
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2022) Volume 7, Issue 3
Determinants and Efficacy of Herbal Medicine Use among Pregnant Women in the Asante Akim North District, Ghana
2Wesley Girls High School, P.O. Box KS8481, Kumasi, Ghana
Received Date: Sep 14, 2022 / Accepted Date: Sep 21, 2022 / Published Date: Sep 28, 2022
Copyright: ©Buor Daniel, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Buor Daniel, Awuku Paul. (2022). Determinants and efficacy of Herbal Medicine Use among pregnant women in the Asante Akim North District, Ghana. Int J Women's Health Care, 7(3), 140-148.
Abstract
The use of herbal medicine is gaining roots in Africa and research works on the theme have attracted attention. In Ghana, research on the theme is limited so needs further interrogation in order to come out with conclusions for an appropriate policy direction to improve its use and efficacy. The study examines the determinants of herbal medicine use by pregnant women in a predominantly rural district in Ghana. It was underpinned by the theory of planned behaviour and a conceptual framework based on the Andersen behavioural framework on use of health services. The cross-sectional design, mixed method approach as well as questionnaire and interview guide instruments were the methodological tools used to gather information for the study whilst descriptive and non-parametric statistical tools were used for data analysis. Results show that the prevalence rate of the use of herbal medicine by pregnant women is quite high and income and religion are the main predictors of its use; and that Moslem pregnant women use it more regularly than their Christian counterparts. Health problems herbal medicine addresses are anaemia, waist pains, nausea, long duration of labour, cold and malaria; and the herbs regularly used are ginger, lemon, neem, mahogany, dandelion, Aloe vera and tea leaves (Camellia sinensis). It was also observed that reasons for the regular use of herbal medicine by pregnant women, among other factors, are that it is rooted in their culture and for its efficacy. The conceptual framework which hinged on Andersen behavioural model and the theory of planned behaviour have reflected in the findings. It is recommended that government encourage the use of herbal medicine through promotion and making it safe and that the World Health Organisation (WHO) must carry out research on the safety and efficacy of herbal medicine to ensure its safe use and effectiveness.
Keywords
Herbal Medicine, Pregnant Women, Andersen Behavioural Model, Cross-Sectional Design, Ghana
Introduction
The use of plant medicine is widespread, especially in develop¬ing countries. A study by [1] has revealed the increased percent¬age (about 80%) of people who use herbal medicine to meet their health care needs in Africa. Studies by [2,3] reveal similar results. Plant medicines are affordable, thus, in the face of increasing or-thodox health care costs, indigenous practices become appealing to people [4]. There are many known benefits associated with herbal medicines that can help during or after pregnancy. Some other advantages are low cost, affordability, availability, accept-ability and low toxicity [5].
In most rural settings, pregnant women consider plant medicine as a cure-all remedy in the face of any health challenge [6]. Thus, the popularity of herbal medicine among pregnant women is attributed to the common belief that herbs are natural and free of any adverse effects that are usually associated with conventional drugs and can also be obtained without prescription [7,8,4]. Thus, in the early stages of pregnancy, women are advised to use some tested and proven herbs to prevent unforeseen events [9,10].
A successful use of herbal medicine by pregnant women would help fulfil the UN sustainable development goal 3, “Good health and wellbeing” and universal health coverage [11]. Maternal deaths are a serious health problem especially in sub-Saharan Af¬rica where maternal health services coverage is very limited. A research into access and efficacy of herbal medicine by pregnant women would provide a basis for developing policies to improve the quality of herbal medicine hence, serve as a complement to or-thodox health care to expand universal health coverage. Globally, and especially in developing countries, pregnant women usually perceive herbal products as a safe, natural alternative to conven¬tional drugs [12], a perception which could be dangerous in the administration of health care.
In Ghana and some other developing countries, data and studies on herbal medicine usage amongst pregnant women are scanty [13]. Conducted research titled ‘We are nothing without herbs’: a story of herbal remedies’ use during pregnancy in rural Ghana at Birim South District. In another study by on herbal medicine usage be¬fore and during pregnancy in Tamale, unemployment was reported to have been the only factor that accounted for a significant in¬crease in herbal medicine use among participants [14]. Since 1992, the Ghana Food and Drugs Law has been in existence to regulate herbal medicines as well as conventional medicines in the country [15].
