
Journal of Depression Anxiety Science(JDAS)

Research Article - (2025) Volume 2, Issue 1
Depression Among HIV-Positive Individuals Attending the Antiretroviral Treatment Clinics of Wolaita Zone, Southern Ethiopia.
2Wolaita Sodo University, College of Medicine and Health Sciences, School of Public Health, Ethiopia
3Wolaita Sodo University, College of Medicine and, Ethiopia
Received Date: Aug 07, 2025 / Accepted Date: Jan 08, 2025 / Published Date: Aug 12, 2025
Copyright: ©©2025 Yohannes Yaya Uka, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Arba, A., Awoke, N., Teshome, M., Lolaso, T., Paulos, K., et al. (2025). Depression Among HIV-Positive Individuals Attending the Antiretroviral Treatment Clinics of Wolaita Zone, Southern Ethiopia. J Dep Anxiety Sci, 2(1), 01-11.
Abstract
Introduction: People who are infected with HIV are more likely to develop depression than the general population. It is one of the causes of poor adherence to Anti-retroviral therapy and worsens the patient’s condition and leads to death. Most studies conducted in the area addressed a single setting whereas this study was multi-central. So, it is important to assess the prevalence of depression and its determinants among HIV-positive individuals attending ART clinics of Wolaita Zone.
Objective: This study aimed to assess the prevalence and determinants of depression among HIV-positive individuals attending ART clinics in Wolaita Zone, Ethiopia.
Methods and Materials: Institution-based cross-sectional study was conducted among HIV-positive individuals attending ART clinics of Wolaita Zone. Data was collected from 596 participants. Health facilities were clustered based on the number of patients attending to ART clinics. Then, facilities were selected randomly from the respective clusters. Data was collected through the face-to-face interview. Epi data for data entry and analyzed using SPSS’s version 20. The presence and strength of association were declared when p-value < 0.05 and using AOR in multivariate analysis respectively.
Result: The prevalence of depression among HIV-positive individuals in the Wolaita Zone is 32.6% at 95% CI [29%, 36%]. Marital status, educational status, living with families, family history of depression, place of medical follow- up, presence of Tuberculosis co-infection, and presence of sleep problems are significantly associated with depression among study participants.
Conclusion and recommendation: The prevalence of depression among HIV-positive individuals in the Wolaita Zone is high. Being single, living far away from family members, having a family history of depression, the presence of sleep problems and TB co-infection, and making medical follow up at governmental facilities are determined to be factors associated with the occurrence of depression among HIV-positive individuals attending ART clinics of Wolaita Zone. Therefore, psychological support with differential counseling of patients on ART based on their specific needs is essential to minimize the occurrence of depression. In addition, early screening and treatment of TB co-infection, and depression are very important.
Keywords
Depression, Depressive Disorders, HIV Patients, Patients on ARTIntroduction
Background
The hallmarks of depression, a common mental condition, include dark mood, lack of interest or pleasure, diminished energy, guilt or feelings of feeling worthless, sleep disruptions or food, and troubles concentration [1]. Everyone can be unhappy and depressed, but when such adverse feelings continue to rule daily life and lead to bodily and mental decline, they are known to as depressive disorders [2].
Human immune deficiency virus, HIV/AIDS, is a cause of death and disability, especially in low- and middle-income countries [3]. Over 25.5 million people suffer with the virus in Sub-Saharan Africa, making this part of Africa the most impacted in the world [4]. Data from Ethiopian Federal HIV/AIDS Prevention and Control Office (EFHAPCO) indicates that there are over 718,550 people (a little over 1.18% of the population) living with HIV in Ethiopia alone [5]. People living with HIV (PLWHA) now have greater access to highly effective antiretroviral therapy (ART), which has lengthened survival and slowed the advancement of the HIV disease, bringing issues with quality of life, particularly their mental wellbeing, at the forefront [6,7].
Depending on the local context, people with chronic health conditions may be placed at a significantly higher risk of experiencing mental health problems [8]. Depression is the most common neuropsychiatric complication of HIV/AIDS disease [9]. People who are infected with HIV are more likely than the general population to develop depression [10-14]. Depression affects a person’s ability to follow treatment for HIV/AIDS [15]. Depression associated with poor adherence to ART leading to immunological failure and may independently increase HIV progression [16].
Stress, difficult situations in life, drugs side effects, or the impact of HIV on the brain could all contribute to depression in PLWHA. Depression may also hasten the progression of HIV to AIDS [10]. Studies indicate that in patients with HIV disease, severity of de-pression correlates with rapidity of decline in CD4 count, sug-gesting that failure to treat depression may accelerate HIV disease progression and impact on survival [17]. When recent affective losses (death or rejection of any kind), the rate of hospitalizations, a faster progression of opportunistic infections, or physical deteri¬oration occur, there may be a greater chance of depression in HIV/ AIDS patients [18].
Depressive symptom among HIV-positive clients is associated with low income, widowed, being female, non-adherence of ART, having frequent of schedule for clinical visit in a month, low educational status, being female, age category [40-49], and having stage III and Stage IV HIV-related symptom [11,12,19-22]. Being mentally impaired has been linked with an impaired adherence to ART and poor treatment outcome, decrease in CD4 count and increase in viral load [23]. In addition, depression has been associated with high risk behaviors like engaging in unsafe sex [24].
