
COVID Research: Open Access(CROA)
ISSN: 2995-7826 | DOI: 10.33140/CROA


Research Article - (2024) Volume 2, Issue 2
Covid-19 Vaccination Prevents Functional Loss in Elderly
2Secretaria de Salud de Nuevo Leon, Geriatric Service, Hospital, Metropolitano, San Nicolas de los Garza, Nuevo Leon, Mexico
Received Date: Jun 25, 2024 / Accepted Date: Jul 22, 2024 / Published Date: Jul 31, 2024
Copyright: ©©2024 Jose De Jesus, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Gutierrez, M., De Jesus, J., Ramos, G., Ariel, A., Quintanilla, R. et al. (2024). Covid-19 Vaccination Prevents Functional Loss in Elderly. COVID Res OA, 2(2), 01-08.
Abstract
Background: COVID-19 caused high morbidity among persons 65 years and older. It is known that the disease reduces the independencies of a patient. SARS-CoV2 vaccination significantly reduced the severity of cases, hospitalizations, and mortality, especially in older people. Is vaccination preserving functional performance in older adults?
Methods: This study conducted in a COVID-19 concentration hospital in North Mexico. Patients 60 years and older, who were hospitalized and tested positive for SARS-CoV-2 between March 1 and October 31, 2021 were included. Participants were categorized based on their vaccination status upon admission and a 6-month follow-up phone call. The study examined functional performance assessing daily life activities using Katz index and Lawton Brody Scale.
Results: A total of 266 patients with an average age was 74 years. Regarding vaccination status, 40% were not immunized, and 31.4% had completed their immunization schedule. The analysis revealed that any immunization status significantly preserved IADL, with the highest level of protection observed in complete immunization status (p<0.001; OR 0.05, 95% CI 0.01-0.18). The former doesn’t apply for ADL performance since only complete vaccination status resulted protective (p=0.008; OR 0.26, 95% CI 0.09-0.71).
Conclusion: The key finding: even incomplete vaccinations prevent functional loss in the elderly, but a complete status confers maximum protection. Our study underscores the need to remove barriers hindering elderly vaccination.
Keywords
Older Adults, Elderly, Covid-19, Sars-Cov2 Vaccine, Covid-19 Vaccination, Dependence, Functional Performance
Abbreviations
COVID-19 - The Coronavirus Disease 2019
SARS-CoV-2 - Severe Acute Respiratory Syndrome Coronavirus
2 ADL - Activities of Daily Living
BADL - Basic Activities of Daily Living
IADL - Instrumental Activities of Daily Living
RNA - Ribonucleic acid
RT-PCR - Reverse Transcriptase Polymerase Chain Reaction qCSI - Quick COVID-19 Severity Index AUC - Area Under the Curve
GCA - Geriatric Comprehensive Assessment
PHQ - Patient Health Questionnaire
MNA-SF - Mini Nutritional Assessment Short Form
Introduction
The coronavirus disease 2019 (COVID-19) started in Wuhan, China, by the end of 2019 [1]. By March 11, 2020, it had become the first pandemic of the 21st century [2]. Once inhaled this 120-nanometer particle with a single-stranded ribonucleic acid (RNA) genome causes a severe inflammatory response in the body, contributing to its clinical presentation [3-5]. Although initially described as a respiratory disease, COVID-19 has implications beyond the respiratory system, affecting almost every system in the body [6].
Multiple risk factors contribute to the spread of COVID-19, but preventive measures such as social distancing, mask-wearing, and increased hygiene practices helped curb the outbreak [7,8]. However, even with these measures, the pandemic persisted. COVID-19 disproportionately affects older people worldwide. This age group is more likely to develop severe illness and die [9]. The mortality rate for adults over 80 years was 15%, and 8-10% for those aged 70-79 years [10-12]. Before the implementation of vaccines, eight out of ten COVID-19 deaths occurred in patients over 65 years [13]. Initially, treatment for COVID-19 consisted in supportive measures [14]. Treatment options improved once the disease became understood [15,16].