This study, therefore, sought to investigate the regularity of use of herbs and the parameters that influence their use among preg-nant women in the Asante Akim North District where there is no evidence of such research having been undertaken. The findings are related to similar findings in other developing countries to es-tablish the basis for common policies to be recommended by the WHO for adoption by developing countries to improve maternal health care. This will fulfil the UN Strategic Development Goal (SDG) 3 and to ensure universal health coverage.
The null hypotheses which were tested in this study are as follows
1. HO= There is no statistically significant difference in the use of herbal medicine by the level of education of pregnant women.
2. HO = There is no statistically significant difference between rural and urban areas in the use of herbal medicine
Thereotical Framework
Several theories can be used to explain the utilization of herbal medicine among pregnant women. To understand how personal health beliefs and behaviour impact utilization of herbal medicine, theory of planned behaviour was adopted to guide the study [16]. The Theory of Planned Behaviour establishes a connection be¬tween one’s perception and behaviour [16]. The theory of reasoned action was in turn included in the theory of planned behaviour. Per the content of the theory of reasoned action, if people review the recommended behaviour as positive (attitude), person’s beliefs about the particular behaviour, which is inspired by the comment of others such as friends, parents, spouse, it results in a higher in¬tent (motivation) and they are more probable to use it.
Conceptual Framework
The conceptual framework for the study is the Andersen health¬care utilization model [17]. The purpose of the framework is to discover the conditions that either facilitate or impede the utili¬zation of herbal medicine among pregnant women. The Andersen healthcare utilization model is a conceptual framework that tar¬gets the demonstration of parameters that lead to the utilization of health services [17]. According to the model, the use of health ser¬vices (including physician visits, inpatient care, dental care, etc.) is assessed via three (3) dynamics; predisposing factors, enabling factors, and need.
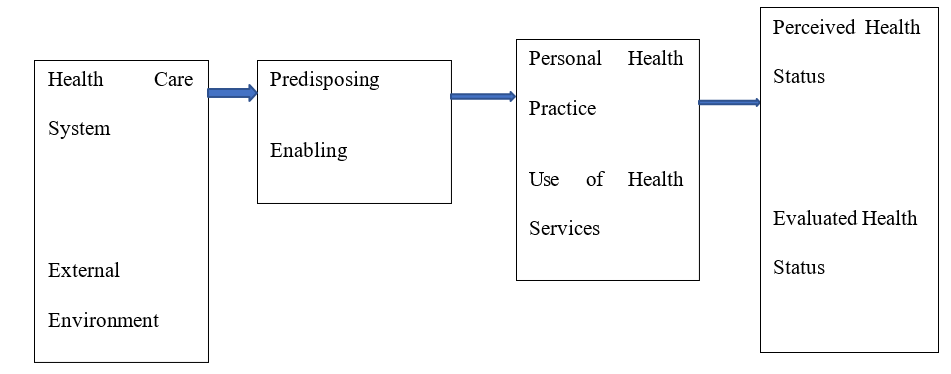
Figure 1: Andersen Healthcare Utilization Model
Environment Population Health Outcomes Characteristics Behaviour Source: [17]
The adapted model has the use of herbal medicine at the centre, being the dependent (outcome) variable. Influencing the use of herbal medicine, and showing a relationship with it are the pre-disposing characteristics, enabling resources, need factors; spatial setting (rural-urban), and reasons for utilization; efficacy, accessi¬bility, affordability, and cultural acceptability. Predisposing char- acteristics include the sex, occupation, and level of education of the patient; enabling resources include basically income and NHIS cardholding. Also, the spatial setting includes rural and urban set¬tings. Moreover, herbal medicine use depends on its efficacy, ac¬cessibility, affordability, and cultural acceptability.