Early identification of depressive symptoms among HIV-positive individuals is critical to improving health outcomes in this vulner¬able population. In HIV care, treating depressed symptoms may improve quality of life and lower the effect of depression on HIV clinical advancement. Although studies on depression and HIV are numerous, research is limited on the factors that contribute to depression among HIV-positive individuals. However, little is known about how depression affects one's socioeconomic status and physical health after receiving antiretroviral therapy (ART).
Thus, the aim of this study was to identify the magnitude of depression among HIV positive individuals attending ART clinics of Wolaita Zone, South Ethiopia. This study finding will give direction for further interventions and provision of comprehensive care and bases for further study.
Objectives
• To assess the prevalence of depression among HIV-positive individuals attending ART clinics of Wolaita Zone
• To identify determinants of depression among HIV-positive individuals attending ART clinics of Wolaita Zone
Methods And Materials
Study Area and Period
The study was conducted in hospitals and health centers providing ART clinics in Wolaita Zone, Southern regional state, located 387 Km from Addis Ababa. Regarding public health facilities in Zone, there is 1 teaching and referral hospital, 4 primary hospitals and 68 health centers. This study was conducted among HIV positive individuals attending ART clinics of Wolaita Zone from Dec- Jan, 2021.
Study Design
A health facility-based cross-sectional study design was used
Population
• Source population: All HIV-positive individuals attending ART clinics in Wolaita Zone
• Study population: All HIV-positive individuals attending selected ART clinics of Wolaita Zone
Inclusion and Exclusion Criteria
Inclusion Criteria
All HIV-positive individuals attending ART clinic for at least the past 6 months with CD4 counts measured within the last 6 months were included in the study.
Exclusion Criteria
Individuals who are critically sick and unable to hear, with known psychiatric diagnosis, and are on ART for less than 6 months were excluded.
Sample Size Calculation
The sample size was calculated using single population formula taking the prevalence of depression in the study conducted in Hawassa, South Ethiopia, which is 48.6%, at a confidence level of 95%, with a 5% margin of error (Bereket et al., 2018).
![]()
Where, n = the minimum sample size, Z = the desired level of confidence interval 95% (1.96), sample size was 384; by adding 10% non-response rate and multiplying by 1.5 design effect final sample size was 634
Sampling Procedure
To get adequate and well representing sample from HIV positive individuals attending ART clinic, institutions was clustered based on their level and proportional allocation was made based on case number in each ART clinics of Wolaita Zone. Participants was selected using systematic random sampling techniques. Every sixth patients were selected.
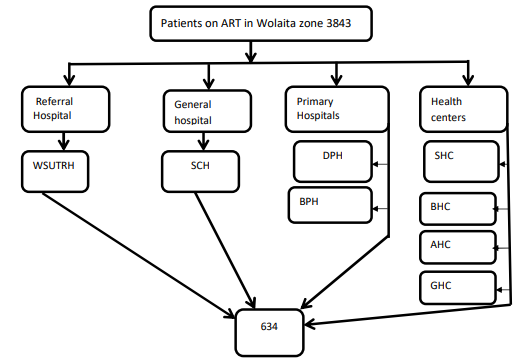
*WSUTRH-Wolaita Sodo University Teaching and Referral Hospital*SCH-Sodo Christian Hospital *DPH-Dubo Primary Hospital
*BPH Bedesa Primary Hospital SHC-Sodo Health Center BHC-Boditi Health Center AHC-Areka Health Center GHC- Gesuba Health Center
Figure 1: Sampling Procedure to Get HIV Positive Individuals Attending Art Clinics of Wolaita Zone, 2021
Data Collection Methods & Tools
Data Collection Tools
Structured questionnaire was used to collect data. Questionnaire was designed in English and was translated to both Amharic and Wolaita language include patient’s Socio-demographic charac-teristics, personal behaviors, economic factors, life events, drug related factors, health related factors, family or social support related factors, adherence of treatment assessed using the Eight-Item Morisky Medication Adherence Scale. These questionnaire items were developed based on literature, the dependent variable assessed using PHQ-9.
Data Collectors
Nurses with bachelor degree was recruited to collect data in each clinic. Prior to that actual data collection, data collectors were trained about tools, data collection procedure. Two MSc nurses were recruited for supervision.
Data Collection Procedure
Data was collected through direct interview to get quantitative data. First informed voluntary written consent was obtained from each study participant after explaining purpose of study. Structured questionnaire was used to collect data from HIV positive individuals through interview on different variables after they get service they want in ART clinics. The interview was conducted in private place.
Variables
Dependent/Outcome Variable
• Depression among HIV positive individuals
Independent Variables
• Socio-demographic characteristics
• Personal behaviors
• Economic factors
• Life events
• Drug related factors
• Health related factors
• Family or social support related factors
Operational Definitions
• Depression: Those with a PHQ-9 score greater than 9 [25].
• Adherence; Total score of Morisky: With a sum of scores 8=high, 6 to <8=medium and <6=low adherence to therapy [26].
Data Quality Control
Data quality was controlled through training of data collectors on questionnaire, ways of conducting interview. Data collectors were supervised by 2 supervisors and principal investigator was received report on daily basis. Before actual data collection, pretest was conducted two health center/hospital. After pretest any ambiguity, confusions, difficult words and differences in understanding was revised based on pretest experience. Completeness and consistency of questionnaire and checklist was checked before and immediately after interview by each data collector and supervisor. Simple frequencies and cross tabulation were done for identifying missing data, and inconsistency.
