
Journal of Novel Physiotherapies Research Reviews(JNP)
ISSN: 2771-7739 | DOI: 10.33140/JNP

Research Article - (2022) Volume 3, Issue 2
Comparison Of Quality-Of-Life Questionnaires, In Patients with Osas
2Director from N√ļcleo de Otorrinolaringologia e Medicina do Sono de S√£o Paulo, Adress: Alameda dos Nhambiquaras 159, Moema, S√£o Paulo, SP, Brazil
3M.D from N√ļcleo de Otorrinolaringologia e Medicina do Sono de S√£o Paulo, Adress: Alameda dos Nhambiquaras 159, Moema, S√£o Paulo, SP, Brazil
4M.D from N√ļcleo de Otorrinolaringologia e Medicina do Sono de S√£o Paulo, Adress: Alameda dos Nhambiquaras 159, Moema, S√£o Paulo, SP, Brazil
Received Date: Jun 01, 2022 / Accepted Date: Jun 14, 2022 / Published Date: Aug 05, 2022
Copyright: ©√ā¬©2022 Gabriel Santos de Freitas, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Gabriel Santos de Freitas, José Antonio Pinto, Davi Knoll Ribeiro, Heloisa dos Santos Sobreira Nunes .(2022). Comparison Of Quality-Of-Life Questionnaires, In Patients with Osas. J Nov Psy, 3(2), 76-81.
Abstract
Obstructive sleep apnea syndrome (OSAS) is a chronic and progressive disease with high morbidity and mortality, affecting 4% of men and 2% of women [1]. It includes a wide variety of symptoms, the most important being snoring (90% of the case), excessive daytime sleepiness, altered mood, morning headache, impotency, decrease of intellectual yield and cardiology, neurological and metabolic changes [2].
Keywords
Fosq; Epworth; AHI; questionnaires; quality of life; Osas.
Introduction
Obstructive sleep apnea syndrome (OSAS) is a chronic and progressive disease with high morbidity and mortality, affecting 4% of men and 2% of women [1]. It includes a wide variety of symptoms, the most important being snoring (90% of the case), excessive daytime sleepiness, altered mood, morning headache, impotency, decrease of intellectual yield and cardiology, neurological and metabolic changes [2].
Excessive daytime sleepiness is the main and most common symptom. Apneas are characterized by a complete stop and hypopneas by a reduction of the passage of air through the upper airway with a minimum duration of 10 seconds, occurring several times and exclusively during sleep [3].
In case of obstructive sleep apnea syndrome (OSAS), obtaining a complete and accurate history is often problematic, due to the occurrence of nocturnal OSA signs, being often, only understood by one’s spouse [4].
Combined to these difficulties, various subjective evaluation methods have been developed in an attempt to elucidate the diagnosis of OSAS, aided by the evaluation of home monitoring and sleep laboratory polysomnography.
Self-assessment questionnaires, can provide subjective data about the intensity of daytime sleepiness. Among the existing questionnaires the most used one is the Epworth Sleepiness scale (ESS), which measures the propensity to fall asleep, as well as the severity of excessive sleepiness, and the evaluation of the response in OSA treatment. In 1997, the Functional Outcome Sleep Questionnaire (FOSQ), was developed to evaluate the functional impact of sleepiness in daily life activities [5, 6].
In this study, we will use the Epworth sleepiness scale, and the Functional Outcome Sleep Questionnaire in its shortest version, known as FOSQ 10 developed in 2009 by Weaver, who in addition to drowsiness included the relationship of sleep to the quality of life [7].
Although OSAS take into account abnormalities in PSG and symptoms, its severity is usually defined separately by the AHI. However, we are aware of the fact that the AHI on its own does not evaluate the severity of the disease but it does in combination with the data provided by the sleep study [8].
There is a need for validation of the FOSQ in Brazil, which is already established in other countries. We believe that any cultural differences will not interfere in our context.
Objectives
To evaluate the effectiveness of two quality of life questionnaires in patients complaining about excessive daytime sleepiness and snoring, using the Functional Outcome Sleep Questionnaire (FOSQ-10), and Epworth sleepiness Scale of (ESS), as well as one’s application and its direct correlation with the AHI.
Materials and Methods
Our study received approval from the Research Ethics Committee, registered under number 059170/2016. We delineated an observational prospective study.