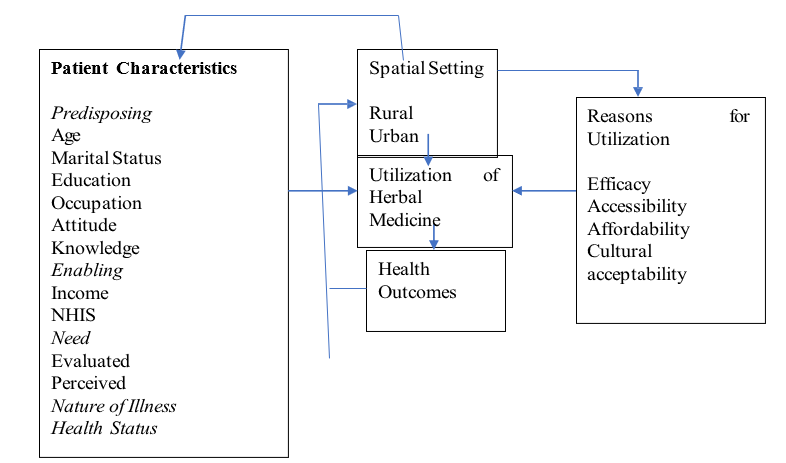
Figure 2: Modified Andersen model on utilization of herbal medicine
Profile, Design and Approach
The population of Asante Akim North District (Figure 3) as of 2010 was 68,186 . Out of these, 33,275 (48.8%) were males and 34,911 (51.2%) females [18]. About 53.5 percent of the population are rural whiles 46.5 percent are urban. Pregnant women making four visits to the antenatal clinic were 71.6% (2.042) in 2015 as against 109.3% (3,311) in 2014 [19].

Figure 3: Map of Asante Akim North District
Source: [18,20]
This study adopted a cross-sectional study design. The study utilized a mixed-method approach to achieve its purpose. The mixed-method approach of a study is when a researcher adopts both quantitative and qualitative means of assessment to arrive at the aim of a study [21].
Sampling, Data Collection and Analysis
The study adopted a convenient sampling technique to select preg-nant women for the study. The convenient sampling technique in¬volves the selection of participants based on their ready availabil¬ity and convenience. The sample size of the study was estimated using Cochran’s formula and the rate of herbal medication in Gha¬na (7%) as reported by [13, 22]. The sample size was calculated as follows:
n =z2pq/e2
where: n= sample size,
z= critical value of 1.96 at a 95% confidence interval,
p= prevalence of herbal medication (7%), and e = margin of error, (0.05).
Hence, the sample size (n) is approximately 100. Moreover, 15% of the determined figure was added to cater for the non-response rate of the questionnaires. Therefore, the study sampled a total of 115 respondents.
The study focused on five communities within the Asante Akim North District. These include Agogo, Ananekrom, Juansa, Akutu¬ase, and Domeabra (Table 1). The respective sample size (S) allo¬cation by the selected communities was determined by the propor¬tionate sampling method [given by S = (b/100)115]. The selection of settlements was done purposively; taking into consideration the availability of a health facility, population, and physical accessi¬bility to a health institution. Included in the community sample were pregnant women of any age. Three respondents from each community were randomly selected for in-depth interview.
Table 1: Sample Size Determination for the Communities
|
COMMUNITY |
POPULATION |
PERCENTAGE (b) |
SAMPLE SIZE(S) |
|
Agogo |
32,196 |
71 |
80 |
|
Domeabra |
4,770 |
10 |
12 |
|
Juansa |
4,472 |
10 |
12 |
|
Akutuase |
2,217 |
5 |
6 |
|
Ananekrom |
1,992 |
4 |
5 |
|
TOTALS |
45,647 |
100 |
115 |
Source: [18].
Both primary and secondary data were used. Primary data were used through the use of structured questionnaire whilst interview guides were used for the collection of data from key stakehold¬ers including midwives, traditional birth attendants, herbalists and three respondents from each of the study communities. The main components of the questionnaire were the prevalence of herb¬al medicine use among pregnant women, determinants of herbal medicine use among pregnant women and the efficacy of herbal medicine use. During the days for antenatal services for all preg¬nant women in the selected health facilities, the researcher visited them, explained the purpose of the study and sought their volun¬tary consent to participate. Consent forms were signed by the liter¬ate whilst the illiterate thumb printed. The research reported in this manuscript has been approved by the Humanities and Social Sci¬ences Research Ethics Committee (Ref: HuSSREC/AP/31/Vol.1) of the Kwame Nkrumah University of Science and Technology (KNUST), Kumasi-Ghana.
