



Case Report - (2022) Volume 7, Issue 1
Cystic Adventitial Popliteal Disease: Personal Experience and Literature Review
Received Date: Feb 05, 2022 / Accepted Date: Feb 14, 2022 / Published Date: Feb 22, 2022
Copyright: ©Luca Garriboli, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Luca Garriboli, Claudia Fedelini, Tommaso Miccoli, Michele Bedetti, Gianguido Pruner. (2022). Cystic Adventitial Popliteal Disease: Personal Experience and Literature Review. Cardio Open, 7(1): 186-191.
Abstract
Background: Cystic adventitial disease (CAD) primarily affects arteries and is described as a rare vascular disorder characterized by fluid accumulation in the adventitial layer of a vessel which may cause luminal narrowing or even complete occlusion. Nowadays different pathogenetic theories exist as well as different treatment solution.
Case Report: We report two cases of cystic adventitial disease of the popliteal artery treated over the last 4 years in healthy men. Both experienced the sudden onset of intermittent calf claudication; one also presented blue toe syndrome. In both cases the diagnose was confirmed after open surgery and histological evaluation. Complete resection and autologous vein bypass were performed in one case; complete resection and direct end to end anastomosis in the others.
Discussion: Cystic adventitial disease is a rare vascular disorder with different interesting theories on its aetiology. Treatment options include percutaneous ultrasound-guided aspiration, endovascular approaches and open surgical cyst excision with or without direct reconstruction. In our Institution, we faced two popliteal CAD cases; open surgery represented the treatment strategy for both: in the first case an autologous vein bypass was performed, while in the second case the artery contiguity was restored with an end-to-end anastomosis. Both patients experienced full relief of symptoms without any recurrence of the disease.
Conclusion: Even if rare, popliteal artery CAD has to be suspected in young healthy patients who refer the sudden onset of acute or sub-acute symptoms related to peripheral arterial occlusive disease. Differential diagnose between popliteal entrapment syndrome and popliteal aneurysms is not always easy. When CAD is suspected or diagnosed a conventional surgical approach is recommended.
Keywords
Cyst, Disease, Popliteal Artery, Lower Leg Ischemia, Bypass
Introduction
Cystic adventitial disease (CAD) is a rare vascular disorder characterized by fluid accumulation in the adventitial layer of a vessel, which may cause narrowing or even complete occlusion of the lumen [1,2]. The cystic fluid has been described as gelat- inous or mucoid with a high content of hyaluronic acid and dif- ferent combinations of mucopolysaccharides and mucoproteins [1,3].
The first case of CAD was described in 1947 by Atkins and Key who reported a case of myxomatous tumour at the level of the external iliac artery [4]. This vascular disease primarily affects arteries; venous CAD is extremely rare and predominantly de- scribed at the level of the common femoral vein being an unusu- al cause of venous thrombosis [5].
Popliteal artery is the site where CAD is most frequently local- ized although external iliac, femoral and radial arteries are pos- sible sites of presentation [6,7]. Cystic adventitial disease of the popliteal artery is characterized by variety of symptoms similar to peripheral arterial occlusive disease; main differences are the absence of atherosclerotic risk factors and the age of their onset. Multiple techniques have been described for the treatment, with open surgical repair remaining the most successful one.
We report our experience in the treatment of cystic adventitial disease of popliteal artery describing two cases of surgical re- section and different methods of reconstruction, performing a reversed small saphenous vein bypass in one patient and a direct artery reconstruction in the others. We also describe the main pathogenetic theories of CAD, its management and the different suitable treatment options by reviewing articles published be- tween 2010 and March 2021 searched via PUBMED databases.
Case Report
Case 1: A healthy and active 56 years old man was referred to our institution because of 3-months history of intermittent claudication involving the left calf after a walking distance of 300 meters. During last 10 days he experienced the progressive worsening of the symptoms and the sudden appearance of cya-nosis of the homolateral big toe. The only atherosclerotic risk factor was smoking. The physical examination of the affected leg showed normal femoral pulse, no popliteal and distal puls- es and cyanosis of the big toe. All contralateral leg pulses were present.
