
World Journal of Clinical & Medical Images(WJCMI)
ISSN: 2833-9312 | DOI: 10.33140/WJCMI


Mini Review Article - (2026) Volume 4, Issue 1
Concomitant Anterior and Posterior Urethral Valves in an 11-Year-Old Boy
Received Date: Feb 02, 2026 / Accepted Date: Feb 27, 2026 / Published Date: Mar 11, 2026
Copyright: ©2026 Diptiranjan Bai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Bai, D. (2026). Concomitant Anterior and Posterior Urethral Valves in an 11-Year-Old Boy. World J Clin Med Img, 4(1), 01-03.
Abstract
Concomitant anterior and posterior urethral valves are extremely rare causes of bladder outlet obstruction in children. An 11-year-old boy presented with acute dysuria and long-standing weak urinary stream. Imaging revealed a dilated posterior urethra with distal narrowing, and cystoscopy confirmed both posterior and anterior urethral valves. Holmium: YAG laser fulguration of both lesions resulted in marked improvement and a normal postoperative MCU. This case emphasizes the need for thorough radiologic and endoscopic evaluation in children with persistent voiding symptoms to identify rare dual obstructive anomalies.
Introduction
Prevalence ratio of posterior urethral valve (PUV) is 2.10 per 10,000 births.1 Anterior urethral valve (AUV) is the most common congenital obstructive lesion of the anterior urethra but are 25 to 30 times less common than PUVs.2 But concomitant occurrence of anterior and posterior urethral valves is rare. Very few such cases have been reported in literature. Here we are reporting one such case treated by us.Case Description
An 11-year-old boy presented with severe dysuria and difficulty voiding for 4 days, with a long-standing history of weak urinary stream for 3 years. He had no prior urethral instrumentation, urinary tract infections, or perinatal complications. Antenatal ultrasound was normal. Urine examination was unremarkable and serum creatinine was 1 mg/dL. Ultrasonography showed mild bladder wall thickening without hydroureteronephrosis and bilaterally normal kidneys. Uroflowmetry demonstrated a voided volume of 240 mL and Qmax of 4 mL/s. Micturating cystourethrogram (MCU) revealed a dilated posterior urethra consistent with posterior urethral valve (PUV), along with abrupt tapering of the anterior urethra, suggesting an anterior urethral valve (AUV).
Cystourethroscopy confirmed obstructing PUV distal to the verumontanum. The valves were fulgurated using Holmium: YAG laser at the 5, 7, and 12 o’clock positions. A cusp-like anterior urethral valve at 6 o’clock in the penile urethra was identified, and both its proximal and distal lips were incised to lay it open. The child had immediate improvement in urinary stream. Follow-up MCU demonstrated a normal urethral contour without obstruction.
Discussion
Concomitant occurrence of AUV and PUV is extremely rare, with only a small number of cases reported. AUVs are 25–30 times less common than PUVs, and their embryologic coexistence is unexplained because both lesions arise from distinct developmental mechanisms3, 4. One hypothesis suggests that severe proximal obstruction from PUV may prevent adequate expansion of an anterior urethral diverticulum, thereby reducing the likelihood of AUV formation, explaining the rarity of dual lesions5.
AUVs most commonly occur in the bulbar urethra (40%), followed by the penoscrotal junction and pendulous urethra. Clinical presentation of combined PUV and AUV is variable, ranging from neonatal bladder outlet obstruction to late-childhood symptoms such as poor stream, straining, incontinence, or recurrent infections. MCU remains the most useful initial investigation because it can demonstrate both posterior dilation and anterior urethral caliber change. Endoscopic valve ablation is the treatment of choice and usually results in symptom resolution.

Figure 1: Pre-Operative MCU of Patient Showing Post Urethral Valve
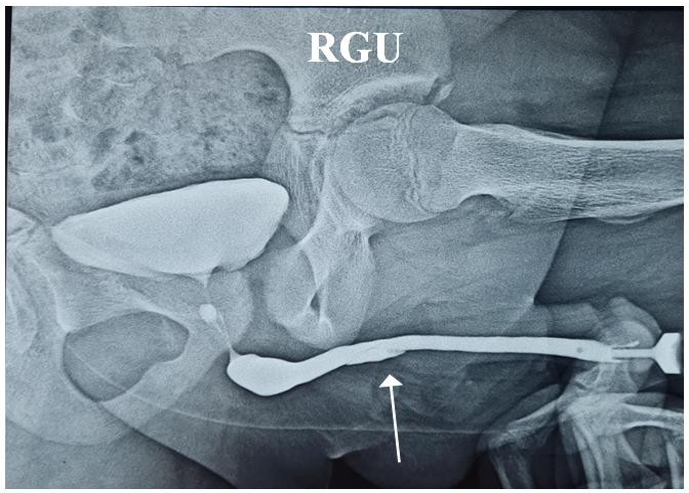
Figure 2: Pre-Operative RGU of Patient Showing Anterior Urethral Valve
Conclusion
Concomitant PUV and AUV can occur rarely. MCU is the most useful investigation helping in its diagnosis. Patients may present later in childhood with this disease. Endoscopic fulguration of the valves is currently most favoured treatment of this condition.
Declaration of Patient Consent:
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship: Nil.
References
- Malin, G., Tonks, A. M., Morris, R. K., Gardosi, J., & Kilby,M. D. (2012). Congenital lower urinary tract obstruction: a populationâ?based epidemiological study. BJOG: An International Journal of Obstetrics & Gynaecology, 119(12), 1455-1464..
- Tran, C. N., Reichard, C. A., McMahon, D., & Rhee, A. (2014). Anterior urethral valve associated with posterior urethral valves: report of 2 cases and review of the literature. Urology, 84(2), 469-471.
- Rao, K. L. N., Eradi, B., & Menon, P. (2003). Anterior and posterior urethral valves: a rare association. Journal of Pediatric Surgery, 38(7), E23-E24.
- Lassaad, S., Rachida, L., Manel, B. S., Randa, S., Mongi, M., Kais, M., ... & Abdellatif, N. (2011). Anterior and posterior urethral valves: a rare association. Open Journal of Pediatrics, 1(3), 34-36.
- Kajbafzadeh, A. M., Jangouk, P., & Yazdi, C. A. (2005). Anterior urethral valve associated with posterior urethral valves. Journal of pediatric urology, 1(6), 433-435.