



Research Article - (2022) Volume 7, Issue 2
Comparison of Minimally Invasive Mitral Valve Surgery vs Open Mitral Valve Replacement
24thyear student in Zia Uddin University, Pakistan
Received Date: May 29, 2022 / Accepted Date: May 31, 2022 / Published Date: Jun 03, 2022
Copyright: ©Sumera Nasim, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sumera Nasim, Saif Naveed, Muhammad Aadil Qasim (2022). Comparison of Minimally Invasive Mitral Valve Surgery vs Open Mitral Valve Replacement. Cardio Open, 7(2): 254-258.
Abstract
Objective: To establish the advantages of invasive mitral valve surgery over open heart mitral valve surgery in treating patients with mitral valve pathologies.
Material and Methods: A literature search was done on PubMed, google scholar, and Embase using search terms like open ‘invasive mitral valve surgery’, ‘mitral clip’, ‘sternotomy’, and ‘annuloplasty.” The time limit was set to 5 years ago and the language set to English. After searching, a quick screening of the title and abstract was done for relevance. The selected papers were then used in this review.
Results: The minimally invasive mitral valve surgery was shown to have significantly greater survival rates across all post-surgical time frames as well as lower short-term mortality rates. Mini MVS was also shown to be more effective in treating infective endocarditis and is a highly impractical operation for patients with left ventricular dysfunction or other cardiomyopathies. The Minimally Invasive Mitral valve surgery (Mini MVS) proved to cause fewer mortalities and clearly showed a lower number of complications; the complications that exist are highly preventable. In addition, the mini MVS is more effective in treating patients with mitral regurgitation.
Conclusion: This review confirms that employing the minimally invasive MVS procedure for patients with mitral valve pathologies is more effective than the standard open heart MVS in terms of post-surgery mortalities and hospital stay times. It is also more effective in treating patients with preexisting cardiomyopathies. However, sufficient training should be done to prevent complications from arising. The mitraliclp device should be further developed to prevent complications that arise due to the clip attachment.
Keywords
Mitral Valve Surgery, Minimally Invasive Mitral Valve Surgery, Infective Endocarditis, Minimally Invasive Valve Repair
Introduction
Surgical repair, whether it be surgical replacement or repair, as a standard of care in Mitral valve (MV) pathologies due to degenerative changes depends on many factors influenced by both patient as well as surgeon and center [1]. These include the pre-operative status of the patient, any comorbidities, and severity of disease, expertise and experience of the respective surgeons as well as the centers providing this treatment. Such a procedure takes place when analysis based on three principles; creating large surface of leaflet cooptation, remodeling the an- nulus to Left Ventricle provide stable and optimal orifice area and restoring or preserving full mobility of leaflets, comprehen- sively done [2]. Being one of the most common heart valves related surgeries, it is imperative to shed light on the current lit- erature and look at what is known and what still needs lot needs to which is not known with as this a new technique its benefits will come and newer technique [3,4].
Previously conducted studies have reported on the short-term outcomes of the procedures that has observed that minimally invasive mitral valve surgery is favorable in terms of Intensive Care Unit (ICU) stay, need for blood transfusion and in hospi- tal stay. Such findings are suggestive of the fact that minimally invasive approaches have become the choice of treatment with such benefits are reported some of the risk factors such as in- creased risk of stroke, aortic dissection or injury, cardiopulmo- nary bypass etc [5-7]. The limitation however in such studies is the length of time it was conducted thus calling for a review of long-term studies in order to assess the full potential of the said risks as well as benefits [7,8].
This review provides a comprehensive view of the current litera- ture regarding the long-term survival rates of patient undergoing the surgery with any reported complications [7]. We shall also view the problems associated with the use the Mitra Clip and help in the identification of any possible solutions proposed for it. Lastly a common factor while performing any surgery that is, the different comorbidities and its role in the outcomes will help in providing the readers good understanding of the potential high-risk patients who require additional care.