Data Processing and Analysis
First data was coded, completeness and consistencies of question¬naires was checked and double data entry was made using Epi data 3.02 software. Then the data was exported to the SPSS statistical package version 20 for further analysis. Before analysis, data was further cleaned for possible errors. Data was presented in frequen¬cy, proportions and summary statistics to describe the study variables.
Bivariate analysis was carried out to identify candidates for multivariate analysis. Variables whose p value less than 0.25 in bivariate analysis was included in multivariable logistic regression. Then multivariate logistic regression analysis was performed to identify independent predictors by controlling for possible confounders. AOR at 95% CI with p-value < 0.05 was estimated to identify the associated factors on multivariate logistic regression. Variables was interpreted as having statistically significant association when p < 0.05 in multivariate logistic regression.
Ethical Consideration
This study approved by Institutional Health Research Ethical Review Committee of Wolaita Sodo University College of Health and Medical Sciences with the reference number of 08/01/13 with project code of CHSM/ERC/1. Letter was written from college to each Hospital and health centers. Data collection was made after informed written voluntary consent is taken from each participating patients after informing about study. Patient with depression was linked to social support center or psychiatry unit.
Results
Socio-demographic Characteristics This study was conducted on 596 participants, making the response rate 94%. More than half of the respondents were females. The mean age of the respondents was 35.39 years with standard deviation of 11.41. Married participants and those from urban area were taking more than half proportion of the respondents. Mothers share the highest proportion in family responsibility, the respondents are the main sources of income in majority of respondents, and majority are not happy by their monthly income. Those who own the living house takes higher share (56.9%) among the study participants as described in the table 1 below.
|
Variables |
Category |
Frequency |
Percent |
|
Sex |
Male |
268 |
44.8 |
|
Female |
330 |
55.2 |
|
|
Age |
≤25 |
91 |
15.2 |
|
26-35 |
235 |
39.3 |
|
|
≥36 |
272 |
45.5 |
|
|
Marital status |
Single |
78 |
13 |
|
Married |
308 |
51.5 |
|
|
Divorced |
102 |
17.1 |
|
|
Widowed |
110 |
18.1 |
|
|
Place of residence |
Urban |
416 |
69.6 |
|
Rural |
182 |
30.4 |
|
|
Educational status |
Unable to read & write |
183 |
30.6 |
|
Able to read & write |
157 |
26.3 |
|
|
Primary education |
152 |
25.4 |
|
|
Secondary and above |
106 |
17.7 |
|
|
Responsibility in family |
Father |
220 |
36.8 |
|
Mother |
288 |
48.2 |
|
|
Child |
74 |
12.4 |
|
|
Relative |
16 |
2.7 |
|
Occupation |
Farmer |
73 |
12.2 |
|
Private business |
300 |
50.2 |
|
|
Employee |
83 |
13.9 |
|
|
Student |
25 |
4.2 |
|
|
Housewife |
100 |
16.7 |
|
|
Others |
17 |
2.8 |
|
|
Monthly income (Eth. Birr) |
≤500 |
179 |
29.9 |
|
501-1500 |
202 |
34.1 |
|
|
1501-2500 |
77 |
12.9 |
|
|
≥2501 |
138 |
23.1 |
|
|
Source of income |
Respondent |
384 |
64.2 |
|
Others |
214 |
35.8 |
|
|
Satisfaction with income |
Yes |
138 |
23.1 |
|
No |
460 |
76.9 |
|
|
House ownership |
Private |
340 |
56.9 |
|
Rented |
258 |
43.1 |
Table 1: Socio-Demographic Characteristics of the Participants in Art Clinics of Wolaita Zone, South Ethiopia, 2021
Personal and Clinical Characteristics
The respondents were asked for their personal and clinical characteristics which are the main independent variables. More than three-fourths of the respondents had no history of depression in their lifetime and also in their family members and live with their nuclear family members and had good relations with their family members. Nearly all were making regular follow-ups of their health status, comply with the prescribed regimen properly, and are in stage I of HIV infection. Tuberculosis co-infection was reported in 213 (35.6%) participants and 226 (37.8%) faced the sleep problems as shown in table 2 in detail.