The following variables were analyzed: age, anthropometric characteristics (weight, height, body mass index [BMI]), duration of complaints, type of complaints related to sleep (snoring, insomnia, excessive daytime sleepiness), sleep apnea and hypopnea index (AHI). Inclusion criteria were patients between 18 and 80 years, without prior surgery, with complaints related to sleep disorders. Exclusion criteria were: children under 18 years, previous surgeries, previous use of CPAP.
All participants who sought our institution with sleep-related complaints filled out the FOSQ and ESE questionnaires that are described in table 1, they underwent polysomnography, were evaluated by two different examiners, weighted on a digital scale, height was measured and BMI calculated.
The reference values of ESS and FOSQ 10, are described in table 2.
Table 1: Questionnaires of Quality of Life
|
Epworth sleepiness scale |
Functional sleep questionnaire* |
|
Situation chance of dozing |
Fosq 10 |
|
1. Sitting and reading............................................................ |
Q1. You have difficulty to concentrating for being sleepy or tired? |
|
2. Watching TV ...................................................................... |
Q2. Do you have difficulty in remembering things about being sleepy or tired? |
|
3. Sitting, inactive in a public place (e.g., a theatre or a meeting.) ............................................................................... |
Q3. Do you have difficulty in driving a car for short distances (less than 300 km) by getting sleepy? |
|
4. As a passenger in a car for an hour without a break......... |
Q4. Do you have difficulty in driving a car for long distances (more than 300 km) by getting sleepy? |
|
5. Lying down to rest in the afternoon when circumstances permit. .................................................................................... |
Q5. Have you been having trouble leaving home to visit family or friends to be sleepy or tired? |
|
6. Sitting and talking to someone .......................................... |
Q6. Have you been having relationship problems with family, friends or co-workers to be sleepy or tired? |
|
7. Sitting quietly after a lunch without alcohol...................... |
Q7. You have a hard time watching TV by sleepy or tired? |
|
8. In a car, while stopped for a few minutes in the traffic .... |
Q8. You have difficulty making activities at night by sleepy or tired? |
|
|
Q9. You have trouble starting in the morning activities to be sleepy or tired? |
|
|
Q10. Have you been having mood swings to be sleepy or tired? |
|
Chance of Dozing (0-3) |
*For all the questions respond: |
|
0 = would never doze |
(1). yes, many |
|
1 = slight chance of dozing |
(2). yes, medium. |
|
2 = moderate chance of dozing |
(3) yes, little. |
|
3 = high chance of dozing |
(4). no |
Table 2: Reference Values of Ess and Fosq 10
|
Fosq |
Normal value |
Standart deviation |
Ess |
Meaning |
|
General Productivity |
3.64 |
0.51 |
<10 |
normal |
|
Vigilance |
3.51 |
0.67 |
10 -16 |
sleepiness |
|
Social Outcomes |
3.80 |
0.46 |
>16 |
excessive daytime sleepiness |
|
Activity Level |
3.61 |
0.54 |
- |
- |
|
Intimacy and sexual Relationships |
3.93 |
0.17 |
- |
- |
|
Total |
17.87 |
3.08 |
- |
- |
Linear correlation analyses were conducted using the Spearman rank correlation coefficient (rho). The considered Kappa coefficient with its 95% CI was used as a standard to evaluate the correlation between ordinal scale variables. Categorical variables were described with counts and proportions. Quantitative variables of normal distribution and asymmetry were described as mean ± standard deviation or median (interquartile range) respectively. The software R (R Foundation, Vienna, Austria) was used in the statistical analysis of data. All the probabilities of the significance presented are of the bilateral type and values that are less than 0.05 are considered statistically significant [9].
Results
Comparison of the effectiveness of two quality of life questionnaires, ESS and FOSQ-10, using data from patients (n = 100), with complaints of snoring, insomnia and excessive daytime sleepiness, who were attended in the years 2015 to 2017 in a private institution. The average age of the patients was 47.69, BMI medium was 28.91 kg/m ², the most common complaint was snoring in 86% of patients. The average AHI was 24.95 ranging from 3.7 to 106.6 in 100 patients, with 32 light apneas, 38 moderate and 30 severe, (AHI-5 -15 = light; moderate; 15-30 > 30 severe). (Table 3).