Color Doppler ultrasonography (DUS) revealed at the site of popliteal artery a bilobed anechoic lesion completely inclosing the vessel wall. Contrast enhanced computed tomography (CT) showed compression of the left popliteal artery by a non-en- hancing structure, initially described as Baker’s cyst, associated with the complete thrombosis of the lumen of the artery and its re-habitation at the distal segment under the knee Figure 1.

Figure 1: Ultrasound imaging showing a bilobed anechoic le- sion compressing the left popliteal artery. Angio CT scan show- ing complete occlusion of the left popliteal artery and the cystic lesion in its place.
After a collegial consultation with radiologist and orthopedic colleagues, a suspicious diagnosis of CAD was advanced and surgical treatment was chosen. After obtaining patient’s in- formed consent the popliteal artery was exposed through a pos- terior approach via an S-shaped incision over the popliteal fossa. The mass was completely mobilized circumferentially revealing an apparent communication between the cyst and knee joint. Af- ter systemic heparinization (5000 IU of heparin sulphate) and clamping the popliteal artery was incised through a longitudi- nal arteriotomy: after the advential tunica incision the Authors observed the leaking of a gelatinous material that strongly con- firmed the diagnosis of CAD Figure 2
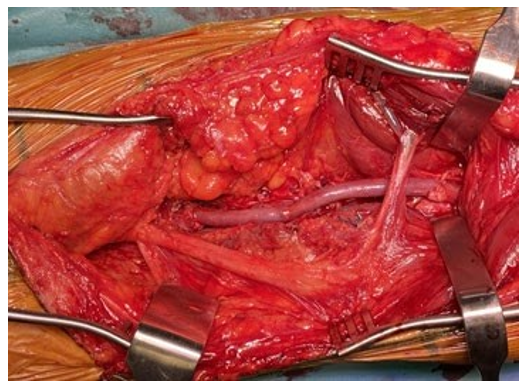
Figure 2: Mucoid material leaking out after incision of the ad- ventitial cyst.
The entire cyst was then resected and a segment of patient’s homolateral small saphenous vein was interposed in a reverse fashion Figure 3 the blood flow was restored with the recovery of all distal arterial pulses. The patient made an uneventful re- covery and was discharged on the third post-operative day with-out any complication. Single antiplatelet therapy was prescribed (100 mg/die of acetylsalicylic acid). DUS examination before discharge showed normal triphasic Doppler waveform through the left popliteal artery without anastomotic defects; histological examination of artery’s segment defined its content as “amor- phous material”, excluding any oncological disease.

Figure 3: Popliteal artery replaced with reversed small saphe-nous vein interposition.
The 1-month follow up Duplex ultrasound exam showed good patency of the vein graft and the absence of cyst recurrence. Fur- thermore, the patient experienced fully relief of symptoms; the big toe recovered normal color, temperature and sensibility few days afterwards.
Case 2: A 64 years old sportsman was admitted to our institution with 1-month history of left calf intermittent claudication. Phys- ical examination revealed only a good left femoral pulse. Color Doppler ultrasonography showed sudden focal occlusion of a dilatated popliteal artery with poorly detectable distal flow. Hy- pertension was the only atherosclerotic risk factor. Patient un- derwent digital subtraction angiography (DSA) which showed perfect patency of all below the knee vessels and the “scimitar sign” at the popliteal level Figure 4.
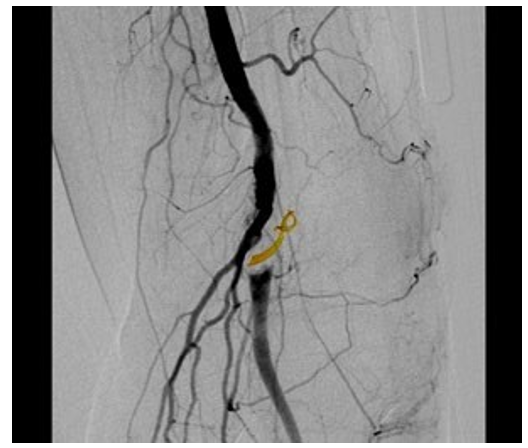
Figure 4: Angiography showing the typical curvilinear scimitar sign due to extrinsic compression of the lumen.