Vaccination became the breakthrough of the pandemic. Margaret Keenan, a 90-year-old woman, became the first person to receive the vaccine [17]. The impact of COVID-19 vaccination has been substantial, approximately 1.1 billion cases, 400 million hospitalizations, and 100 million deaths globally prevented by November 2021 [18-20]. However, the impact of vaccination varied widely depending on the vaccination coverage achieved in each country, the patient’s comorbidities, and the burden of disease [9], [21,22]. In older adults, conditions like functional dependency, cognitive decline, depression, and frailty are more prevalent, conditioning to a worst outcome for COVID-19 [23- 25]. Studies in France and Spain have found that COVID-19 vaccination is associated with a significant reduction in healthcare attention needed among elderly individuals, including nursing, rehabilitation and hospitalization for any cause [26,27]. This study aims to analyses whether the immunization status before hospital admission for COVID-19 is associated with changes in functional performants in DLA in elderly patients.
Materials and Methods
This work was conducted in a concentration hospital for COVID-19 patients during the critical phases of the pandemic. This center is a second-level hospital in North Mexico. The ethics committee of the Hospital Metropolitan, part of the healthcare network under the State Health Department approved the protocol (Registration number DEISC-19 01 22 023). Informed consent was obtained from all participants.
This is an exploratory, observational, cross-sectional and prospective research. The participants were 60 years and above, hospitalized for COVID-19 with a positive result on the reverse transcriptase polymerase chain reaction (RT-PCR) test between March 1 and October 31, 2021. The timeframe ensures the inclusion of patients with different vaccination statuses, as the vaccination program in Mexico began in December 2020 [28]. In addition, participants were discharged from the Internal Medicine/Geriatrics Service. Patients not located for follow-up were excluded.
The participants were grouped based on their vaccination status at admission, regardless of the type of vaccine received. Data were collected form electronic records. The data included background and medical history, including vaccination status (brand, doses, and application dates), clinical presentation, and COVID-19 RT-PCR test results.
We used the Quick COVID-19 Severity Index (qCSI) for grading disease status. This index predicts the progression of respiratory failure within 24 hours (AUC 0.81; 95% CI 0.73-0.89) using the initial respiratory rate, oxygen saturation and supplemental oxygen requirement (in litters per minute) at presentation [29- 32].
A Geriatric Comprehensive Assessment (GCA) which included functional assessment, using the Katz index for Basic Activities of Daily Living (BADL) which include performance in bathing, dressing, toileting, transfer, continence and feeding and Lawton & Brody for Instrumental Activities of Daily Living (IADL) including preparing meals, housekeeping and laundry, managing medications and finances, shopping, using transportation and telephone [33,34]. In cases where the functional status wasn’t available in the medical records, the researchers used phone calls to retrieve the information using validated instruments [35,36].
The GCA included a Gijon Scale adaptation to screen for socio- familial situations. Cognitive screen using memory complaints, and if positive, Mini-Cog test was performed. Depression was the only mood pathology screened using the Patient Health Questionnaire (PHQ). We used the Mini Nutritional Assessment Short Form (MNA-SF) for nutritional screening and the FRAIL tool for Frailty. We also asked about pressure sores and sensory deficits.
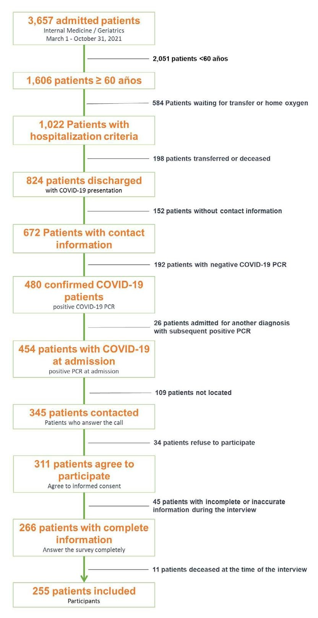
Figure 1: Flow of Patients
We conducted a 6-month phone call follow-up assessing changes in participants’ basal state. The primary endpoint was to determine whether vaccination status before hospital admission due to COVID-19 in adults aged 60 years or older changes the performance in BADL and IADL. The secondary objective describes changes in COVID-19 immunization schedule. We also compared the COVID-19 severity, mortality at discharge, and time to outof-hospital death. All the aforementioned were analysed according to the vaccination status.