Procedure Review
Tran’s catheter repair is a more invasive approach, occurs with the help of Mitral Clip, and used to treat symptomatic mitral regurgitation in those patients who cannot undergo open mitral valve surgery The Mitral Clip is made up of metal alloys and a polyester fabric [9]. In this procedure, cardiopulmonary bypass is not required. First patients are placed under general anesthe- sia due to the need of a Tran’s esophageal echo. The access is taken via the femoral vein. First, a transept puncture is made so that the catheter can pass through. After this, a steerable guide sheath is inserted into the left atrium. The Mitral Clip delivery system goes through this sheath and to the mitral valve. The clip is positioned where the mitral regurgitation is greatest, and the clip arms attach to the leaflets and closes, preventing the leaflets from going backward, thus prevents regurgitation. The delivery system is removed, and femoral site closed [10].
Annuloplasty is a low-risk surgical procedure to repair mitral valve. First, an incision is created on the left atrium to reveal the mitral valve. Certain structures need to be identified, namely the anterior and posterior commissures, and the right and left trigon. In addition, the central portion of the leaflets must be identified, and this is done by viewing the portion supported by the chordae. Then, the first suture should be placed at the poste- rior commissure and right trigon. Another suture is placed at the left trigone. To avoid rhythm disturbances, the sutures should be placed at the atrio-valvular junction, 1 millimeter from the leaflet hinge with the needle towards the ventricular cavity. The third suture on the posterior annulus is placed the same way with the 2 stitches at a space of 2 millimeters from the leaflet hinge, penetrating the atriovalvular junction. The remaining sutures are to be placed with the same method at the posterior annulus. Us- ing the inter-commissural distance and sept-lateral dimension to assess the size of the annulus, a prosthetic ring is selected. The annular sutures are passed within the ring, the ring is parachuted into place and sutures are sealed. To check if the repair was suc- cessful, the ventricle is filled with cardioplegia, a process known as hydrodynamic valve testing [11].
Minimally invasive techniques are starting to be preferred over conventional surgery for many reasons as quoted by several re- search findings. With this procedure, the length of in hospital stay as well as intensive care unit stay was significantly reduced, and a more prominent finding was the reduced need for blood transfusion [5]. A study conducted showed that the in-hospital length of stay was significantly lower with those patients having undergone trans catheter procedure (11.56 days) as compared with those undergone open surgery (14.01 days) (p = <0.0001) [12]. Furthermore, a 2013-14 registry involving those patients with mitral regurgitation (564 patients) showed that the Mitra Clip device had a 91.8% Success rate [13].
Statistical Analysis
A comparison between the long-term survival rate in conven- tional mitral valve surgery and the new minimally invasive mi- tral valve surgery was done. Minimally invasive surgery showed to have better results in one, five, ten-year survival rates. The one, five, and ten-year survival rates were significantly higher in the minimally invasive cohort compared to the conventional approach (96%, 90%, and 84% vs. 89%, 85%, and 70%) [14]. Even when the short- term survival rate was compared, the min- imally invasive technique showed better results. The mortality rate 30 days after discharge was far less in patients who under- went mini MVS as compared to the conventional MVS. Some data also suggests lower risk of perioperative morbidity and mortality with mini MVS.
