
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Case Report - (2022) Volume 4, Issue 1
De Novo Minimal Changes Disease Associated to Inoculation with Adenovirus Vector Vaccine (Sputnik V)
Received Date: Dec 25, 2021 / Accepted Date: Dec 30, 2021 / Published Date: Jan 05, 2022
Copyright: ©Rios Maria Celeste. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Rios Maria Celeste, Weiss Natalia, Parodi Francesco and Alberton Valeria. (2022) De Novo Minimal Changes Disease Associated to Inoculation with Adenovirus Vector Vaccine (Sputnik V) Adv J Uro Nephro 4(1): 13-16.
Abstract
Due to the pandemic caused by the virus SARS-CoV-2, multiple therapeutic and preventive strategies have been developed in order to avoid its propagation. Vaccines have been proved to be the most efficient means to control the spread of COVID 19, which has prevented both massive admissions of critical patients to intensive care units and the collapse of the health system from happening.
To the present day there are different tested vaccine platforms with adenovirus vectors, inactivated vaccines and nucleic acid vaccines, among others [1]. As the vaccination process moved forward around the globe, there has been a number of publications reporting on adverse renal events, which included case reports on Secondary Nephrotic Syndome derived from Minimal Changes Disease (MCD) after the application of both, nucleic acid (RNAm) and adenovirus vector vaccines.
Case presentation: male patient presented with nephrotic syndrome without microhematuria and with renal dysfunction after the application of the second dose of SPUTNIK V vaccine, which is why a renal biopsy was carried out. Such biopsy reported it was a case of MCD, which had a complete remission after six weeks of oral corticosteroids.
Introduction
MCD represents approximately 15% of the reports on renal bi-opsies of adult patients with Idiopathic Nephrotic Syndrome [2]. This anatomopathological pattern can spring secondarily from neoplasia, toxic reactions to drugs, immunizations, immunological diseases and miscellaneous entities. Such association of MCD sec-ondary to an extraglomerular situation is purely casual [3]. Recent-ly, numerous publications have described the development of de novo and recurrent MCD after vaccination against SARS-CoV-2 (4). In the emerging cases such development appears after the ap¬plication of nucleic acid vaccines (ARNm), as well as adenovirus vector (Janssen vaccine) and inactivated (Cancino) platforms. In this respect we describe the case of a 75 year-old patient without comorbidity, who after the application of the Sputnik V vaccine developed a nephrotic sydrome with kidney failure due to MCD and responded with complete remission after administration of corticosteroids.
Clinical Case
75 year-old patient, male, without pathological antecedents or fre- quent medication use who on July 20 2021 received his second dose of Sputnik V. 24 hours later, he develops a macular erythema-tosus pruritic rash with predominance in his superior and inferior limbs. 4-5 days after the resolving of the skin manifestation, he de¬velops a facial swelling and an increase in the diameter of the su¬perior and inferior limbs. He sees his GP who runs some tests that yield the following: proteinuria 26g/24hs, albumin 2.2mg, urea 62 mg/dl, creatinine 1.2mg/dl, cholesterol 339 mg/dl, hematocrit 48.4 4%, sodium 113. A medical treatment against the nephrotic syn¬drome (loop diuretics and potassium-sparing diuretics) is started, without clinical response. Therefore, the patient is hospitalized for further tests and treatment. When he is admitted, the swelling of limbs is confirmed, together with scrotum and eyelid swelling, ar¬terial hypertension (TA169/90) and an overweight of 14 kg (90 kg, when his usual weight is 76 kg). We carry out a urine sediment analysis which yields: SA: ++++ blood-, OM: Oval fat bodies, cy¬lindrical structure without microhematuria. Renal sonogram with Doppler ultrasound: normal findings. Tests were expanded (table 1). The obtained results show, through electrophoretic proteino¬gram, hypogammaglobulinemia and hypotiroidism with values slightly out of range, which were interpreted to derive from the course of the nephrotic syndrome. The rest of the carried out deter-minations did not show positive results. The patient is prescribed a strict hyposodic and hypotroeic diet, water restriction, a treatment with furosemide 240 mg/day EV associated to albumin to 20% (4 flasks=40g/day), atorvastatin 20 mg/day, enalapril 10mg/day and amiloride 5mg/day. He starts taking meprednisone at a ratio of 1mg/kg per day during six weeks.
A renal puncture was carried out for biopsy, which was analyzed by a nephropathologist, whose report describes two cylinders that include 23 clusters within the different cuts. None of theme is glob¬ally sclerosed. The walls of the capillary tubes appear to be thin and there is no cellular proliferation. Podocytes are hypertrophied.
In some cases there is extensive fibrosis that extends to the hila. The thioflavin image resulted negative in this material. Minimum focus of tubular atrophy and interstitial fibrosis. The tubules signal light dilatation and a strong irregular vacuolization of the lining epithelium. Vessels with no peculiarities. Inmunohistochemistry: IgG, IgA negative. IgM positive intensity +/++++ focal mesangial and segmental. C3, C1q negative fibrinogen. Kappa and lambada negative. Diagnosis: Morphological findings possibly connected to an MCD. Acute tubular injury (Picture 1a-b, 2a-b).
