviral prophylaxis in pregnancy. World Health Organization.
- Inoue, T., & Tanaka, Y. (2016). Hepatitis B virus and its sexually transmitted infection-an update. Microbial cell, 3(9), 420.
- Akibu, T. (2018). Formative research for enhancing interventions to prevent violence against women: men’s perceptions in Diepsloot, South Africa (Doctoral dissertation, doctoral dissertation].[Johannesburg]: University of Witwatersrand.
- Kebede, K. M., Abateneh, D. D., & Belay, A. S. (2018). Hepatitis B virus infection among pregnant women in Ethiopia: a systematic review and Meta-analysis of prevalence studies. BMC infectious diseases, 18, 1-9.
- Bayo, P., Ochola, E., Oleo, C., & Mwaka, A. D. (2014). High prevalence of hepatitis B virus infection among pregnant women attending antenatal care: a cross-sectional study in two hospitals in northern Uganda. BMJ open, 4(11), e005889.
- Alter, M. J. (2003). Epidemiology of hepatitis B in Europe and worldwide. Journal of hepatology, 39, 64-69.
- Negesse, Z. A., & Debelo, D. G. (2019). Seroprevalence of hepatitis B surface antigen and associated risk factors among pregnant women in Gandhi Memorial Hospital, Addis Ababa. Journal of Public Health and Epidemiology, 11(6), 123-129.
- Amsalu, A., Ferede, G., Eshetie, S., Tadewos, A., & Assegu,D. (2018). Prevalence, Infectivity, and Associated Risk Factors of Hepatitis B Virus among Pregnant Women in Yirgalem Hospital, Ethiopia: Implication of Screening to Control Motherâ?ÂÂtoâ?ÂÂChild Transmission. Journal of pregnancy, 2018(1), 8435910.
- Chernet, A., Yesuf, A., & Alagaw, A. (2017). Seroprevalence of Hepatitis B virus surface antigen and factors associated among pregnant women in Dawurozone, SNNPR, SouthwestEthiopia: a cross sectional study. BMC research notes, 10, 1-5.
- Yohanes, T., Zerdo, Z., & Chufamo, N. (2016). Seroprevalence and predictors of hepatitis B virus infection among pregnant women attending routine antenatal care in Arba Minch Hospital, South Ethiopia. Hepatitis research and treatment, 2016(1), 9290163.
- Gedefaw, G., Waltengus, F., Akililu, A., & Gelaye, K. (2019). Risk factors associated with hepatitis B virus infection among pregnant women attending antenatal clinic at Felegehiwot referral hospital, Northwest Ethiopia, 2018: an institution based cross sectional study. BMC research notes, 12, 1-7.
- Tanga, A. T., Teshome, M. A., Hiko, D., Fikru, C., & Jilo, G.K. (2019). Sero-prevalence of hepatitis B virus and associated factors among pregnant women in Gambella hospital, South Western Ethiopia: facility based cross-sectional study. BMC infectious diseases, 19, 1-7.
- Umer, A., Teklemariam, Z., Ayele, F., & Mengesha, M. M. (2023). Prevalence of hepatitis B infection and its associated factors among pregnant mothers attending antenatal care at public hospitals at Hararghe, Eastern Ethiopia. Frontiers in Global Women's Health, 4, 1056488.
- Anaedobe, C. G., Fowotade, A., Omoruyi, C. E., & Bakare,R. A. (2015). Prevalence, socio-demographic features and risk factors of Hepatitis B virus infection among pregnant women in Southwestern Nigeria. The Pan African Medical Journal, 20.
- Gedefaw, G., Waltengus, F., Akililu, A., & Gelaye, K. (2019). Risk factors associated with hepatitis B virus infection among pregnant women attending antenatal clinic at Felegehiwot referral hospital, Northwest Ethiopia, 2018: an institution based cross sectional study. BMC research notes, 12, 1-7.
- Bafa, T. A., & Egata, A. D. (2020). Seroepidemiological patterns and predictors of hepatitis B, C and HIV viruses among pregnant women attending antenatal care clinic of Atat Hospital, Southern Ethiopia. SAGE Open Medicine, 8, 2050312119900870.
- Asaye, Z., Aferu, T., Asefa, A., Feyissa, D., Regasa, T.,Kebede, O., ... & Feyisa, M. (2021). Prevalence of hepatitis B virus among pregnant women on antenatal care follow-up at Mizan-Tepi university teaching hospital and Mizan Health Center, southwest Ethiopia. International Journal of General Medicine, 195-200.
- Negesse, Z. A., & Debelo, D. G. (2019). Seroprevalence of hepatitis B surface antigen and associated risk factors among pregnant women in Gandhi Memorial Hospital, Addis Ababa. Journal of Public Health and Epidemiology, 11(6), 123-129.
- Chernet, A., Yesuf, A., & Alagaw, A. (2017). Seroprevalence of Hepatitis B virus surface antigen and factors associated among pregnant women in Dawuro zone, SNNPR, Southwest Ethiopia: a cross sectional study. BMC research notes, 10, 1-5.
- Metaferia, Y., Dessie, W., Ali, I., & Amsalu, A. (2016). Seroprevalence and associated risk factors of hepatitis B virus among pregnant women in southern Ethiopia: a hospital-based cross-sectional study. Epidemiology and health, 38.
- Shiferaw, F., Letebo, M., & Bane, A. (2016). Chronic viral hepatitis: policy, regulation, and strategies for its control and elimination in Ethiopia. BMC Public Health, 16, 1-13.
- Frambo, A. A. B., Atashili, J., Fon, P. N., & Ndumbe, P. M. (2014). Prevalence of HBsAg and knowledge about hepatitis B in pregnancy in the Buea Health District, Cameroon: a cross-sectional study. BMC research notes, 7, 1-7.
- Kinfe, H., Sendo, E. G., & Gebremedhin, K. B. (2021). Prevalence of hepatitis B virus infection and factors associated with hepatitis B virus infection among pregnant women presented to antenatal care clinics at Adigrat General Hospital in Northern Ethiopia. International Journal of Women's Health, 119-127.
- Fomulu, N. J., Morfaw, F. L., Torimiro, J. N., Nana, P., Koh,M. V., & William, T. (2013). Prevalence, correlates and pattern of Hepatitis B among antenatal clinic attenders in Yaounde- Cameroon: is perinatal transmission of HBV neglected in Cameroon?. BMC pregnancy and childbirth, 13, 1-10.