Data were analysed using descriptive and non-parametric statisti¬cal tools such as frequencies, percentages, and the chi-square test of independence. Chi-square test of independence was applied to identify whether there were significant differences by place of res¬idence (rural and urban) and level of education in the use of herbal medicine by pregnant women. Pretesting of data collection tools was carried out in a community in the Asante Akim South District to ensure the reliability of the study. Minor changes were made after the pretesting of the instrument.
Results
Socio-demographic Characteristics of Respondents The socio-demographic characteristics of the respondents are in-dicated in Table 2
Table 2: Socio-demographic characteristics of respondents
|
Variable |
Frequency |
Per cent |
|
Age |
||
|
16-20 |
13 |
11.3 |
|
21-25 |
28 |
24.3 |
|
26-30 |
25 |
21.7 |
|
31-36 |
31 |
27 |
|
37+ |
18 |
15.7 |
|
Total |
115 |
100.0 |
|
Income Per Month |
||
|
<100 |
60 |
52.2 |
|
100-300 |
37 |
32.2 |
|
301-500 |
10 |
8.7 |
|
501-700 |
1 |
0.9 |
|
700+ |
7 |
6.1 |
|
Occupation |
||
|
Trading |
42 |
36.5 |
|
Farming |
36 |
31.3 |
|
Teaching |
8 |
7 |
|
Nursing |
3 |
2.6 |
|
Students |
1 |
0.9 |
|
Unemployed |
25 |
21.7 |
|
Marital Status |
||
|
Married |
51 |
44.4 |
|
Never Married |
25 |
21.7 |
|
Cohabiting |
38 |
33 |
|
Divorced |
1 |
0.9 |
|
Education |
||
|
No Formal Education |
8 |
7 |
|
Primary |
18 |
15.7 |
|
Junior High School |
60 |
52.2 |
|
Senior |
19 |
16.5 |
|
Tertiary High School |
10 |
8.7 |
|
Religion |
||
|
Christianity |
82 |
71.3 |
|
Islam |
29 |
25.2 |
|
Traditional |
4 |
3.5 |
|
Residence |
||
|
Urban |
13 |
11.3 |
|
Rural |
102 |
88.7 |
|
Family Size |
||
|
Non-Response |
12 |
10.4 |
|
1-5 |
51 |
44.3 |
|
6-10 |
40 |
34.8 |
|
>10 |
12 |
10.4 |
Source: Field Work, 2020
A greater proportion of the respondents were aged between 21 and 36 which is within the age of maturity whilst majority earned very low incomes. Traders and farmers dominated whilst workers in formal employment who earned regular monthly incomes were very few. The married dominated whilst those with basic educa¬tion constituted 67%. Those with Christian religion and also living in the rural sector constituted a significant proportion of the re¬spondents, with large families dominating.
Prevalence of herbal medicine use among pregnant women
The analysis revealed that approximately sixty-two percent (61.7%) of the women use herbal medicine at least once a week whilst 6.9% use it when necessary (Table 3). The diseases that attract the use of health services more regularly are waist pains, shortening of long duration of labour, miscarriage, nausea/vomit-ing, cold, malaria and anaemia. Field work showed that the herbs pregnant women use most are ginger and lemon (for waist pains, abdominal pains, malaria, and shortening of duration of labour); neem leaves (for nausea/vomiting, malaria and shortening of du-ration of labour); mahogany (for waist pains and malaria); dande- lion (malaria and nausea/vomiting); tea leaves (Camellia sinensis for anaemia) and Aloe vera for skin disease and worm infestation. Medication for miscarriage is sold by the herbal practitioners.
In an in-depth interview, a respondent who use herbs regularly re¬sponded to a question on regularity of use of herbal medicine as follows:
I use it when I started experiencing abdominal pains during my pregnancy; I used herbs until I gave birth. For me, I started expe¬riencing abdominal and waist pains in the early stage of the preg¬nancy, which led me to use herbs (Pregnant Woman; Agogo).