|
Variables |
Category |
Frequency |
Percent |
|
History of depression |
Yes |
145 |
24.2 |
|
No |
453 |
75.8 |
|
|
With whom the respondent lives |
Nuclear family |
457 |
76.4 |
|
Relatives |
48 |
8 |
|
|
Others |
93 |
15.6 |
|
|
Substance use |
Yes |
38 |
6.4 |
|
No |
560 |
93.6 |
|
|
|
|
|
|
|
Relationship with family members |
Good |
519 |
86.8 |
|
Poor |
79 |
13.2 |
|
|
Support from friends |
Yes |
271 |
45.3 |
|
No |
327 |
54.7 |
|
|
Discrimination |
Yes |
248 |
41.5 |
|
No |
350 |
58.5 |
|
|
Family history of Depression |
Yes |
124 |
20.7 |
|
No |
474 |
79.3 |
|
|
Regular medical check-up |
Yes |
577 |
96.5 |
|
No |
21 |
3.5 |
|
|
HIV infection staging |
Stage I |
523 |
87.5 |
|
|
Stage II |
29 |
4.8 |
|
Stage III |
32 |
5.4 |
|
|
Stage IV |
14 |
2.3 |
|
|
TB co-infection |
Yes |
213 |
35.6 |
|
No |
385 |
64.4 |
|
|
Taking medications Properly |
Yes |
552 |
92.3 |
|
No |
46 |
7.7 |
|
|
Ever faced sleep problem |
Yes |
226 |
37.8 |
|
No |
372 |
62.2 |
|
|
Presence of severe side effects |
Yes |
58 |
9.7 |
|
No |
540 |
90.3 |
|
|
Recent loss of family Member |
Yes |
120 |
20.1 |
|
No |
478 |
79.9 |
Table 2: Personal and Clinical Characteristics of the Respondents Attending Art Clinics of Wolaita Zone, 2021
Prevalence of Depression
The depression was computed from 10 questions of the tool. The maximum score of the tool was 30 and the minimum was 0. In the current study, the prevalence of depression among HIV-positive individuals attending ART clinics in the Wolaita zone was found to be 32.6% at 95% CI [29%, 36%].
Figure 1 below shows the prevalence of depression among HIV-positive individuals attending ART clinics of Wolaita Zone.

Figure 1: Prevalence of Depression Among HIV-Positive Individuals Attending Art Clinics of Wolaita Zone
Bivariate and Multivariate Analysis Results
In the multivariate analysis, marital status, sleep problems, living with nuclear families, having tuberculosis co-infection, family history of depression, and place of medical follow-up were variables found to be associated with depression among HIV-positive individuals attending ART clinics of Wolaita Zone. Among marital status, being single [AOR = 0.205, CI [0.047, 0.90]] was found to be preventive from the occurrence of depression. Living out of a nuclear family, specifically living with relatives [AOR=6.79, 95 CI [1.92, 24.1]] found to be associated with the occurrence of depression.
Table Bivariate and multivariate analysis results of variables asso¬ciated with depression among HIV-positive individuals attending ART units of Wolaita Zone, 2021
|
Variables |
Category |
Depression |
COR (95%CI) |
AOR (95%CI) |
P-value |
|
|
Yes |
No |
|||||
|
Income (Eth. Birr) |
≤500 |
73 |
106 |
2.28[1.39, 3.74]* |
1.43[0.74,2.78] |
|
|
501-1500 |
69 |
133 |
1.72[1.05, 2.81]* |
0.57[0.20,1.57] |
|
|
|
1501-2500 |
20 |
57 |
1.16[0.61,2.22] |
1.12[0.45,2.77] |
|
|
|
≥2500 |
32 |
106 |
1 |
1 |
|
|
|
Marital status |
Single |
20 |
58 |
0.49[0.26,0.93]* |
0.205[0.047,0.90] |
0.036 |
|
Married |
79 |
228 |
0.49[0.31,0.78] |
1.04[0.49, 2.19] |
|
|
|
Divorced |
50 |
52 |
1.37[0.79,2.36] |
1.6 [0.66, 3.91] |
|
|
|
Widowed |
45 |
64 |
1 |
1 |
|
|
|
Educational status |
Unable to write and read |
80 |
102 |
2.19[1.30, 3.68] |
2.04[0.77,5.42] |
|
|
Able to write and read |
102 |
2.19[1.30, 3.68] |
2.04[0.77,5.42] |
|
|
|
|
Able to write |
62 |
95 |
1.82 [1.06,3.11] |
0.65[0.25,1.71] |
|
|
|
Primary Education |
24 |
127 |
0.53[0.29, 0.97] |
0.68[0.25,1.88] |
|
|
|
Secondary education |
28 |
78 |
1 |
1 |
|
|
|
Family responsibility |
Father |
73 |
145 |
0.229[0.077, 0.68] |
1.18[0.57,2.45] |
|
|
Mother |
93 |
195 |
0.217[0.073, 0.64] |
0.82[0.22,3.02] |
|
|
|
Child |
17 |
57 |
0.14[0.04,0.45] |
3.65[0.51,26.3] |
|
|
|
Relative |
11 |
5 |
1 |
1 |
|
|
|
Satisfaction with income |
Yes |
20 |
118 |
1 |
1 |
|
|
No |
174 |
284 |
3.62 [2.17, 6.02] |
1.67[0.81,3.44] |
|
|
|
Source of income |
Respondent |
142 |
240 |
1.84[1.27, 2.68] |
1.13[0.61,2.01] |
|
|
Other |
52 |
162 |
1 |
1 |
|
|
|
Homeownership |
Private |
93 |
245 |
1 |
1 |
|
|
Rental |
101 |
157 |
1.70 [1.20, 2.40] |
0.99[0.55,1.82] |
|
|
|
History of depression |
Yes |
106 |
39 |
11.21 [7.26, 17.3] |
1.65[0.78,3.50] |
|
|
No |
88 |
363 |
1 |
1 |
|
|
|
Living with |
Nuclear Family |
126 |
330 |
1 |
1 |
|
|
Relatives |
39 |
9 |
11.35[5.34,24.1] |
6.79[1.92, 24.1]* |
0.03 |
|
|
Others |
29 |
63 |
1.21[0.74,1.96] |
0.97[0.48,1.95] |
|
|
|
Relation with family |
Good |
159 |
358 |
1 |
1 |
|
|
Poor |
35 |
44 |
1.79 [1.11, 2.90] |
1.18[0.53,2.64] |
|
|
|
Support from friends |
Yes |
107 |
163 |
0.555[.392, .784] |