The patient evolves with complete remission, showing a progres¬sive decline in weight up to a dry weight of 72kg and a proteinuria of less than 300mg at the time he left the hospital with normal kidney function.
TABLE 1: Carried out tests
|
DATE |
TEST |
REPORT |
|
24/08/21 |
Immunological Profile |
Antibodies ANA: <1/80 (negative), ANCA: negative, Antibodies anti-DNA: negative, antibodies anti-myeloperoxidase: <3.2 CU (negative), Antibodies anti-protein 3: <2.3 CU (negative), Complement C3: 159 mg/ dl (negative), Complement C4: 34 mg/dl (negative). |
|
24/08/21 |
Electrophoretic Proteinogram |
ALFA 1M: 3.3, ALFA 2M: 31.70, BETA 1M: 8.60, BETA 2M: 7.90, GAMMA M: 8.30, ALFA 1F: 0.15 (VN 0.10-0.30), ALFA 2F: 1.41 (VN 0.50-1.10), BETA 1F: 0.38 (VN 0.50-0.90), BETA 2F: 0.35 (VN 0.20- 0.50), GAMMA F: 0.37 (VN 0.70-1.60). |
|
25/08/21 |
Serology tests |
HBV-AgS, HBV-AgC, HBV-AcS: negative, IgM-HCV: negative, VDRL: negative, VIH: negative. |
|
25/08/21 |
Thyroid Profile |
T3 <40 ug/dl (VN 70-200) T4 4.30 ug/dl (VN 5-12.5) TSH: 5.44 UI/ml (VN: 0.5-4.5), T4L 1.27 ug/dl (VN: 0.75-1.8) ATG: <20 ug/dl (VN <40) |
|
27/08/21 |
Tuberculin test |
Valor: 0 mm |
|
30/08/21 |
Ocular Fundus |
No reportable changes. |
|
15/09/21 |
Abdominal CT |
No reportable changes. |
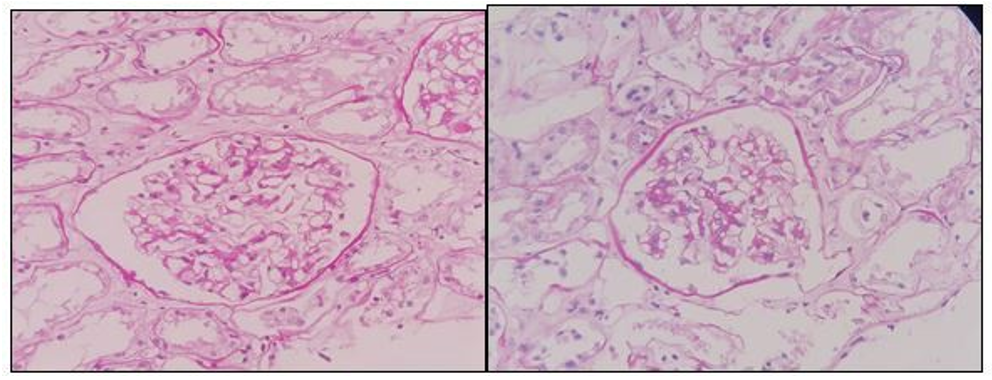
PICTURES 1a-1b: Periodic Acid-Schiff 200X. Glomerulus without significant histological alterations.
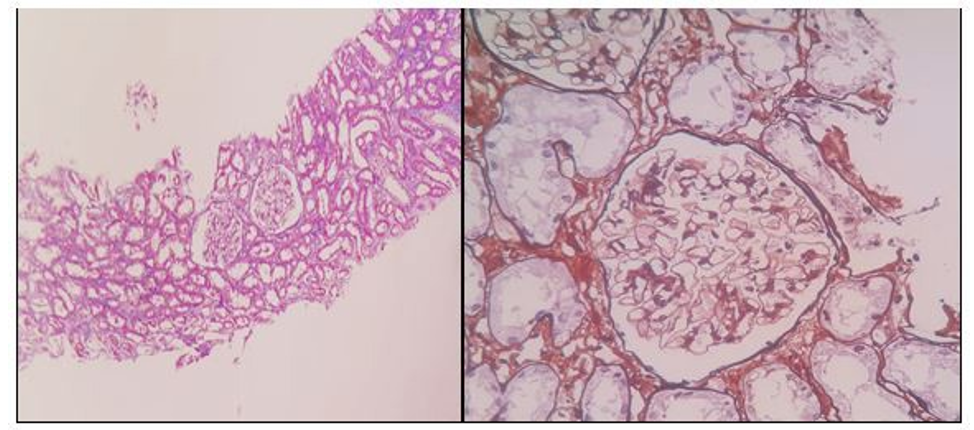
PICTURE 2a-2b: Masson Trichromic Staining 40X. Tubules with vacuolyzation of the lining epithelium. 2b.Silver Methenamine Stain 200X. Thin capillary walls, without deposits or hypercellularity.