A health worker responded that their regularity of use of herbal medicine is a practice emerging from culture. She narrated as fol¬lows:
One way or the other, they are being forced by the older generation to use it. Even though some feel uncomfortable when they use herbs in pregnancy, because they were forced to use it during their earlier pregnancies, it just feels right to use it every time (Midwife, Juansa Health Center)
Table 3: Prevalence of herbal medicine use among pregnant women
|
Period |
Frequency (n=71) |
Rate (61.7%) |
|
Once a week |
41 |
35.65 |
|
Once in two weeks |
6 |
1.74 |
|
Once in three weeks |
15 |
13.04 |
|
Once in a month |
1 |
0.87 |
|
When needed/necessary. |
8 |
6.96 |
Source: Field Survey, 2020
Socio-demographic Determinants of Herbal Medicine Use
Scio-demographic factors determining herbal medicine use are income (p=0.014) and religion (p=0.045) (Table 4). Respondents with low oncomes will tend to use herbal medicine more than those with high incomes. There are however some deviations from this model more likely due to other factors such as religion as depicted by the results. Respondents who are Muslims and Traditionalists utilise health services more than Christians.
Table 4: Socio-demographic Determinants of Herbal Medicine Use in Pregnancy
|
Variables |
Sub-Variables |
Usersn=95 (82.6%) |
Non-Usersn=16 (13.9%) |
Can’t re-calln=4 (3.5%) |
Total N=115 (100%) |
Chi-Square/ (p-value) |
|
Marital status |
Married |
45 (88.2) |
4 (7.8) |
2 (3.9) |
51 (100.0) |
X =13.373a 2 P = 0.158 |
|
Cohabitation |
33 (86.8) |
5 (13.2) |
0 (0.0) |
38 (100.0) |
||
|
Never Married |
16 (64.0) |
7 (28.0) |
2 (8.0) |
25 (100.0) |
||
|
Divorced |
1 (100.0) |
0 (0.0) |
0 (0.0) |
1 (100.0) |
||
|
Age |
16-20yrs |
9 (69.2) |
3 (23.1) |
1 (7.7) |
13 (100.0) |
X =20.868a 2 p = 0.643 |
|
21-25yrs |
22 (78.6) |
5 (17.8) |
1 (3.6) |
28 (100.0) |
||
|
26-30yrs |
20 (80.0) |
4 (16.0) |
1 (4.0) |
25 (100.0) |
||
|
31-36yrs |
26 (83.9) |
4 (12.9) |
1 (3.2) |
31 (100.0) |
||
|
37 and above |
18 (100.0) |
0 (0.0) |
0 (0.0) |
18 (100.0) |
||
|
Occupation |
Teaching |
4 (50.0) |
3 (37.5) |
1 (12.5) |
8 (100.0) |
X = 26.554a 2 p = 0.220 |
|
Nursing |
1 (100.0) |
0 (0.0) |
0 (0.0) |
1 (100.0) |
|
|
Trading |
38 (90.5) |
3 (7.1) |
1 (2.4) |
42 (100.0) |
|
|
Farming |
31 (86.1) |
5 (13.9) |
0 (0.0) |
36 (100.0) |
||
|
Student |
2 (66.7) |
1 (33.3) |
0 (0.0) |
3 (100.0) |
||
|
Unemployed |
19 (76.0) |
4 (16.0) |
2 (8.0) |
25 (100.0) |
||
|
Monthly income (GHC) |
<100 |
46 (76.7) |
12 (20.0) |
2 (3.3) |
60 (100.0) |
X = 41.601a 2 p = 0.014* |
|
|
|
|
|
|
||
|
100 - 300 |
37 (100.0) |
0 (0.0) |
0 (0.0) |
37 (100.0) |
||
|
301 - 500 |
8 (80.0) |
1 (10.0) |
1 (10.0) |
10 (100.0) |
||
|
701 - 900 |
1 (100.0) |
0 (0.0) |
0 (0.0) |
1 (100.0) |
||