In the suspect of a non-atherosclerotic popliteal disease an MRI was then preoperatively performed. T2 weighted sequences showed a fluid aspect inside popliteal artery confirming CAD diagnosis. An open surgical repair through an S-shaped poste- rior incision over the popliteal fossa was chosen. The patient was systemically heparinized (5000 IU of heparin sulphate), the diseased popliteal artery segment was resected, and the vessel continuity was restored through an end-to end 6/0 prolene suture Figure 5. Patient totally recovered from the symptoms and was discharged on second post-operative day with single antiplate- let therapy (Clopidogrel 75 mg/die). The 3- months follow-up revealed no limb pain and a normal walking distance. The 24 months follow-up Duplex ultrasound showed no signs of recur- rence or restenosis. Histological evaluation showed fibroscle- rosis of the vessel wall associated with areas of old and fresh haemorrhage.
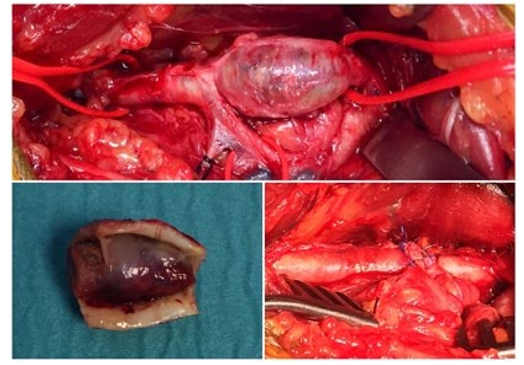
Figure 5: Resected segment of affected popliteal artery with te- nacious mucoid material coming from the adventitial cyst. End to end anastomosis to restore the arterial continuity.
Discussion
Adventitial cystic disease is a rare cause of claudication as rare is the pathology itself. It should be suspected in patients with no or minimal cardiovascular risk factors, with a reported male-to-fe- male ratio of approximately 5:1 and mean age of onset between 40 and 50 years [1,2,8]. In our study series mean age at diagno- sis was 51 years (Range 5-87) with a prevalence in males (M= 90; 76,9%; male-to female ratio 10:3) in Table 1. Because of its rarity, prevalence of CAD is unknown, but it is estimated that CAD accounts for <0.1% of cases of intermittent claudication [1]. A multicentric experience coming from fourteen different institutions, describes an average number of cases per institution of 3 over a period of 10 years, which is in line with our data [3].
Table 1: Patient Demographics
|
Patients (N, %) |
117 |
|
90 (76,9 %) |
|
27 (23,1%) |
|
Mean age |
51 y (Range 5-87) |
|
Presenting symptoms (N, %) |
|
|
104 (89%) |
|
6 (5%) |
|
3 (2,6%) |
|
2 (2%) |
|
1 (0,7%) |
|
1 (0,7%) |
Aetiology
When it comes to the definition of its origin, different theories can be postulated: the trauma theory, the systemic disorder the- ory, the synovial theory and the developmental theory. The trau- matic theory suggests that multiple (micro) traumas due to ana- tomical position of the popliteal artery could be responsible for the degeneration of its wall. The systemic disorder theory con- siders the cystic degeneration of the popliteal artery as part of a generalized disorder involving connective tissue [9]. Because of the histological and biochemical similarity between adventitial cyst and ganglia, the synovial theory suggests a possible origin of the former from the capsular synovial structures that eventu- ally enlarge and involve the adventitia of adjacent vessel [10,11]. Finally, the developmental theory suggests mucin secreting cells becoming incorporated into the vessel wall during embryologi- cal development [12,13]. This could support the evidence of an apparent communication between artery and adjacent joint, fre- quently identified intraoperatively.
The most unifying theory however comes from Levien et al ac- cording to whom CAD is caused by the incorporation of mes- enchymal cells, that normally are destined to joint tissue, into the developing of non-axial vessel approximately during the 10-22th week of embryological development [14]. These cells would later be responsible of the production of mucoid material.