A pilot study was conducted demonstrating that the survey was feasible, reliable and effective for the purpose of the study and despite time spent for the interview patients accepted it well. Due to the exploratory nature of this study, the sample size depended on the number of discharges from the Internal Medicine / Geriatrics Service of patients aged 60 years or older with a positive COVID-19 RT-PCR test result from March 1 to October 31, 2021.
Variables distribution was assessed using the Kolmogorov- Smirnov test. Categorical variables were compared using the chi-square or Fisher’s exact tests. For quantitative variables the MannWhitney, independent samples t-test or KruskalWallis test were used depending on the number of groups compared. To analyse non-parametric correlations The Spearman correlation coefficient was used. Alogistic regression analysis was performed to identify factors associated with worsening ACDLs. Possible confounders between variables were assessed, < 0.1 p-value was the threshold significance of confounders’ associations. And a p-value < 0.05 and a 95% confidence interval defined for statistical significance. SPSS (version 25) software (IBM Inc.) were used.
Results
266 patients were included, Figure 1. 255 (95.9%) survived, 11 (4.1%) patients died at the time of follow-up, those patients had a higher median hospital stay of 107 vs. 12 days, p<0.001, and a higher frequency of severe illness 81.8% vs. 42.4%, p=0.011. The median survival time was 86 days (22-138 days) after hospital discharge. The mean age was 74 yr, with 124 (48.6%) women. The median number of comorbidities was 1, with 75% of patients having between 1 and 2 comorbidities. Only one patient had no comorbidities, while the maximum number was 7. Regarding vaccine status, 102 (40%) patients were not immunized, 61 (23.9%) had an incomplete vaccination schedule, 80 (31.4%) had a complete immunization schedule, and 12 (4.7%) received a booster dose. We decided to count the few boostered patients in the complete vaccination schedule group. According to the qCSI, 57.6% of patients had a moderate illness, while 42.4% had severe disease. The median hospital stay was 12 days, with 75% of patients having a hospital stay between 8 and 15 days, ranging from 6 to 62 days. Table 1. Lack of vaccination was associated with more comorbidities (p=0.001).
Table 1: Basic Demographic and Clinical Characteristics at Hospital Admission
|
Characteristics of the Patients at Baseline. |
||
|
Variable |
Category |
n (%) |
|
Age(years) |
74 ± 9.1 |
|
|
Marital status |
Male |
131 (51.4%) |
|
Female |
124 (48.6%) |
|
|
Number of comorbidities* |
1 (1 - 2) |
|
|
|
Non-vaccinatedChrysler |
102 (40 %) |
|
Vaccination status |
Incomplete Complete |
61 (23.9%) 92 (36.1%) |
|
COVID-19 severity ** |
Moderate (qCSI 4 - 9) |
147 (57.6%) |
|
Moderate (qCSI >9) |
108 (42.4%) |
|
|
Hospital stay (days)* |
12 (8 -15) |
|
|
* Median (IQR 25% - 75% ** Quick COVID-19 Severity Index |
||
Table 2 shows the patients’ demographic characteristics distribution and clinical characteristics. The follow-up was at 6.5 ± 1.2 months.