|
>900 |
3 (42.9) |
3 (42.9) |
1 (14.2) |
7 (100.0) |
||
|
Education |
No formal Edu. |
7 (87.5) |
1 (12.5) |
0 (0.0) |
8 (100.0) |
X = 13.738a 2 p = 0.777 |
|
Primary Edu. |
16 (88.9) |
2 (11.1) |
0 (0.0) |
18 (100.0) |
||
|
JHS |
50 (83.3) |
7 (11.7) |
3 (5.0) |
60 (100.0) |
||
|
SHS |
15 (78.9) |
4 (21.1) |
0 (0.0) |
19 (100.0) |
||
|
Tertiary |
7 (70.0) |
2 20.0) |
1 (10.0) |
10 (100.0) |
||
|
Religion |
Christianity |
62 (75.6) |
16 (19.5) |
4 (4.9) |
82 (100.0) |
X = 9.422a 2 p = 0.045* |
|
Islam |
29 (100.0) |
0 (0.0) |
0 (0.0) |
29 (100.0) |
||
|
Traditional |
4 (100.0) |
0 (0.0) |
0 (0.0) |
4 (100.0) |
||
|
Residence |
Urban |
10 (76.9) |
3 (23.1) |
0 (0.0) |
13 (100.0) |
X = 1.284a 2 p = 0.484 |
|
Rural |
85 (83.3) |
13 (12.7) |
4 (4.0) |
102 (100.0) |
||
|
Family size |
None |
9 (75.0) |
2 (16.7) |
1 (8.3) |
12 (100.0) |
X = 15.622a 2 p = 0.817 |
|
1-5 |
43 (84.3) |
6 (11.8) |
2 (3.9) |
51 (100.0) |
|
|
|
6-10 |
34 (85.0) |
5 (12.5) |
1 (2.5) |
40 (100.0) |
|
|
|
Above 10 |
9 (75.0) |
3 (25.0) |
0 (0.0) |
12 (100.0) |
|
Source: Field Survey, 2020* indicates significant at P < 0.05 significance level.
Efficacy of Herbal Medicine
Respondents responded to the question of efficacy of herbal med¬icine as follows: Herbal medicine is helpful when one has low blood during preg-nancy. I know of one herbal medicine that gives a lot of blood. Anytime am told I have less blood, after taking this particular herbal medicine, I get more blood (Pregnant woman, Juansa).
Herbal medicine is good for managing miscarriages. I also pre-scribe herbs for those having difficulty with delivery. I am not a birth attendant though, but the herbs I prescribe enhances easy and safe delivery. I prescribe herbs for headaches as well. I do these at no charge (Herbalist, Wioso).
The efficacy of herbal medicine was confirmed by both a herbalist who observed that herbal medicine addresses miscarriage and a study participants who also observed that herbal medicine is an antidote for anaemia. These are indicated in the quotes below: Herbal medicine is good for managing miscarriages. I also pre-scribe herbs for those having difficulty with delivery. I am not a birth attendant though, but the herbs I prescribe enhances easy and safe delivery. I prescribe herbs for headaches as well. I do these at no charge (Herbalist, Wioso).
Herbal medicine is helpful when one has low blood during preg¬nancy. I know of one herbal medicine that gives a lot of blood. Anytime am told I have less blood, after taking this particular herbal medicine, I get more blood” (Pregnant woman, Juansa). There was an instance where my blood level was around 9 but upon drinking ‘Jehovafo mojaduro’ for morning and evening, within 4 days, my blood level rose to 12” (Pregnant woman, Akutuase).