0.76[0.42,1.38] |
|
|
No |
87 |
239 |
1 |
1 |
|
|
|
Experienced Discrimination |
Yes |
142 |
106 |
7.63[5.18, 11.23] |
1.83[0.97,3.42] |
|
|
No |
52 |
296 |
1 |
1 |
|
|
|
Family history of depression |
Yes |
104 |
20 |
22.1[12.98,37.53] |
5.06[2.02,12.63] |
0.000 |
|
No |
90 |
382 |
1 |
1 |
|
|
|
Place of follow-up |
Government facility |
190 |
318 |
12.55 [4.53,34.76] |
7.67[1.98,29.74] |
0.003 |
|
Private facility |
4 |
84 |
1 |
1 |
|
|
|
TB co-infection |
Yes |
126 |
86 |
6.81 [4.66, 9.95] |
2.3[1.28, 4.21] |
0.006 |
|
No |
68 |
316 |
1 |
1 |
|
|
|
Sleep problem |
Yes |
138 |
88 |
1 |
2.1[1.16, 3.72] |
0.013 |
|
|
No |
56 |
314 |
0.114 [0.77, 0.168] |
1 |
|
|
Severe side-effects |
Yes |
39 |
19 |
5.07 [2.84, 9.05] |
1.49[0.58,3.87] |
|
|
No |
155 |
383 |
1 |
1 |
|
|
|
Recent family Loss |
Yes |
87 |
33 |
9.1 [5.77, 14.33] |
1.63[0.65,2.84] |
|
|
No |
107 |
369 |
1 |
1 |
|
|
|
CD4 count |
<500 |
91 |
164 |
1.28 [0.98, 1.81] |
1.64[0.97,2.97] |
|
|
>501 |
103 |
238 |
1 |
1 |
|
|
|
Duration on ART (months) |
<12 |
15 |
45 |
1 |
1 |
|
|
13-59 |
33 |
110 |
0.6 [0.31,1.16] |
0.77[0.29,2.05] |
|
|
|
60-119 |
81 |
130 |
0.54 [0.33,0.88] |
1.19[0.56,2.52] |
|
|
|
>120 |
65 |
117 |
1.12 [0.74,1.69] |
1.20[0.62,2.29] |
|
Discussion
This study presents significant information regarding depression experienced by individuals with HIV who attending HAART treatment in the study's contexts. The study found that the prevalence of depression among participants was about one third (32.6%). The factors of depression included those with sleep problem, co-infection with tuberculosis, a family history of depression, place of medical follow-up and living with relatives (outside of a nuclear family). On the other hand, being single was found to be preventive from the occurrence of depression.
Findings from this study is higher when compared to the rate of depression among general population in Ethiopia 17.5%, [11]. The stigma linked to HIV among these communities may increase their risk of developing depression that could be responsible for it. The results of this study is comparable with previous study conducted among HIV positive individuals in Jimma 30.2% , Addis Ababa 35.5% , Gurage Zone 37.5% , Hawassa 32.0% , Somalia 3.5% , Kenya 35.6%, and pooled prevalence in Sub-Saharan Africa which ranged between 9% and 32% [27-33]. On other hand, similar study showed lower prevalence of depression among individuals with HIV such as Aksum 14.6% , Mecha district, Northwest Ethiopia 13.3% , National Health Survey of Ethiopia 9.1% , and Kenya 13.8% , However, this result lower when compared with study conducted in different parts of Ethiopia Gimbi 41.7% , Bahir Dar 57.9% , Bale 44.9% , West Hararghe 52.4% , Harar 45.8% , and also Nigeria 39.6% , Sudan 63.1% , and Uganda 46% [10,20,34-42]. The differences are may be due to the different measurement tools, sample size variations, different locations of the study, sociocultural features participants, and different study setting.
In this study, sleep problem is associated with depression among individuals with HIV in which those with sleep difficulty two times more likely to report sleep problem than those did not report sleep problem. This supported by evidence from Hawassa University hospital southern Ethiopia, Mettu Karl hospital southwest Ethiopia, Dessie town northeast Ethiopia in which the prevalence of poor quality of sleep found to be 57.6%, 57.1%, 36% respectively [43-45]. This might be explained by bidirectional relationship between depression and sleep problem and the effect of HIV positive on both neuropsychiatric complications.
Co-infection with tuberculosis is also important factor linked with depression in this study. Individuals with positive TB status 6 times more likely to develop depression when compared with those with negative TB status. This finding could be supported by the evidence from the Oromia region in which tuberculosis and HIV co-infected patients had significantly greater risk of common mental disorders (63.7%), and study from the Kenya depression accounts 31%, among those who has positive clinical status of both TB and HIV [22,46]. There is also another evidence which suggests prevalence of depression among TB patients was found to be 45.19%, and having comorbid with TB and HIV might increase the severity of depression [47]. TB and HIV can contribute to depression through their direct and complex interplay with each other, and it is important for healthcare providers to recognize and address the mental health needs of individuals dealing with TB and HIV.