Table 2: Variable Distribution by Vaccination Status Group
|
Patients’ characteristics according immunization status. |
||||
|
Variable |
Non-vaccinated |
Incomplete |
Complete |
p |
|
Patients |
102 |
61 |
92 |
|
|
Age(years) |
73.5 ± 8.3 |
74.2 ± 9.8 |
74.4 ± 9.6 |
|
|
Gender |
|
0.508 |
||
|
- Female |
48 (47.1%) |
27 (44.3%) |
49 (53.3%) |
|
|
- Male |
54 (52.9%) |
34 (55.7%) |
43 (46.7%) |
|
|
Num. of comorbidities* |
2 (1 - 2) |
2 (1 - 2) |
2 (1 - 2) |
0.001 |
|
Hospital stay (days)* |
12 (8 - 16) |
12 (8 - 15) |
11 (8 - 14) |
0.507 |
|
Severity ** |
|
0.363 |
||
|
- Moderate |
54 (52.9%) |
35 (57.4%) |
58 (63%) |
|
|
- Severe |
48 (47.1%) |
26 (42.6%) |
34 (37%) |
|
|
Follow-up (months) |
6.7 ± 1.4 |
6.8 ± 1.5 |
6.2 ± 0.6 |
0.001 |
|
* Median, IQR (25% - 75%) ** cQSI = Quick COVID-19 Severity Index |
||||
Illness severity was not associated with the number of comorbidities, prior vaccination status, or independence in activities of daily living before admission. Severe cases had prolonged hospital stays (median 16 vs. 9 days, p<0.001). The number of comorbidities did not correlate with the number of days of hospital stay (Spearman’s rho = -0.053, p=0.401).
Unvaccinated patients more frequently stopped working (p<0.001) and gave up recreational activities (p<0.001). A higher percentage of patients with a complete or a booster schedule had no sequelae (77.2%) compared to those with an incomplete scheme (29.5%) and unvaccinated (33.3%) (p<0.001).
Comparing the number of ADL, for BADL the Katz scale before admission with those performed at the time of the interview, 7 (2.7%) showed improvement, 214 (83.9%) did not show any changes, and 34 (13.3%) decreased the number of activities they performed independently. For those who had poorer performance the median lost activities were 3 (1-3). Using the Lawton & Brody scale to compare IADLs before admission and at the interview, 191 (74.9%) showed no changes, while 64 (25.1%) decreased the number of independent activities. For the group that worsened, the decreased activities had a median of 2 (1-4) Table 3.
Table 3: Changes in Performance of Activities of Daily Life and Number of Activities Lost.
|
Changes in ADL |
||||
|
|
Performance |
Activities lost |
||
|
Activities |
No change |
Worse |
Improved |
|
|
Katz Indez (BADL)* |
214 (83.9%) |
34 (13.3%) |
7 (2.7%) |
3 (1 - 3) |
|
Lawton-Brody scale (IADL)* |
191 (74.9%) |
64 (25.1%) |
0 |
2 (1 - 4) |
|
* Median, IQR (25% - 75%) |
||||
Vaccination status had a statistically significance for daily life activities performance (BADL p=0.002 / IADL p<0.001). Patients with a complete status lost less independence in ADL, with a greater loss for IADL (p <0.001) in comparation with BADL (p=0.002), as shown in Table 4. In contrast non, vaccinated patients performed fewer BADLs after hospital discharge (p=0.032) and this group lost more activities than those vaccinated regarding the status (p=0.026).
Table 4: Statistical Analysis for ADL According to the Vaccination Status After and Before Covid-19.