Discussion
This study showed that there is a high prevalence of the use of herbal medicine by pregnant women in a predominantly rural dis¬trict in Ghana. The health problems for which the herbs are taken are anaemia, miscarriage, shortening of labour period, malaria, nausea, cold and waist pains. Some of these findings are affirmed by [23]. In a study of herbal medicine use among pregnant women attending antenatal clinics in Lusaka, Zambia observed that lem¬on for nausea/vomiting, ginger for cold, nausea and vomiting and Aloe vera for skin care were the common herbal medicines used and users were willing to use them in the future for their effica¬cy. Some of the main reasons for the regularity of use of herbal medicine as reported in the Lusaka study were safety and com-plementation with conventional medicine hence, confirming its efficacy. In another study by on prevalence of herbal medicine use and associated factor among pregnant women attending antenatal care at public facilities in Southern Ethiopia similar results were observed [24]. In the current study, one of the main reasons for the regularity of use of herbal medicine by pregnant women is that they are culturally used to it. The use has been passed on to them by their parents and grandparents. Besides, they have observed the efficacy of some herbal medicines. The Socio-demographic fac¬tors that predicted the use of herbal medicine by pregnant women were income and religion. Pregnant women with low incomes are more likely to use herbal medicine than those with high incomes. This corresponds with the studies by [10,25,26] which affirmed that pregnant women who had low income were more likely to use herbal medicines. Religion emerged as a factor in the use of herbal medicine by pregnant women. Observed in a study that Muslim women are more likely to use herbal medicine more than Chris¬tian women and the same will go for them when they are preg¬nant [27]. The two null hypotheses: that there is no statistically significant difference between education and the use of herbal by pregnant women and that there is no statistically significant dif¬ference between the use of herbal medicine by place of residence (rural and urban) could not be rejected. The conceptual framework was partially vindicated. Some predisposing factors have informed the use of herbal medicine with favourable outcomes. Besides, the theory of planned behaviour has been justified in the sense that the participants use herbal medicines upon the belief that they would be efficacious. The study has several limitations. Firstly, the study coverage was limited. There should have been several district communities to serve as a basis for comparison and generalisa¬tion. Nevertheless, the use of the current district has provided a blueprint for other studies to be undertaken. Secondly, the sample size for a district of over 60,000 residents was not large enough for the study. The methods used for the sampling procedures however make it representative enough to give credibility to the results.
Conclusion
The findings of this study and related studies bring to the fore is-sues for both national and international policy direction especial-ly in Africa and the developing world. First, pregnant women in several areas in the Africa and the developing world affirm the efficacy of herbal medicine and use it regularly. Second users are confident in the safety. In the light of this, national governments and the World Health Organisation (WHO) must carry out preclin-ical and clinical studies to assess the efficacy and toxicity of herbal medicine. The notion held by the indigenes that herbal medicine could be complementary to conventional medicine is without a ba-sis so its regular use could be dangerous. Since the use of herbal medicine is rooted in the culture of the people, is readily available and affordable, if its safety is ensured through research it could help achieve the goal of universal health coverage and partially fulfil the 3rd SDG.
Acknowledgements
We acknowledge the role played by the participants who guaran-teed information to make the study a success.
References
- Bakato, O., Ansong, J. (2019) Traditional healers broadenhealth care in Ghana, WHO Africa, WHO.
- Ozioma, E. O. J., & Chinwe, O. A. N. (2019). Herbal medicines in African traditional medicine. Herbal medicine, 10, 191-214.
- Barnes, L. A. J., Barclay, L., McCaffery, K., & Aslani, P. (2018). Complementary medicine products used in pregnancy and lactation and an examination of the information sources accessed pertaining to maternal health literacy: a systematic review of qualitative studies. BMC complementary and alternative medicine, 18(1), 1-27.
- Vandana Parmar, D. A. (2005). HERBAL MEDICINES: ITS TOXIC EFFECTS AND DRUG INTERACTIONS.
- Frawley, J., Adams, J., Steel, A., Broom, A., Gallois, C., & Sibbritt, D. (2015). Women’s use and self-prescription of herbal medicine during pregnancy: an examination of 1,835 pregnant women. Women’s Health Issues, 25(4), 396-402.
- Mahomoodally, M. F. (2013). Traditional medicines in Africa: an appraisal of ten potent African medicinal plants. Evidence-Based Complementary and Alternative Medicine, 2013.
- Nergard, C. S., Ho, T. P. T., Diallo, D., Ballo, N., Paulsen,B. S., & Nordeng, H. (2015). Attitudes and use of medicinal plants during pregnancy among women at health care centers in three regions of Mali, West-Africa. Journal of ethnobiology and ethnomedicine, 11(1), 1-11.