Table 3: Reference Values
|
Variables |
Patients |
Mean |
Standart deviation |
|
AGE |
100 |
47.69 |
14.63 |
|
BMI |
100 |
28.91 |
4.413 |
|
FOSQ |
100 |
15.18 |
3.147 |
|
EPW |
100 |
9.7 |
5.1 |
|
AHI |
100 |
24.95 |
19.30 |
Figures 1 and 2 present the comparative graphs at a significance level of 5%, showing that no significant correlation was observed between FOSQ and PSG (AHI) with (p = 0.91), furthermore no significant correlation was observed between ESE and PSG (AHI) (p = 0.27). (Table 4).


Figure 1: FOSQ X AIH Figure 2: ESS X AIH
Table 4
|
Variables |
N |
Spearman rank correlation |
Spearman 95% ci lower |
Spearman 95% ci upper |
P-VALUE |
|
|
ESS |
PSG (IAH) |
100 |
0.112 |
-0.087 |
0.302 |
0.27 |
|
FOSQ |
PSG (IAH) |
100 |
-0.011 |
-0.207 |
0.185 |
0.91 |
|
Fosq = functional outcome sleep questionaire; ess = epworth sleep scale; n = number of patients = 100; ahi = apneia-hipopneia index |
||||||
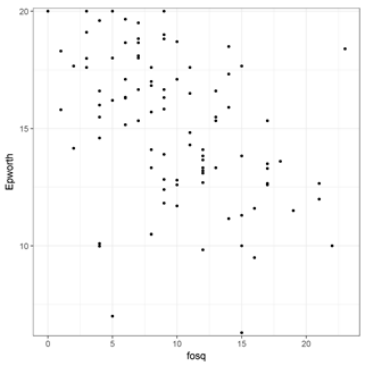
Figure 3
Figure 3 evaluates the significance level at 5%, where we observed moderate and significant inverse correlation between FOSQ and ESS (p < 0.001), which evidences that the higher the ESS value, the lower the FOSQ value will be. (Table 5).
Table 5
|
VARIABLES |
N |
SPEARMAN RANK CORRELATION |
SPEARMAN 95% CI LOWER |
SPEARMAN 95% CI UPPER |
P-VALUE |
|
|
FOSQ |
ESS |
100 |
-0.497 |
-0.632 |
-0.333 |
<0.0001 |
|
N = number of patients = 100 |
||||||
Discussion
This paper reflects our interest in these questionnaires, this is due to the increasing development of instruments designed for the evaluation of specific diseases. The Epworth was developed as a subjective measuring instrument of daytime sleepiness and has been translated and validated for use in several other languages, including Brazilian Portuguese, its use is simple, easy to understand and quick to fill in [10].
The FOSQ is a self-evaluating questionnaire, with the following fields: social status, intimacy and sex, activity level, surveillance, and overall productivity. In this way, it gives additional information about the general health of the patient and therefore complements the evaluation provided by the Epworth sleepiness scale.
FOSQ validation was realized in innumerable countries, [11 -17] in some cases like in the one of Korea, the original questionnaire was adapted and reduced to 24 questions showing that this validation is faced with cultural differences, so the cultural variability can seriously affect the design of the questionnaire and the expected results [18].
We know that the prevalence of light OSA can vary from 3 to 28% of the adult population, while moderate to severe OSA (AHI ≥ 15) can range from 1 to 14% [19].
It is important to note that OSAS used to be underdiagnosed, especially in cases where there is no complaint of excessive daytime sleepiness. Due to this difficulty, simple and effective tracking methods are therefore essential to the ENT, in situations where the full sleep evaluation, including polysomnography is not practical or feasible, so more and more subjective evaluation methods prevail to attempt to elucidate the diagnosis of OSAS.
The use of quality-of-life questionnaires has been employed not only in otolaryngology, also in rheumatology. Sleep disorders are common in a wide variety of rheumatologic diseases sleep changes can have direct correlation with pain, depression, lack of exercise, or the use of corticosteroids. FOSQ’s results has been used in research and clinical practice to measure the impact of daytime sleepiness in activities on daily living [20]. We use its simplified version known as FOSQ 10, being a psychometric instrument that works similarly to the long version (FOSQ-30), which is easy and quickly to use, and it has a good configuration in clinical application [7].
The ESS is designed to measure the propensity of sleep in a simple and standardized way. It covers the whole range of propensities of sleep, from the highest to the lowest and is based on eight questions where the subjects are asked to rank on a 0-3 scale the chance of dozing off or falling asleep in eight situations, based on their way of life in recent times. The total score is obtained by adding up the values for all the options. The minimum score is 0 (no sleepiness) and the maximum 24 (disabling drowsiness) [5].