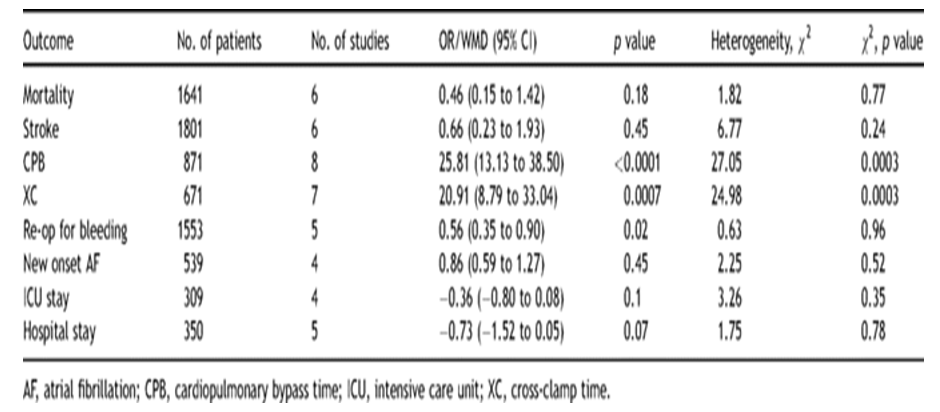
We also wanted to compare the two procedures when done on patients with the same co morbid such as rheumatic mitral valve disease, infective endocarditis, left ventricular dysfunction (along with the mitral valve repair itself). Anh Tuan Vo, et al re- ports a study where people with rheumatic disease were treated with mini MVS refer to Table 1, thirty-day mortality was signifi- cantly lower (0.7%). The overall survival rate was also higher 98.6%. Freedom from reoperation was 97.1% [15].
Table 1: Meta-Analysis of outcomes of Minimally Invasive Surgery
Cristina Barbero, et al report a mini MVS conducted on patients with infective endocarditis. Mini MVS showed and proved to be feasible for patients with I.E and was associated with better early and long-term results. Overall, actuarial survival rate at 1 and 5 years was 83%; freedom from MV reoperation and/ or recurrence of IE at 1 and 5 years was 97%. Thirty-day mortality was 11.4% [16]. The utilization of mini MVS approach has been rather controversial in presence of left ventricular (LV) dysfunc- tion. A study was done comparing patients with LV dysfunction underwent minimally invasive MVS. Patients with LV dysfunc- tion underwent mini MVS had low mortality (2.1% v 1.7%) and morbidity that was comparable with patients with normal ven- tricular function. Postoperative recovery was only slightly lon- ger compared with patients with normal LV function as noted by time to extubation (6.0 vs 7.0 hours) and hospital length of stay (7.0 vs 6.0 days) [17]. These shows that mini MVS is not only safe but also feasible for patients having a known cardiomyopa- thy with having minimal morbidity and mortality.
Team Dynamics and Leadership
A successful team should consist of high-performing individuals who each understand their roles and work as a cohesive unit. Achieving this goal within a MIVS program requires substan- tial collaborative effort for success. The team of dedicated pro- fessionals includes a lead cardiac surgeon, a surgical assistant, cardiologists, per fusionists, anesthesiologists, operating room (OR) technicians, and nurses [18].

Figure 1: Development of mini MVS Program
Complications
If we compare the clinical outcomes of the two procedures, that minimally invasive mitral valve repair is the ideal approach giv- en the reduced the number of mortalities (952 mortalities fur minimally invasive and 1011 for stem tom) a lower number of adverse clinical outcomes (wound injection, cerebrovascular in- cidents etc) in the case of minimally invasive repair, as compare to sternotomy is MIVR is more effective. Lesser the cross-clamp time, time for cardiopulmonary bypass, and duration of hospi- talization were all lower in the case of minimally invasive repair (although the ICU duration remained the same in 247 case of both procedures). This data further provide strength the fact that MIVR is a far safer procedure than the conventional sternotomy.
However, there are potential risks of irritation of the femoral nerve, seromas and lymphatic fistulas (while using the seldinger technique in which arterial air venous cannula are placed hi femo- ral vesse4) which can be prevented by properly clipping large ves- sels. In some cases, the femoral artery may be damaged after the cannula is removed. In addition, the risk of piercing the right atrial wall exists if canalization of the superior vena cava s carried out without Tran esophageal echo [19]. A times the surgeon is forced to convert to a full sternotomy if the pulmonary artery is damaged when placing the aortic cross lamp. Before the surgery proceeds further, the proper cannula positioning is ensured to minimize risk of the venous cannula being dislodged out of the superior vena cava outcomes of mini MVS vs CABG Table 2.