- Agyei-Baffour, P., Kudolo, A., Quansah, D. Y., & Boateng, D. (2017). Integrating herbal medicine into mainstream healthcare in Ghana: clients’ acceptability, perceptions and disclosure of use. BMC complementary and alternative medicine, 17(1), 1-9.
- Peprah, P., Agyemang-Duah, W., Arthur-Holmes, F., Budu, H. I., Abalo, E. M., Okwei, R., & Nyonyo, J. (2019). ‘We are nothing without herbs’: a story of herbal remedies use during pregnancy in rural Ghana. BMC complementary and alternative medicine, 19(1), 1-12.
- UN, 2015. Sustainable Development Goals, UN Resolution 70/1. New York.
- Adusi-Poku, Y., Vanotoo, L., Detoh, E. K., Oduro, J., Nsiah,R. B., & Natogmah, A. Z. (2015). Type of herbal medicines utilized by pregnant women attending ante-natal clinic in Of-finso north district: Are orthodox prescribers aware?. Ghana Medical Journal, 49(4), 227-232.
- Frawley, J., Adams, J., Steel, A., Broom, A., Gallois, C., & Sibbritt, D. (2015). Women’s use and self-prescription of herbal medicine during pregnancy: an examination of 1,835 pregnant women. Women’s Health Issues, 25(4), 396-402.
- Ameade, E. P. K., Ibrahim, M., Ibrahim, H. S., Habib, R. H., & Gbedema, S. Y. (2018). Concurrent use of herbal and orthodox medicines among residents of Tamale, Northern Ghana, who patronize hospitals and herbal clinics. Evidence-Based Complementary and Alternative Medicine, 2018.
- Republic of Ghana, Ghana Food and Drugs Act, 1992. PND-CL 305B, Accra. 1992.
- Ajzen, I. (1991). The theory of planned behaviour. Organizational Behaviour and Human Decision Processes, 50 (2), 179-211.
- Andersen, R. M. (1995). Revisiting the behavioral model and access to medical care: does it matter?. Journal of health and social behavior, 1-10.
- Ghana Statistical Service (GSS), 2010 Population and Housing Census, 2012, GSS, Accra
- Ghana Health Service (GHS), Maternal Health, GHS-Family Health Division Annual Report, Accra. 2015.
- GSS. 2010 Population and Housing Census: District Analyt-ical Report, Asante Akim North District. 2014. GSS, Accra.
- Creswell, J. W. Research Design: Qualitative, Quantitative and Mixed Method Approaches (4th Eds) California, USA, SAGE Publications, 2014.
- Kotrlik, J. W. K. J. W., & Higgins, C. C. H. C. C. (2001).Organizational research: Determining appropriate sample size in survey research appropriate sample size in survey research. Information technology, learning, and performance journal, 19(1), 43.
- El Hajj, M., Sitali, D. C., Vwalika, B., & Holst, L. (2020). Herbal medicine use among pregnant women attending antenatal clinics in Lusaka Province, Zambia: A cross-sectional, multicentre study. Complementary Therapies in Clinical Practice, 40, 101218.
- Laelago, T., Yohannes, T., & Lemango, F. (2016). Prevalence of herbal medicine use and associated factors among pregnant women attending antenatal care at public health facilities in Hossana Town, Southern Ethiopia: facility based cross sectional study. Archives of Public Health, 74(1), 1-8.
- Laelago, T. (2018). Herbal medicine use during pregnancy:benefits and untoward effects. Herbal medicine.
- James, P. B., Taidy-Leigh, L., Bah, A. J., Kanu, J. S., Kangbai,J. B., & Sevalie, S. (2018). Prevalence and correlates of herbal medicine use among women seeking Care for Infertility in Freetown, Sierra Leone. Evidence-Based Complementary and Alternative Medicine, 2018.
- James, P. B., Bah, A. J., Tommy, M. S., Wardle, J., & Steel, A. (2018). Herbal medicines use during pregnancy in Sierra Leone: an exploratory cross-sectional study. Women and Birth, 31(5), e302-e309.