ESS has been used in medical practice since its inception in 1991, in the questionnaire a distinction is made between dozing off or simply feeling tired. Scores above 16 points indicate a high rate of daytime sleepiness, and according to the studies, these levels are only found in patients with narcolepsy, idiopathic hypersomnia and OSAS (AHI > 15), less than 8 points, refer to normal daytime vigilance [5].
FOSQ 10 is a consistent instrument that performs similarly to the previous version (FOSQ-30), the measure of the impact of daytime sleepiness in activities of daily living, is based on 10 issues, representing each of the 5 subscales (overall productivity, level of activity, level of vigilance, social coexistence and evaluations of intimacy and sex).
In case of subjective evaluation questionnaires, we must agree that there may be flaws in the measures of quality of life, even to discriminate primary snorers from OSA patients, as proven by Liu et al. in 69 patients [21].
This present study showed a correlation between an acceptable score on the scale of Epworth and the score of FOSQ. Thus, FOSQ can provide additional information on how excessive sleepiness evaluated by the Epworth scale affects the quality of life of patients.
The PSG indexes correlate poorly with other measures for the evaluation of OSA, including subjective evaluation of the degree of sleepiness, quality of life questionnaires related to OSAS and the assessment of the general state of health [22].
Therefore, this study suggests that the PSG measures failed to evaluate all elements of OSAS, so it should not be used exclusively to evaluate the response to treatment [23]. We have noticed that patients seldom show direct care to improve the AHI or another parameter of PSG, but rather improve the symptoms of the disease in question as well as their quality of life. Despite the AHI being the measure used to assess the severity of the patient with OSA, we should not associate the index with subjective assessment and instead correlate the Polysomnographic data and subjective evaluation questionnaires with the clinical condition of the patient.
However, PSG indices are not consistently associated with sleepiness, quality of life, this both at the baseline and as measures of outcome in patients with OSAs. The indexes cannot quantify some important aspects of OSAS nor the outcome of treatment. The clinical results have their due importance and should be measured directly [24].
This is an initial study comparing two subjective ways related to the evaluation of the quality of life in patients with OSAS, it´s the first step towards validation of FOSQ in Brazil.
Conclusion
This study has shown an acceptable correlation between the scores on the Epworth and FOSQ scale. Hence, FOSQ can provide additional information about how excessive sleepiness evaluated by the Epworth scale affects the quality of life of patients. There is no relationship between the severity of the AHI Polysomnographic characteristics with the quality-of-life questionnaires, evidencing that the AHI is not an isolated dominant factor during the evaluation of patients with obstructive sleep apnea syndrome.
Conflict of Interest
Author José Antonio Pinto declares that he has no conflict of interest, Author Gabriel Santos de Freitas declares that he has no conflict of interest, Author Antonio Abel Pauperio declares that he has no conflict of interest, Author Davi Knoll Ribeiro declares that he has no conflict of interest, Author Heloisa dos Santos Sobreira Nunes declares that he has no conflict of interest, Author Beatriz Silveira Zalla declares that he has no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards, The Research and Ethics Committee of the São Camilo University center reviewed and approved the research protocol 059170/2016.
References
- Young, T., Palta, M., Dempsey, J., Skatrud, J., Weber, S., & Badr, S. (1993). The occurrence of sleep-disordered breathing among middle-aged adults. New England Journal of Medicine, 328(17), 1230-1235.
- Pinto, J. A. (2000). Síndrome da apnéia obstrutiva do sono: uma tarefa multidisciplinar. Pinto JA. Ronco e apnéia do sono. Revinter, 1, 1-2.
- Aloe, F. (1999). Distúrbio respiratório sono dependente. Ronco e Apnéia do sono, 21-32.
- Friedman, M., Wilson, M. N., Pulver, T., Pandya, H., Joseph,N. J., Lin, H. C., & Chang, H. W. (2010). Screening for obstructive sleep apnea/hypopnea syndrome: subjective and objective factors. Otolaryngology--Head and Neck Surgery, 142(4), 531-535.
- Johns, M. W. (1991). A new method for measuring daytime sleepiness: the Epworth sleepiness scale. sleep, 14(6), 540-545.