Table 2: Comparison of Mini invasive MVS VS MVR
|
OUTCOMES |
Mini MVS |
CABG |
|
Bleeding |
less |
high |
|
Transfusion of blood |
less |
high |
|
Atrial fibrillation |
less |
high |
|
Sternal wound infection |
less |
high |
|
Sternal scar |
less |
high |
|
Hospital Stay |
8 days |
15 |
|
Re valvular reintervention in Ist year |
less |
more |
|
Stroke |
high |
less |
|
Groin complication |
high |
less |
|
Aortic dissection |
high |
less |
|
Cross clamp and procedure time |
long |
short |
Life Threatning Complications
Phrenic nerve injury, vascular complications of the femoral ar- tery aortic dissections, unilateral pulmonary edema, and periop- erative strokes [10]. Partial clip detachment, embolization of clip, mitral valve stenosis, and clip entanglement in the chorda and mitral regurgitation are other potential complications of the mitral clip device [8]. Two studies have been carried out EVER- EST 1 & EVEREST 2 to determine the potential complications of the Mitraclip [20-22]. The goal of EVEREST 1 was to eval- uate the feasibility safety and efficacy of the Mitraclip system whereas the goal of EVEREST 2 was to evaluate the Mitraclip in those patients with elevated surgical risk due to previous car- diac surgery or multiple comorbidities. The results of EVEREST 1 concluded that the mitraclip system has reduced the rates of mortality and morbidity [22]. The results of EVEREST 2 con- cluded that the mitraclip system proved to be effective in patients suffering from mitral regurgitation and reduced other symptoms.
Abbreviations
MVS: Mitral Valve Surgery
MV: Mitral Valve
ICU: Intensive Care Unit
Mini MVS: Minimally Invasive Mitral Valve Surgery
IE: Infective Endocarditis
LV: Left Ventricle
MIVR: Invasive Valve Repair
Conclusion
Minimally invasive procedures are becoming increasingly com- mon in today’s age, considering the benefits especially in terms of postoperative care. Previously stated data showed that 30-day mortality rate, long-term survival and in hospital stay were all reduced in patients who underwent minimally invasive proce- dures. Furthermore, patients who were treated for rheumatic heart disease and infective endocarditis showed to have prom- ising results with the minimally invasive techniques. To prevent complications involving the femoral vessels, adequate training must be given to those who will be required to perform, inva- sive procedures in their practice. In addition, more research and explanation is needed for the mini MVS and training to avoid complication so more center should use this technique. Popu- lation will be benefited. Because refusal to open heart surgery was high in our population and cost effective than mitral valve replacement so it is the need of time and large randomized trials needed in Pakistani population where rheumatic heart disease of mitral valve is more prevalent.
References
- Salik, I., Lee, L., Widrich, J. (2020). Mitral Valve Repair. Stat Pearls Publishing.
- Carpenter Reconstructive Valve Surgery. First EditionValve-surgery/carpenters/December 11, 2010.
- Options for Heart Valve Replacement. (2020). American Heart Association. Beat-valve-problems and disease/under- standing.
- Van Praet, K. M., Stamm, C., Sündermann, S. H., Meyer, A., Unbehaun, A., & et al. (2018). Minimally invasive sur- gical mitral valve repair: state of the art review. Interven- tional Cardiology Review, 13(1), 14.
- Sündermann, S. H., Czerny, M., & Falk, V. (2015). Open vs. minimally invasive mitral valve surgery: surgical tech- nique, indications and results. Cardiovascular Engineering and Technology, 6(2), 160-166.
- Holzhey, D. M., Shi, W., Borger, M. A., Seeburger, J., Gar- bade, J., Pfannmüller, B., & Mohr, F. W. (2011). Minimal- ly invasive versus sternotomy approach for mitral valve surgery in patients greater than 70 years old: a propensi- ty-matched comparison. The Annals of thoracic surgery, 91(2), 401-405.