Family history of depression is another factor associated with depression in this study. Those with history of depression with in their family more likely to report depression when compared with their counterparty. Studies have found that individuals with a family history of depression are more likely to experience depressive symptoms, and be diagnosed with major depressive disorder (MDD) than those without a family history [48]. This association has been observed in both HIV-positive and HIV-negative populations. One potential explanation for this association is the role of genetics. In the context of HIV, family history of depression may be particularly relevant due to the added stressors associated with the illness.
Place of follow up is another important factor which associated with depression in this study. Individuals who follow their treatment at government health facility more likely to report depression than those who follow their treatment at private health facilities. This might be due to the patient preference to private health care providers, with the possible reasons of better and more flexible access, shorter waiting, greater confidentiality, which might differ quality of care in further and result in different rate of depressive symptoms in the same group of population [49,50]. The finding of this study that living outside of a nuclear family is associated with depression among HIV-positive individuals is consistent with previous research on the relationship between social support and mental health outcomes [51]. This finding also consistent with systematic review report of HIV-positive individuals who live outside of a nuclear family may be at higher risk of depression due to the lack of social support and increased isolation [52].
In this study, being single is preventive factor as contrary to general assumption of risk factor for depression. However, this finding also supported by the evidence which reports being single or being divorced/widowed were associated with depressive symptoms at every age in men but for women turn, being single was associated with depressive symptoms [53]. Married women suffer more depression than unmarried ones [54]. This could be explained by the majority of participants in this study are women.
Conclusion
Depression is a prevalent mental health issue among the participants, with approximately one third of them experiencing symptoms of depression. The study identified several factors that were associated with depression, including sleep problems, living outside of a nuclear family, co-infection with tuberculosis, a family history of depression, and place of medical follow-up. Being single was found to be a protective factor against the occurrence of depression. These findings suggest that healthcare professionals should be aware of the risk factors for depression, particularly in patients with sleep problems, co-infection with tuberculosis, and a family history of depression. Additionally, the findings indicate that social support, such as living in a nuclear family, may be beneficial in preventing depression. However, the protective effect of being single against depression should be interpreted with caution, as social isolation can also contribute to poor mental health outcomes.
Limitation
The following potential limitations should be taken into consideration when considering the study's conclusions. Firstly, this study only included individuals who attend the antiretroviral treatment clinic, which may limit the generalizability of the findings to those who do not attend such clinics. Also, those who attend the clinic may be more likely to have depression compared to those who do not attend, leading to potential self-selection bias. Participants may not be truthful about their depression symptoms due to social desirability bias. Secondly, this study may not be able to establish causality as it is based on a cross-sectional design. Third, the study depend on self-reported data which may not be accurate due to recall bias or social desirability bias. And finally, the study only focuses on depression among HIV-positive individuals and does not explore other mental health conditions or factors that may contribute to depression.
Recommendation
Healthcare professionals should screen patients for depression, particularly those with sleep problems, co-infection with tuberculosis, and a family history of depression. Early identification and treatment of depression can prevent it from worsening and improve outcomes for patients. Family support should be promoted to prevent depression. Social support should be provided to patients who are at risk of depression. Support groups, community engagement activities, and counseling services can help patients build social connections and reduce feelings of isolation. Further research is needed to better understand the relationship between social factors and depression.
Disclosure statement: Authors has no conflict of interest to declare. The authors didn’t receive fund for this study.
References
- EDITION, F. (1980). Diagnostic and statistical manual of mental disorders. American Psychiatric Association, Washington, DC, 205-224.
- EDITION, F. (1980). Diagnostic and statistical manual of mental disorders. American Psychiatric Association, Washington, DC, 205-224.
- Shao, Y., & Williamson, C. (2012). The HIV-1 epidemic: low-to middle-income countries. Cold Spring Harbor perspectives in medicine, 2(3), a007187.
- Del Rio, C. (2017). The global HIV epidemic: What the pathologist needs to know. In Seminars in diagnostic pathology (Vol. 34, No. 4, pp. 314-317). WB Saunders.
- addisstandard. Analysis: HIV/AIDS is surging in Ethiopia, again [Internet]. Addis Standard. 2017 [cited 2023 Jul 25]. Available from: https://addisstandard.com/analysis-hivaids-is-surging-in-ethiopia-again/
- Huang, Y., Zhou, O., Zheng, Z., Xu, Y., Shao, Y., Qin, C., ... & Jiang, J. (2020). Effect of AIDS-defining events at initiation of antiretroviral therapy on long-term mortality of HIV/ AIDS patients in Southwestern China: a retrospective cohort study. AIDS Research and Therapy, 17(1), 44.
- Oguntibeju, O. O. (2012). Quality of life of people living with HIV and AIDS and antiretroviral therapy. HIV/AIDS-Research and Palliative Care, 117-124.
- Chronic Illness and Mental Health: Recognizing and Treating Depression.
- Obiajulu V. (2011). Neuropsychiatric Manifestations of HIV Infection and AIDS. In: Dumais N, editor. HIV and AIDS- Updates on Biology, Immunology, Epidemiology and Treatment Strategies [Internet].
- Beyene Gebrezgiabher, B., Huluf Abraha, T., Hailu, E., Siyum, H., Mebrahtu, G., Gidey, B., ... & Angesom, T. (2019). Depression among Adult HIV/AIDS Patients Attending ART Clinics at Aksum Town, Aksum, Ethiopia: A Cross- Sectional Study. Depression research and treatment, 2019(1), 3250431.