Clinical Presentation
The most common symptom of popliteal artery CAD is inter- mittent claudication of the lower extremity: the onset is usually acute and can rapidly progress. Other presenting symptoms can be burning pain and paraesthesia of the affected lower extremity, pain behind the knee, acute calf pain, cyst rupture (rarely), isch- emic rest pain and occasionally deep vein thrombosis also [1-3]. In those series the most frequent presenting symptom was calf intermittent claudication (89% of the total), followed by burning pain and paraesthesia (5%), pain behind the knee (2,6%), rest pain (2%), acute limb pain (0,7%) and one case of deep vein thrombosis (0,7%) Table 1.
Diagnosis
No diagnostic criteria have been standardized for CAD: clinical examination, paying attention to absence of risk factors, mean age, sudden as well as rapidly progressive symptoms and duplex ultrasound have to be considered as the first level exams. When popliteal artery appears totally occluded, as described in our cas- es, it is difficult to differentiate between entrapment syndrome, popliteal artery aneurysms or popliteal cysts using only duplex ultrasound. In these cases, CT and MRI may help: MRI, thanks to 3D reconstruction, may allow to recognize the cystic nature of the lesion and may show the connection between the adventitial cyst and the adjacent joint capsule appearing the cyst’s fluid as a high signal intensity on T2-weighted images [15,16]. Current- ly angiography is no more considered diagnostic However, it should be considered a useful completion exam to preoperative planning: for example, the evidence of the “scimitar sign”, due to displacement of the artery to one side, provides further sup- port to the diagnosis of CAD.
Treatment
Treatment options of CAD include percutaneous ultra- sound-guided aspiration, endovascular approach with percuta- neous transluminal balloon angioplasty (PTA) and open surgi- cal cyst excision with patch interposition or bypass grafting; in this case the use of the autologous veins is recommended when available. The surgical approach strongly depends on clinical symptoms and radiological findings; however, it should be rec- ommended even if the diagnosis is not certain. The main goals of the surgical procedure are to remove the mass from popliteal fossa in order to have a certain histological examination and, as in our case, to restore arterial patency preventing progression of symptoms.
The cyst excision is by far the most widely reported surgical treatment: removal of the cyst content allows lumen to return to its regular diameter. Success rates range from 85% to 94% with failure often due to cyst recurrence [17,18]. The second most reported technique is surgical excision of the pathological artery segment with interposition of venous or prosthetic graft. Suc- cess rates between 93.5%-95% are reported for this procedure; among patients treated with resection of the artery and bypass grafting, the use of autologous vein reported better results com- pared to prosthetic graft [19,20].
The percutaneous cyst aspiration, not always practicable due to viscosity of the cyst content or the presence of multilocular cysts, shows little success; a high recurrence rate is caused by the re-accumulation of fluid or its incomplete aspiration [21,22]. Percutaneous endovascular procedures using angioplasty or stenting initially aroused enthusiasm for the treatment of these lesions. However, considering the poor results mainly due to the nature of the disease that is extraluminal and not atherosclerotic, it has progressively abandoned [23-26].
Table 2 provides an overview of popliteal CAD cases published on PubMed between 2010 and March 2021. In the Study se- ries a total of 117 procedures were described: among surgical techniques cyst resection, with or without bypass interposition, was the most performed technique. Open surgical treatment was performed in 103 of 117 patients (89%); the remaining four- teen patients underwent US guided percutaneous cyst aspiration (n=7; 6%), observation (n=4; 3,4%) or percutaneous angioplas- ty/stenting (n=3; 2,6%).