|
Performance in ADL according to the vaccination status |
|
|
Katz Index |
|
|
Variable No-vaccinated Incomplete Complete |
p |
|
Pre COVID-19* 6 (6 - 6) 6 (6 - 6) 6 (6 - 6) |
0.507 |
|
POST COVID-19* 6 (5 - 6) 6 (6 - 6) 6 (6 - 6) |
0.032 |
|
- Improved 0 2 (3.3%) 5 (5.4%) - No change 79 (77.5%) 53 (86.9%) 82 (89.1%) - Worse 23 (22.5%) 6 (9.8%) 5 (5.4%) |
0.002 |
|
|
|
|
|
|
<0.001 0.026 |
|
|
Lawton-Braody scale |
|
|
Variable No-vaccinated Incomplete Complete |
p |
|
Pre COVID-19* 5 (5 - 8) 8 (7 - 8) 4 (3 - 6) |
<0.001 |
|
POST COVID-19* 4 (3 - 6) 8 (6 - 8) 4 (3 - 6) |
<0.001 |
|
- Improved 0 0 0 - No change 49 (48%) 53 (86.9%) 89 (96.7%) - Worse 53 (52%) 8 (13.1%) 3 (3.3%) |
<0.001 |
|
|
|
|
- Overall 1 (0 -2) 0 0 - Patients with poorest performace* 2 (2-4) 2 (1-6) 1 (1-1) |
|
|
<0.001 0.719 |
|
|
* Median, IQR (25% - 75%) |
|
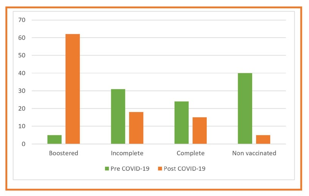
Figure 2: Changes in vaccination status
Changes in the COVID-19 vaccination schedule, Figure 2, were substantial and suffered dramatic improving coverage at the follow-up.We conducted a logistic regression analysis comparing patients who worsened with those who had no changes in DLA, trying to identify factors associated with worst scores in Katz index and Lawton-Brody scale.The univariate analysis showed that immunization maintains IADLs. The best protection seen with a complete immunization status (p<0.001; OR 0.05, 95% CI 0.01-0.18), Table 5.
Table 5: This Table Presents the Results of the Univariate and Multivariate Analysis of Factors Associated with Impairment in IDLA among older Adults.
|
Factors associated with instrumental activities of daily life deterioration |
||||||
|
|
|
Multivariable |
||||
|
|
Univariable |
|
Model 1 |
|
Model 2 |
|
|
Variable |
p |
OR |
p |
OR |
p |
OR |
|
Age ≥ 75yr |
0.859 |
0.95 (0.53-1.68) |
0.771 |
0.89 (0.42-1.88) |
- |
- |
|
Male |
0.159 |
0.66 (0.37-1.17) |
0.02 |
0.42 (0.20-0.87) |
- |
- |
|
Married |
0.901 |
0.96 (0.53-1.73) |
0.651 |
1.19 (0.55-2.59) |
- |
- |
|
Comorbidities ≥ 2 |
0.773 |
0.89 (0.43-1.84) |
0.107 |
0.47 (0.19-1.17) |
- |
- |
|
Hospital stay ≥ 10days |
0.155 |
1.53 (0.84-2.76) |
0.998 |
1.001 (0.35-2.84) |
- |
- |
|
Severe COVID-19 |
0.085 |
0.60 (0.34-1.07) |
0.600 |
0.6 (0.22-1.62) |
0.232 |
0.66 (0.34-1.29) |
|
Complete vaccination |
<0.001 |
0.05 (0.01-0.18) |
<0.001 |
0.02 (0.007-0.08) |
<0.001 |
0.032 (0.009-0.107) |
|
Incomplete vaccination |
0.016 |
0.37 (0.16-0.83) |
<0.001 |
0.12 (0.05-0.29) |
<0.001 |
0.14 (0.06-0.32) |
|
For Model 1 all vasiables were included in the analysis Model 2 only statistically significant variables for Model 1 er included |
||||||
Complete immunization was also a protective factor for losing ADLs by Katz (p=0.008; OR 0.26, 95% CI 0.09-0.71). However, incomplete immunization status unlike IADLs (p=0.36) didn’t reflect protection for BADLs, Table 6.
Table 6: This Table Presents the Results of the Univariate and Multivariate Analysis af Factors Associated with Impairment in BDLA among older Adults.