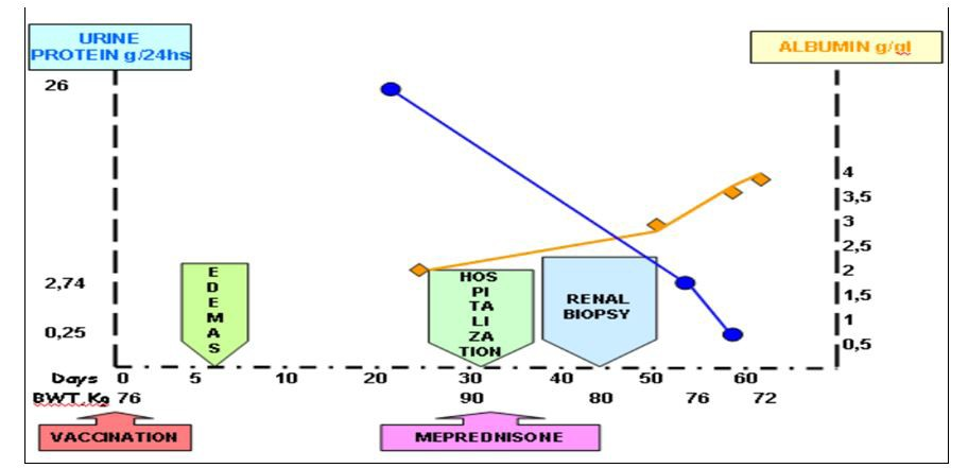
Figure 1: Clinical course after vaccination
Discussion
The development of the MCD after the application of vaccines is not an infrequent event. It has been reported to appear after the administration of vaccines against influenza, polio, hepatitis B, pneumococcal disease, measles, diphtheria and tetanus [5]. There have been many a case related to MCD and Sars-CoV-3 vacci¬nation, among which Pfizer-BioNtech COVID 19 and Moderna are usually mentioned, being both nucleic acid-RNAm vaccines [6]. We have also found, within the literature explored, inactivated vaccines such as CoronaVAc and regarding adenovirus vaccines as Oxford.AstraZeneca Vaccine and only one case linked to JAN- SEN vaccine is to be highlighted [5, 7, 8].
One could argue for different hypotheses on how the inoculation of a vaccine could result into an MCD. Taking into consideration the reports involving RNAm as well as adenovirus vector vac¬cines, this phenomenon could be explained by a potential mech¬anism, presumably not proper of the vaccine, but rather a process of T cells triggered by the vaccine that could cause podocytopathy. Another hypothesis is that of the activation of the immune system in predisposed individuals [9].
To conclude, this report has presented a clinical case of a 75 year-old patient with no relevant background, who developed an MCD manifested through a nephrotic syndrome which sprang from the second dose the Sputnik V vaccine, which is an adenovirus vector vaccine that shares platform with the Janssen vaccine. This last one is associated to such events. The groundbreaking piece of in¬formation of this case is that there are no reports –to the present day- describing the development of MCD after the application of Sputnik V. Although this case goes hand in hand with various publications that link COVID-19 vaccine with the development of an MCD, it is necessary to collect more data and tests to assert whether MCD is effectively linked to vaccines against COVID 19
References
- Zhao J, Zhao S, Ou J, Zhang J, Lan W, et al. (2020). COVID-19: Coronavirus vaccine development updates. Front. Immunol 23: 602256.
- Vivarelli M, Massella L, Ruggiero B and Emma F (2017). Minimal Change Disease. Clin J Am Soc Nephrol 12: 332-345.
- Glassock R (2003). Secondary minimal change disease. Nephrol Dial Transplant 18: 52-58.
- Holzworth A, Couchot P, Cruz-Knight W, Brucculeri M(2021). Minimal Change Disease following the Moderna Mrna-1273 SARS-CoV-2 vaccine. Kidney International 100: 463-464.
- Dirim A, Safak S, Andac B, Garayeva N, Demir E, et al. (2021). Minimal Change disease following vaccination with CoronaVac. Clinical Kidney Journal 14: 2268-2269.
- Levedev L, Sapojnkov M, Wechsler A, Varadi-Levi R, Zamir D, et al. (2021). Minimal change disease following the Pfiz-er-BioNTech COVID-19 Vaccine. Am J Kidney Dis 78:142-145.
- Leclerc S, Royal V, Lamarche C and Laurin L (2021). Minimal change disease with severe acute kidney injury following the Oxford-Aztrazeneca COVID-19 vaccine: A case Report. Am J Kidney Dis 78: 607-610.
- Lim JH, Han MH, Kim YJ, Kim MS, Jung HY, et al. (2021). New-onset nephrotic syndrome after Janssen COVID-19 vaccination: a case report and literature review. J Korean Med sci 36: e218.
- Thappy S, Thalappil S, Abbarh S, Abdulrahman A, Mohammed A, et al. (2021). Minimal change disease following the Moderna COVID-19 vaccine: first case report. BMC Nephrology 22: 376.