Table 2: Published cases between 2010 e 2021 searched via Pubmed databases
|
|
Total Cases |
Success |
Failure |
Comments |
|
Arterial segment resection and vein reconstruction |
28 |
27 |
1 |
|
|
US-guided percutaneous cyst aspiration |
7 |
4 |
3 |
|
|
Arterial segment resection and synthetic graft reconstruction |
30 |
29 |
1 |
|
|
Angioplasty/ Stenting (BMS) |
3 |
3 |
- |
|
|
Arterial segment resection and primary anastomosis |
28 |
15 |
3 |
|
|
Cyst excision |
10 |
8 |
2 |
|
|
+ patch closure |
6 |
6 |
- |
|
|
Arterial segment resection and criopre- served arterial graft reconstruction |
1 |
1 |
- |
|
|
Observation |
4 |
3 |
1 |
|
|
Total |
117 |
106 |
11 |
|
The choice to use or not graft interposition largely depended on individual anatomical characteristics. When available, tendency was to use autologous great or small saphenous vein (1/28 rest- enosis), however good results were achieved also using pros- thetic grafts (only one bypass occlusion after 6 years over thirty performed). Recurrence of the cyst was observed in three pa- tients treated with US guided percutaneous cyst aspiration (3/7), in two patients undergoing simple cyst excision (2/10), and in one case of arterial segment resection and primary anastomosis reconstruction (1/10). In this last surgical group also two rest- enosis occurred (2/10). Three patients treated with angioplasty were asymptomatic after 45, 51, and 117 months respectively, no failures were observed in this group. Among patients treated with simple medical therapy one of them developed acute limb ischemia after three months (1/4).
In our institution we experienced two cases of CAD at popli- teal artery; the treatment was surgical for both patience, in fact we performed the complete excision of the diseased segment in both cases. In one case the artery contiguity was restored with an end-to-end anastomosis thanks to the limited area involved; in the other one an autologous vein bypass was necessary. Both cases experienced fully relief of symptoms without recurrence of cystic adventitial disease.
Highlights
• Cystic adventitial disease is a rare vascular disorder char- acterized by fluid accumulation in the adventitial layer of an artery.
• Cystic adventitial disease may cause luminal narrowing or even complete arterial occlusion.
• Cystic adventitial disease has to be suspected in young healthy patients who refer to acute or sub-acute symptoms of peripheral arterial occlusive disease.
• A conventional surgical approach through open cyst exci- sion and direct or indirect reconstruction remain the treat- ments of choice.
Conclusion
Even if rare, CAD has to be suspected in young patients who refer sudden manifestation of progressive claudication or acute limb ischemia with no or few cardiovascular risk factors. When suspected at Duplex ultrasound it should be always mandatory performing a second level exam in order to confirm the diagno- sis and planning the strategy of the treatment. Considering the nature of the disease, in our experience conventional surgical approach through arterial segment resection and direct recon- struction or bypass grafting remains the treatment of choice.
References
- Del Canto Peruyera, P., Vázquez, M. V. V., Velasco, M. B., Álvarez, P. C., Salgado, A. Á., & et al. (2015). Cystic adven- titial disease of the popliteal artery: two case reports and a review of the literature. Vascular, 23(2), 204-210.
- Paravastu, S. C., Regi, J. M., Turner, D. R., & Gaines, P. A. (2012). A contemporary review of cystic adventitial disease. Vascular and endovascular surgery, 46(1), 5-14.
- Motaganahalli, R. L., Smeds, M. R., Harlander-Locke, M. P., Lawrence, P. F., Fujimura, N., & et al. (2017). A multi-in- stitutional experience in adventitial cystic disease. Journal of vascular surgery, 65(1), 157-161.
- Atkins, H. J. B., & Key, J. A. (1947). A case of myxomatous tumour arising in the adventitia of the left external iliac ar- tery. Journal of British Surgery, 34(136), 426-427.
- Dix, F. P., McDonald, M., Obomighie, J., Chalmers, N., Thompson, D., & et al. (2006). Cystic adventitial disease of the femoral vein presenting as deep vein thrombosis: a case report and review of the literature. Journal of vascular surgery, 44(4), 871-874.
- Hildreth, D. H. (1975). Cystic adventitial disease of the common femoral artery. The American Journal of Surgery, 130(1), 92-96.
- Bäckström, C. G., Linell, F., & Ostberg, G. (1965). Cystic, myxomatous adventitial degeneration of the radial artery with development of ganglion in the connective tissue; re- port of two cases. Acta chirurgica Scandinavica, 129, 447- 451.
- Jarraya, M., Simmons, S., Farber, A., Teytelboym, O., Nag- gara, N., & et al. (2016). Uncommon diseases of the pop-liteal artery: a pictorial review. Insights into imaging, 7(5), 679-688.