|
Factors associated with basic daily life activities impairment |
||||||
|
Variable |
Univariable Multivariable |
|||||
|
Age ≥ 75yr |
0.385 |
1.37 |
(0.66-2.83) |
0.434 |
1.39 |
(0.60-3.19) |
|
Male |
0.363 |
0.71 |
(0.34-1.47) |
0.151 |
0.56 |
(0.25-1.23) |
|
Married |
0.7 |
1.16 |
(0.53-2.51) |
0.743 |
1.16 |
(0.47-2.81) |
|
Comorbidities ≥ 2 |
0.197 |
0.49 |
(0.16-1.47) |
0.068 |
0.33 |
(0.10-1.08) |
|
Hospital stay ≥ 10days |
0.397 |
1.38 |
(0.65-2.93) |
0.86 |
0.89 |
(0.25-3.13) |
|
Severe COVID-19 |
0.18 |
0.61 |
(0.29-1.26) |
0.327 |
0.55 |
(0.16-1.82) |
|
Complete vaccination |
0.008 |
0.26 |
(0.09-0.71) |
0.001 |
0.17 |
(0.06-0.49) |
|
Incomplete vaccination |
0.36 |
0.64 |
(0.25-1.64) |
0.03 |
0.33 |
(0.12-0.90) |
|
For Model 1 all vasiables were included in the analysis Model 2 only statistically significant variables for Model 1 er included |
||||||
Age, gender, marital status, number of comorbidities, length of hospital stays, and severity of illness weren´t predictors of worsening in ADLs. We included all the mentioned variables in a multivariate analysis to predict promoters’ worsening in Katz and Lawton-Brody scores. Immunization, regardless of whether it is complete or not, is a factor that predicts functional preservation.
Discussion
It is well-known that hospitalization, regardless of the cause, leads to functional deterioration in the elderly. COVID-19, particularly in the elderly population, results in severe outcomes, including symptoms, admissions, hospital stays, increased disease severity, convalescence challenges, complications, and higher mortality rates. Hospitalization due to COVID-19 in older adults is anticipated to result in significant functional decline. Some authors have documented functional deterioration in older patients with COVID19. However, there is limited information available about the protective aspects of the SARS-CoV-2 vaccine on elderly functionality. This research investigates the preservation of functionality in the elderly based on their vaccination status. The study hypothesized that a complete vaccine schedule can have protective effects, what was corroborated in this work. Remarkably, it was found that even incomplete vaccination offers protection against functional loss in the elderly. Therefore, it can be concluded that SARS-CoV-2 vaccination plays a role in preventing dependency in COVID-19 cases.
Conclusion
Decreased mortality, severity, hospital stay, and complications are some benefits of vaccination in the elderly. Studies assessing functional dependency, COVID19 and vaccination are scare. Most studies compare symptoms, severity, and infection resolution between functionally dependent and independent geriatric patients [37]. This study compared functional loss according to the vaccination status of geriatric patients. The main finding of this research is that vaccination, even an incomplete scheme, prevents functional loss in the elderly. COVID-19 vaccination in adults over 60 yr depends on some determinants [38,39]. Our findings suggest breaking down the barriers to vaccination in older adults.
Limitations
The present study had several limitations. The timeframe makes this study hard to replicate. The study included critical patients at the internal medicine / geriatric yard but not at the intensive care units. It is single-center research with possible differences in other settings. The cohort included is relatively small.
Ethics Declarations
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of Hospital Metropolitan and performed in compliance with the Declaration of Helsinki. All patients signed informed consent forms before participation.
Competing Interests: The authors declare no competing interests.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
References
- Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J.,... & Tan, W. (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England journal of medicine, 382(8), 727-733.
- World Health Organization. (2022). WHO Director- General’s opening remarks at the media briefing on COVID-19. January, 30.
- Morawska, L., & Cao, J. (2020). Airborne transmission of SARS-CoV-2: The world should face the reality. Environment international, 139, 105730.
- Wu, F., Zhao, S., Yu, B., Chen, Y. M., Wang, W., Song, Z.G., ... & Zhang, Y. Z. (2020). A new coronavirus associated with human respiratory disease in China. Nature, 579(7798), 265-269.
- Gupta, A., Madhavan, M. V., Sehgal, K., Nair, N.,Mahajan, S., Sehrawat, T. S., ... & Landry, D. W. (2020). Extrapulmonary manifestations of COVID-19. Nature medicine, 26(7), 1017-1032.
- Zaim, S., Chong, J. H., Sankaranarayanan, V., & Harky,A. (2020). COVID-19 and multiorgan response. Current problems in cardiology, 45(8), 100618.