- Molla, G. L., Sebhat, H. M., Hussen, Z. N., Mekonen,B., Mersha, W. F., & Yimer, T. M. (2016). Depression among Ethiopian adults: cross-sectional study. Psychiatry journal, 2016(1), 1468120.
- Elbadawi, A., & Mirghani, H. (2017). Depression among HIV/ AIDS Sudanese patients: a cross-sectional analytic study. The Pan African Medical Journal, 26, 43.
- Girma, D., Assegid, S., & Gezahegn, Y. (2021). Depression and associated factors among HIV-positive youths attending antiretroviral therapy clinics in Jimma town, southwest Ethiopia. PLoS One, 16(1), e0244879.
- Anbesaw, T., & Fekadu, B. (2022). Depression and associated factors among older adults in Bahir Dar city administration, Northwest Ethiopia, 2020: Cross-sectional study. Plos one, 17(8), e0273345.
- Moraes, R. P. D., & Casseb, J. (2017). Depression and adherence to antiretroviral treatment in HIV-positive men in São Paulo, the largest city in South America: Social and psychological implications. Clinics, 72(12), 743-749.
- Deshmukh, N. N., Borkar, A. M., & Deshmukh, J. S. (2017). Depression and its associated factors among people living with HIV/AIDS: Can it affect their quality of life?. Journal of family medicine and primary care, 6(3), 549-553.
- Effendy, E., Amin, M. M., de Vega, L., & Utami, N. (2019). The association between CD-4 level, stress and depression symptoms among people living with HIV/AIDS. Open access Macedonian journal of medical sciences, 7(20), 3459.
- Rivera-Rivera, Y., Vázquez-Santiago, F. J., Albino, E., del C Sánchez, M., & Rivera-Amill, V. (2016). Impact of depression and inflammation on the progression of HIV disease. Journal of clinical & cellular immunology, 7(3), 423.
- Anbesaw, T., & Fekadu, B. (2022). Depression and associated factors among older adults in Bahir Dar city administration, Northwest Ethiopia, 2020: Cross-sectional study. Plos one, 17(8), e0273345.
- Zerihun E, Girma F. (2023). Determinants of Depressive Symptoms in People Living with HIV in the Case of Low-Resource Communities in Eastern Ethiopia: A Multi-Centered Study [Internet].
- Agazhu HW, Giru BW, Wurjine TH. Prevalence and Associated Factors of Depression among HIV/AIDS Patients Attending Anti-Retroviral Therapy Clinics at Gurage Zone Selected Government Hospitals, Southwest, South nations, Nationalities and Peoples’ Region, Ethiopia, 2018. 2018;9(12).
- Lee, E. (2015). Prevalence of depression among active TB and TB/HIV patients in Kisumu County.
- Adejumo, O., Oladeji, B., Akpa, O., Malee, K., Baiyewu, O., Ogunniyi, A., ... & Taiwo, B. (2016). Psychiatric disorders and adherence to antiretroviral therapy among a population of HIV-infected adults in Nigeria. International journal of STD & AIDS, 27(11), 938-949.
- Tesfaye, Y., Negash, A., Gebrehiwot, T. T., Tessema, W., Anand, S., Ahmed, G., & Alemu, D. (2019). Is there association between risky sexual behaviors and depression symptoms among youth? A case of Jimma University Students, Ethiopia. Psychiatry journal, 2019(1), 3757656.
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. Journal of general internal medicine, 16(9), 606-613.
- Janezic, A., Locatelli, I., & Kos, M. (2017). Criterion validity of 8-item Morisky Medication Adherence Scale in patients with asthma. PloS one, 12(11), e0187835.
- Girma, D., Assegid, S., & Gezahegn, Y. (2021). Depression and associated factors among HIV-positive youths attending antiretroviral therapy clinics in Jimma town, southwest Ethiopia. PLoS One, 16(1), e0244879.
- Abebe, H., Shumet, S., Nassir, Z., Agidew, M., & Abebaw,D. (2019). Prevalence of depressive symptoms and associated factors among HIV-positive youth attending ART follow-up in Addis Ababa, Ethiopia. AIDS research and treatment, 2019(1), 4610458.
- Agazhu HW, Giru BW, Wurjine TH. Prevalence and Associated Factors of Depression among HIV/AIDS Patients Attending Anti-Retroviral Therapy Clinics at Gurage Zone Selected Government Hospitals, Southwest, South nations, Nationalities and Peoples’ Region, Ethiopia, 2018. 2018;9(12).
- Duko, B., Toma, A., Asnake, S., & Abraham, Y. (2019). Depression, anxiety and their correlates among patients with HIV in South Ethiopia: an institution-based cross-sectional study. Frontiers in psychiatry, 10, 290.
- Mohamud, A. K., Ahmed, O. A., Mohamud, A. A., & Dirie, N.I. (2023). Prevalence of and factors associated with depression among adult patients living with HIV/AIDs undergoing ART unit in Banadir hospital, Mogadishu Somalia. BMC psychiatry, 23(1), 232.
- Jeruto, E., Mogere, D. M., Kerochi, A., Maureen, K. J., & Gwandi, M. P. (2022). Risk factors associated with depression among HIV positive women at Mama Lucy Kibaki hospital in Nairobi County, Kenya. International Journal of Community Medicine and Public Health, 9(6), 2377.