- Linquette, M., Mesmacque, R., Beghin, B., Hubschman, B., & Soots, G. (1967). Degenere scence kystique de l’adven- tite de l’artere poplitee. Semaine Hop Paris, 43, 3005-3013.
- Bergan JJ. (1995). Adventitial cystic disease of the popliteal artery. In: Rutherford RB, editor. Vascular surgery, 883-888.
- Devereux, D., Forrest, H., McLeod, T., & Ahweng, A. (1980). The nonarterial origin of cystic adventitial disease of the popliteal artery in two patients. Surgery, 88(5), 723- 727.
- Haid, S. P., Conn, J., & Bergan, J. J. (1970). Cystic adven- titial disease of the popliteal artery. Archives of Surgery, 101(6), 765-770.
- Shute, K., & Rothnie, N. G. (1973). The aetiology of cystic arterial disease. Journal of British Surgery, 60(5), 397-400.
- Levien, L. J., & Benn, C. A. (1998). Adventitial cystic dis- ease: a unifying hypothesis. Journal of vascular surgery, 28(2), 193-205.
- Michaelides, M., Pervana, S., Sotiridadis, C., & Tsitouridis,I. (2011). Cystic adventitial disease of the popliteal artery. Diagnostic and Interventional Radiology, 17(2), 166-168.
- Peterson, J. J., Kransdorf, M. J., Bancroft, L. W., & Mur- phey, M. D. (2003). Imaging characteristics of cystic ad- ventitial disease of the peripheral arteries: presentation as soft-tissue masses. American Journal of Roentgenology, 180(3), 621-625.
- Kim, H. K., Choi, H. H., & Huh, S. (2012). Cystic adven- titial disease of the popliteal artery: a recurrent case after cyst wall excision. International Angiology: a Journal of the International Union of Angiology, 31(2), 198-201.
- Tsolakis, I. A., Walvatne, C. S., & Caldwell, M. D. (1998). Cystic adventitial disease of the popliteal artery: diagnosis and treatment. European journal of vascular and endovascu- lar surgery, 15(3), 188-194.
- Drac, P., Köcher, M., Utikal, P., Cerna, M., Kozak, J., & Bachleda, P. (2011). Cystic adventitial disease of the popli- teal artery: report on three cases and review of the literature. Biomedical Papers of the Medical Faculty of Palacky Uni- versity in Olomouc, 155(4), 309-321.
- Baxter, A. R., Garg, K., Lamparello, P. J., Mussa, F. F., Cayne, N. S., & et al. (2011). Cystic adventitial disease of the popliteal artery: is there a consensus in management?. Vascular, 19(3), 163-166.
- Do, D. D., Braunschweig, M., Baumgartner, I., Furrer, M., & Mahler, F. (1997). Adventitial cystic disease of the popli- teal artery: percutaneous US-guided aspiration. Radiology, 203(3), 743-746.
- Colombier, D., Elias, A., Rousseau, H., Otal, P., Leger, P., & et al. (1997). Cystic adventitial disease: importance of com- puted tomography in the diagnostic and therapeutic man- agement. Journal des Maladies Vasculaires, 22(3), 181-186.
- Maged, I. M., Kron, I. L., & Hagspiel, K. D. (2009). Re- current cystic adventitial disease of the popliteal artery: successful treatment with percutaneous transluminal angio- plasty. Vascular and endovascular surgery, 43(4), 399-402.
- Rai, S., Davies, R. S., & Vohra, R. K. (2009). Failure of endovascular stenting for popliteal cystic disease. Annals of Vascular Surgery, 23(3), 410-e5.
- Fox, R. L., Kahn, M., Adler, J., Sussman, B., Mendes, D., & et al. (1985). Adventitial cystic disease of the popliteal artery: failure of percutaneous transluminal angioplasty as a therapeutic modality. Journal of vascular surgery, 2(3), 464- 467.
- Patel, S. M., Patil, V. A., & Pamoukian, V. N. (2008). Inter- position grafting of popliteal artery cystic adventitial dis- ease: case report. Vascular and endovascular surgery, 42(2), 192-195.