- Weaver, T. E., Laizner, A. M., Evans, L. K., Maislin, G., Chugh,D. K., Lyon, K., ... & Dinges, D. E. (1997). An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep, 20(10), 835-843.
- Chasens, E. R., Ratcliffe, S. J., & Weaver, T. E. (2009). Development of the FOSQ-10: a short version of the Functional Outcomes of Sleep Questionnaire. Sleep, 32(7), 915-919.
- Quan, S. F., Gillin, J. C., Littner, M. R., & Shepard, J.W. (1999). Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. editorials. Sleep (New York, NY), 22(5), 662-689.
- Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. biometrics, 159-174.
- Bertolazi, A. N., Fagondes, S. C., Hoff, L. S., Pedro, V. D., Menna Barreto, S. S., & Johns, M. W. (2009). Validação da escala de sonolência de Epworth em português para uso no Brasil. Jornal Brasileiro de Pneumologia, 35, 877-883.
- Vidal, S., Ferrer, M., Masuet, C., Somoza, M., Ballarín,J. I. M., & Monasterio, C. (2007). Spanish version of the Functional Outcomes of Sleep Questionnaire: scores of healthy individuals and of patients with sleep apnea-hypopnea syndrome. Archivos de Bronconeumología ((English Edition)), 43(5), 256-261.
- Korpe, L., Lundgren, J., & Dahlström, L. (2013). Psychometric evaluation of a Swedish version of the Functional Outcomes of Sleep Questionnaire, FOSQ. Acta Odontologica Scandinavica, 71(5), 1077-1084.
- Rodríguez-Pérez, V., Valencia-Flores, M., Reyes-Lagunes, I., & del Carmen Lara-Muñoz, M. (2013). Adaptation and Psychometric Validation of the Functional Outcomes Sleep Questionnaire (FOSQ) in Mexico City Inhabitants. Salud mental, 36(4), 307-313.
- Stavem, K., Kjelsberg, F. N., & Ruud, E. A. (2004). Reliability and validity of the Norwegian version of the Functional Outcomes of Sleep Questionnaire. Quality of Life Research, 13(2), 541-549.
- Banhiran, W., Assanasen, P., Metheetrairut, C., Nopmaneejumruslers, C., Chotinaiwattarakul, W., & Kerdnoppakhun, J. (2012). Functional outcomes of sleep in Thai patients with obstructive sleep-disordered breathing. Sleep and breathing, 16(3), 663-675.
- Izci, B., Firat, H., Ardic, S., Kokturk, O., Gelir, E., & Altinors,M. (2004). Adaptation of functional outcomes of sleep questionnaire (FOSQ) to Turkish population. Tuberk Toraks, 52(3), 224-230.
- Han, N. E., Kim, D. Y., & Lee, S. A. (2014). Validity of Korean version of functional outcomes of sleep questionnaire in patients with simple snoring and obstructive sleep apnea. Sleep Medicine Research, 5(1), 5-14.
- Johnson, T. P., Cho, Y. I., Holbrook, A. L., O’Rourke, D., Warnecke, R. B., & Chavez, N. (2006). Cultural variability in the effects of question design features on respondent comprehension of health surveys. Annals of Epidemiology, 16(9), 661-668.
- Young, T., Peppard, P. E., & Gottlieb, D. J. (2002). Epidemiology of obstructive sleep apnea: a population health perspective. American journal of respiratory and critical care medicine, 165(9), 1217-1239.
- Omachi, T. A. (2011). Measures of sleep-in rheumatologic diseases: Epworth Sleepiness Scale (ESS), Functional Outcome of Sleep Questionnaire (FOSQ), Insomnia Severity Index (ISI), and Pittsburgh Sleep Quality Index (PSQI). Arthritis care & research, 63(S11).
- Liu, J., & Toh, S. T. (2013). Failure of Quality-of-Life Measures to Discriminate between Primary Snorers and Patients with Obstructive Sleep Apnea. Otolaryngology— Head and Neck Surgery, 149(2_suppl), P267-P268.
- Weaver, E. M., Kapur, V., & Yueh, B. (2004). Polysomnography vs self-reported measures in patients with sleep apnea. Archives of Otolaryngology–Head & Neck Surgery, 130(4), 453-458.
- Weaver, E. M., Woodson, B. T., & Steward, D. L. (2005). Polysomnography indexes are discordant with quality of life, symptoms, and reaction times in sleep apnea patients. Otolaryngology-Head and Neck Surgery, 132(2), 255-262.