- Du, P., Li, D., Wang, A., Shen, S., Ma, Z., & Li, X. (2021).A Systematic Review and Metaâ?ÂÂAnalysis of Risk Factors Associated with Severity and Death in COVID-19 Patients. Canadian Journal of Infectious Diseases and Medical Microbiology, 2021(1), 6660930.
- Wang, Y., Tian, H., Zhang, L., Zhang, M., Guo, D., Wu, W., ... & MacIntyre, C. R. (2020). Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ global health, 5(5), e002794.
- Hashan, M. R., Smoll, N., King, C., Ockenden-Muldoon, H., Walker, J., Wattiaux, A., ... & Khandaker, G. (2021). Epidemiology and clinical features of COVID-19 outbreaks in aged care facilities: A systematic review and meta- analysis. EClinicalMedicine, 33.
- McMichael, T. M., Currie, D. W., Clark, S., Pogosjans, S., Kay, M., Schwartz, N. G., ... & Duchin, J. S. (2020). Epidemiology of COVID-19 in a long-term care facility in King County, Washington. New England Journal of Medicine, 382(21), 2005-2011.
- Onder, G., Rezza, G., & Brusaferro, S. (2020). Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. Jama, 323(18), 1775-1776.
- Richardson, S., Hirsch, J. S., Narasimhan, M., Crawford,J. M., McGinn, T., Davidson, K. W., ... & Northwell COVID-19 Research Consortium. (2020). Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. jama, 323(20), 2052-2059.
- Hageman, J. R. (2020). The coronavirus disease 2019 (COVID-19). Pediatric annals, 49(3), e99-e100.
- Jung, S. M., Akhmetzhanov, A. R., Hayashi, K., Linton,N. M., Yang, Y., Yuan, B., ... & Nishiura, H. (2020). Real- time estimation of the risk of death from novel coronavirus (COVID-19) infection: inference using exported cases. Journal of clinical medicine, 9(2), 523.
- Ali, M. J., Hanif, M., Haider, M. A., Ahmed, M. U., Sundas,F. N. U., Hirani, A., ... & Karim, A. H. (2020). Treatment options for COVID-19: a review. Frontiers in medicine, 7, 480.
- Rojas-Marte, G., Khalid, M., Mukhtar, O., Hashmi, A. T., Waheed, M. A., Ehrlich, S., ... & Shani, J. (2020). Outcomes in patients with severe COVID-19 disease treated with tocilizumab: a case–controlled study. QJM: An International Journal of Medicine, 113(8), 546-550.
- Basch, C. H., Meleo-Erwin, Z., Fera, J., Jaime, C., & Basch,C. E. (2021). A global pandemic in the time of viral memes:COVID-19 vaccine misinformation and disinformation on TikTok. Human vaccines & immunotherapeutics, 17(8), 2373-2377.
- Jentsch, P., Anand, M., & Bauch, C. T. (2020). Prioritising COVID-19 vaccination in changing social and epidemiological landscapes. medRxiv, 2020-09.
- Shoukat, A., Vilches, T. N., Moghadas, S. M., Sah, P.,Schneider, E. C., Shaff, J., ... & Galvani, A. P. (2022). Lives saved and hospitalizations averted by COVID-19 vaccination in New York City: a modeling study. The Lancet Regional Health–Americas, 5.
- Eyre, D. W., Taylor, D., Purver, M., Chapman, D., Fowler, T., Pouwels, K. B., ... & Peto, T. E. (2022). Effect of Covid-19 vaccination on transmission of alpha and delta variants. New England Journal of Medicine, 386(8), 744-756.
- Watson, O. J., Barnsley, G., Toor, J., Hogan, A. B., Winskill, P., & Ghani, A. C. (2022). Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. The Lancet infectious diseases, 22(9), 1293-1302.
- Meslé, M. M., Brown, J., Mook, P., Hagan, J., Pastore,R., Bundle, N., ... & Pebody, R. G. (2021). Estimated number of deaths directly averted in people 60 years and older as a result of COVID-19 vaccination in the WHO European Region, December 2020 to November 2021. Eurosurveillance, 26(47), 2101021.