- Cheng, D. C., Martin, J., Lal, A., Diegeler, A., Folliguet, T. A., & et al. (2011). Minimally invasive versus conventional open mitral valve surgery a meta-analysis and systematic review. Innovations, 6(2), 84-103.
- https://wwwaccessdata.fda.gov/cirh_docs/pdf10/P100009c.pdf (accessed December11, 2020)
- Transcatheter Mitral Valve Repair. (2020). Mayo Clinic.
- Del Forno, B., Castiglioni, A., Sala, A., Geretto, A., Giaco- mini, A., & et al. (2017). Mitral valve annuloplasty. Multi- media Manual of Cardiothoracic Surgery: MMCTS, 2017.
- Ullah, W., Sattar, Y., Mukhtar, M., Abdullah, H. M., Figuere- do, V. M., & et al. (2020). Outcomes of open mitral valve re- placement versus Transcatheter mitral valve repair; insight from the National Inpatient Sample Database. IJC Heart & Vasculature, 28, 100540.
- Mitral Clip review - UCLA Interventional Cardiology. (2020). Los Angeles.
- Mkalaluh, S., Szczechowicz, M., Dib, B., Sabashnikov, A., Szabo, G., & et al. (2018). Early and long-term results of minimally invasive mitral valve surgery through a right mini-thoracotomy approach: a retrospective propensi- ty-score matched analysis. Peer J, 6, e4810.
- Vo, A. T., Le, K. M., Nguyen, T. T., Vu, T. T., Pham, C. V. T.,& et al. (2019). Minimally invasive mitral valve surgery for rheumatic valve disease. In Heart Surg Forum, 22(5):E390- E3E5.
- Barbero, C., Marchetto, G., Ricci, D., Mancuso, S., Boffini, M., & et al. (2017). Minimal access surgery for mitral valve endocarditis. Interactive CardioVascular and Thoracic Sur- gery, 25(2), 241-245.
- Atluri, P., Woo, Y. J., Goldstone, A. B., Fox, J., Acker, M. A., & et al. (2013). Minimally invasive mitral valve surgery can be performed with optimal outcomes in the presence of left ventricular dysfunction. The Annals of Thoracic Sur- gery, 96(5), 1596-1602.
- Wan, B., Rahnavardi, M., Tian, D. H., Bannon, P. G., & Yan,T. D. (2013). Meta-analysis protocol: MitraClip system ver- sus surgery for treatment of severe mitral regurgitation. An- nals of Cardiothoracic Surgery, 2(5), 679.
- Feldman, T., Kar, S., Elmariah, S., Smart, S. C., Trento, A., & et al. (2015). Randomized comparison of percutaneous repair and surgery for mitral regurgitation: 5-year results of EVEREST II. Journal of the American College of Cardiolo- gy, 66(25), 2844-2854.
- Czesla, M., Götte, J., Weimar, T., Ruttkay, T., & Doll, N. (2013). Safeguards and pitfalls in minimally invasive mitral valve surgery. Annals of Cardiothoracic Surgery, 2(6), 849- 852.
- Cuartas, M. M., & Davierwala, P. M. (2020). Minimally in-vasive mitral valve repair. Indian Journal of Thoracic and Cardiovascular Surgery, 36(1), 44-52.
- Bilge, M., Alsancak, Y., Ali, S., Duran, M., & Biçer, H.(2016). An extremely rare but possible complication of Mi- traClip: embolization of clip during follow-up. Anatolian Journal of Cardiology, 16(8), 636.
- Feldman, T., Kar, S., Rinaldi, M., Fail, P., Hermiller, J., & et al. (2009). Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVER- EST (Endovascular Valve Edge-to-Edge REpair Study) co- hort. Journal of the American College of Cardiology, 54(8), 686-694.