- Bernard, C., Dabis, F., & de Rekeneire, N. (2017). Prevalence and factors associated with depression in people living with HIV in sub-Saharan Africa: a systematic review and meta-analysis. PloS one, 12(8), e0181960.
- Hailemariam, S., Tessema, F., Asefa, M., Tadesse, H., & Tenkolu, G. (2012). The prevalence of depression and associated factors in Ethiopia: findings from the National Health Survey. International journal of mental health systems, 6(1), 23.
- Nyongesa, M. K., Mwangi, P., Wanjala, S. W., Mutua, A. M., Newton, C. R., & Abubakar, A. (2019). Prevalence and correlates of depressive symptoms among adults living with HIV in rural Kilifi, Kenya. BMC psychiatry, 19(1), 333.
- Abadiga, M. (2019). Depression and its associated factors among HIV/AIDS patients attending ART clinics at Gimbi General hospital, West Ethiopia, 2018. BMC research notes, 12(1), 527.
- Anbesaw, T., & Fekadu, B. (2022). Depression and associated factors among older adults in Bahir Dar city administration, Northwest Ethiopia, 2020: Cross-sectional study. Plos one, 17(8), e0273345.
- Desta, F., Tasew, A., Tekalegn, Y., Zenbaba, D., Sahiledengle, B., Assefa, T., ... & Atlaw, D. (2022). Prevalence of depression and associated factors among people living with HIV/AIDS in public hospitals of Southeast Ethiopia. BMC psychiatry, 22(1), 557.
- Bezatu Mengistie MM. (2015). Prevalence of Depression and Associated Factors among HIV Patients Seeking Treatments in ART Clinics at Harar Town, Eastern Ethiopia. J AIDS Clin Res [Internet].
- Olatayo Adeoti A, Dada MU, Fadare JO. (2018). Prevalence of Depression and Anxiety Disorders in People Living with HIV/AIDS in a Tertiary Hospital in South Western Nigeria. Med Rep Case Stud [Internet].
- Elbadawi A, Mirghani H. (2017). Depression among HIV/ AIDS Sudanese patients: a cross-sectional analytic study. Pan Afr Med J [Internet].
- Kemigisha, E., Zanoni, B., Bruce, K., Menjivar, R.,Kadengye, D., Atwine, D., & Rukundo, G. Z. (2019).Prevalence of depressive symptoms and associated factors among adolescents living with HIV/AIDS in South Western Uganda. AIDS care.
- Bedaso, A., Abraham, Y., Temesgen, A., & Mekonnen, N. (2020). Quality of sleep and associated factors among people living with HIV/AIDS attending ART clinic at Hawassa University comprehensive specialized Hospital, Hawassa, SNNPR, Ethiopia. Plos one, 15(6), e0233849.
- Abdu, Z., & Dule, A. (2020). Poor quality of sleep among HIV-positive persons in Ethiopia. HIV/AIDS-Research and Palliative Care, 621-628.
- GebreEyesus, F. A., Degu, F. S., Yohanes, Y. B., & Azagew,W. (2023). Sleep quality and associated factors among adult people living with HIV on follow-up at Dessie Town Governmental Health Facilities Antiretroviral Therapy Clinics, Northeast, Ethiopia, 2020, a multicenter cross-sectional study. BMC psychiatry, 23(1), 132.
- Deribew, A., Tesfaye, M., Hailmichael, Y., Apers, L., Abebe, G., Duchateau, L., & Colebunders, R. (2010). Common mental disorders in TB/HIV co-infected patients in Ethiopia. BMC infectious diseases, 10(1), 201.
- Duko, B., Bedaso, A., & Ayano, G. (2020). The prevalence of depression among patients with tuberculosis: a systematic review and meta-analysis. Annals of general psychiatry, 19(1), 30.
- Monroe, S. M., Slavich, G. M., & Gotlib, I. H. (2014). Life stress and family history for depression: The moderating role of past depressive episodes. Journal of psychiatric research, 49, 90-95
- McCombie, S. C. (1996). Treatment seeking for malaria: a review of recent research. Social science & medicine, 43(6), 933-945.
- Aljunid, S. (1995). The role of private medical practitioners and their interactions with public health services in Asian countries. Health policy and planning, 10(4), 333-349.
- Shao, B., Song, B., Feng, S., Lin, Y., Du, J., Shao, H., ...& Wang, F. (2018). The relationship of social support, mental health, and health-related quality of life in human immunodeficiency virus-positive men who have sex with men: From the analysis of canonical correlation and structural equation model: A cross-sectional study. Medicine, 97(30), e11652.
- Weldesenbet, A. B., Kebede, S. A., & Tusa, B. S. (2020). The Effect of Poor Social Support on Depression among HIV/ AIDS Patients in Ethiopia: A Systematic Review and Metaâ?ÂÂAnalysis. Depression Research and Treatment, 2020(1), 6633686.
- Grundström, J., Konttinen, H., Berg, N., & Kiviruusu, O. (2021). Associations between relationship status and mental well-being in different life phases from young to middle adulthood. SSM-population health, 14, 100774.
- Wu, X., & DeMaris, A. (1996). Gender and marital status differences in depression: The effects of chronic strains. Sex roles, 34(5), 299-319.