- Emily, L., Gilad, G., Haim, M. E., & Galina, G. (2022). Functional dependency and COVID-19 in elderly patients with mild to moderate disease. Experience of tertiary geriatric hospital. Experimental Gerontology, 157, 111620.
- Beauchamp, M. K., Joshi, D., McMillan, J., Oz, U. E., Griffith, L. E., Basta, N. E., ... & Cosco, T. (2022). Assessment of functional mobility after COVID-19 in adults aged 50 years or older in the Canadian longitudinal study on aging. JAMA Network Open, 5(1), e2146168-e2146168.
- Plotnikov, G., Waizman, E., Tzur, I., Yusupov, A., Shapira, Y., & Gorelik, O. (2021). The prognostic role of functional dependency in older inpatients with COVID-19. BMC geriatrics, 21, 1-7.
- Soiza, R. L., Scicluna, C., & Thomson, E. C. (2021). Efficacy and safety of COVID-19 vaccines in older people. Age and ageing, 50(2), 279-283.
- Sadarangani, M., Raya, B. A., Conway, J. M., Iyaniwura,S. A., Falcao, R. C., Colijn, C., ... & Gantt, S. (2021). Importance of COVID-19 vaccine efficacy in older age groups. Vaccine, 39(15), 2020-2023.
- G. de Mexico, “Gobierno de mexico. política nacional de vacunación contra el virus sars-cov-2 para la prevención de la covid19 em méxico.,” Gobierno de Mexico, 2020.
- Fan, G., Tu, C., Zhou, F., Liu, Z., Wang, Y., Song, B., ...& Cao, B. (2020). Comparison of severity scores for COVID-19 patients with pneumonia: a retrospective study. European Respiratory Journal, 56(3).
- Li, X., Zhong, X., Wang, Y., Zeng, X., Luo, T., & Liu, Q. (2021). Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PloS one, 16(5), e0250602.
- Geng, J., Yu, X., Bao, H., Feng, Z., Yuan, X., Zhang, J.,... & Yu, H. (2021). Chronic diseases as a predictor for severity and mortality of COVID-19: a systematic review with cumulative meta-analysis. Frontiers in Medicine, 8, 588013.
- Haimovich, A. D., Ravindra, N. G., Stoytchev, S., Young,H. P., Wilson, F. P., Van Dijk, D., ... & Taylor, R. A. (2020). Development and validation of the quick COVID-19 severity index: a prognostic tool for early clinical decompensation. Annals of emergency medicine, 76(4), 442-453.
- Katz, S., Ford, A. B., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963). Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function. jama, 185(12), 914-919.
- Self-maintenance, P. (1969). Assessment of older people: self-maintaining and instrumental activities of daily living.
- SShinar, D., Gross, C. R., Bronstein, K. S., Licata-Gehr, E. E., Eden, D. T., Cabrera, A. R., ... & Kunitz, S. C. (1987). Reliability of the activities of daily living scale and its use in telephone interview. Archives of physical medicine and rehabilitation, 68(10), 723-728.
- Dauphinot, V., Boublay, N., Moutet, C., Achi, S., Bathsavanis, A., & Krolak-Salmon, P. (2020). Comparison of Instrumental Activities of Daily Living assessment by face-to-face or telephone interviews: a randomized, crossover study. Alzheimer's Research & Therapy, 12, 1-10.
- Emily, L., Gilad, G., Haim, M. E., & Galina, G. (2022). Functional dependency and COVID-19 in elderly patients with mild to moderate disease. Experience of tertiary geriatric hospital. Experimental Gerontology, 157, 111620.
- Wang, G., Yao, Y., Wang, Y., Gong, J., Meng, Q., Wang, H., ... & Zhao, Y. (2023). Determinants of COVID-19 vaccination status and hesitancy among older adults in China. Nature medicine, 29(3), 623-631.
- Gaitán-Rossi, P., Mendez-Rosenzweig, M., García-Alberto, E., & Vilar-Compte, M. (2022). Barriers to COVID-19 vaccination among older adults in Mexico City. International Journal for Equity in Health, 21(1), 85.