
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Review Article - (2021) Volume 6, Issue 2
Comparison between Laparoscopic, Abdominal, and Vaginal Hysterectomy in the Treatment of Gynecological Disease: A Retrospective Review Over Five Years
2Obstetrics and Gynecology Department, Al Zahraa Hospital University Medical Center, Beirut, Lebanon
3Head of Urology Department, Lebanese University, Beirut, Lebanon
4Urology Department Al Zahraa Hospital University Medical Center, Beirut, Lebanon
5Obstetrics & Gynecology Department, Lebanese University, Beirut, Lebanon
Received Date: Jun 10, 2021 / Accepted Date: Jun 16, 2021 / Published Date: Jun 21, 2021
Copyright: ©Kariman Ghazal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Jihad Al Hasan, Mauhammad Mousa, Zaynab Haroun, Kariman Ghazal. (2021). Comparison between Laparoscopic, Abdominal, and Vaginal Hysterectomy in the Treatment of Gynecological Disease: A Retrospective Review Over Five Years. Int J Women's Health Care, 6(2), 182-189.
Abstract
Background: Hysterectomy is one of the most common gynecological surgery worldwide. It is usually performed through the abdominal, vaginal or laparoscopic routes. The objective of this study was to evaluate the role of laparoscopic, vaginal and abdominal hysterectomy in the management of gynecological conditions in terms of operative outcomes, such as operating time and estimated blood loss, as well as complication rates.
Methods: This was a retrospective cohort study carried out over a 5-year period (2016-2020) at Zahraa University Hospital. Patients who underwent abdominal vaginal, and laparoscopic hysterectomies performed for the treatment of multiple gynecological disease during that period were included.
Results: A total of 222 patients were included in the study, 168 (75.7%) patients in the abdominal hysterectomy group, 7 (3.2%) in the vaginal group, and 47 (21.1%) in the laparoscopic group. The mean age was 49.83±9.28 years for the abdominal, 67.14±13.79 for the vaginal, and 47.26±6.77 years for the hysterectomy groups. The most common indication for hysterectomy was the presence of uterine fibroids in the abdominal and laparoscopic groups (47.6% vs. 31.9% respectively) whereas it was pelvic organ prolapse for all patients in the vaginal group. Around 18% in the abdominal group had abnormal uterine bleeding compared to 6.4% in the laparoscopic group. Endometrial hyperplasia was the indication for 9.5% of the patients in the abdominal group while it was 25.5% for the laparoscopic group. Surgery duration was significantly the shortest for abdominal hysterectomy (2.30±0.92 hours), followed by vaginal hysterectomy (2.86±0.24 hours), and the longest was for laparoscopic hysterectomy (4.14±0.90 hours) (p-value<0.0001). The size of the uterus was slightly larger in the abdominal hysterectomy group though the difference was not significantly different. There were no significant differences in pre- and post-operative hemoglobin, or in estimated blood loss among the groups. There were no complications in the vaginal group. The rate of complications was similar between the abdominal and laparoscopic groups (15.5% vs. 17.0% respectively). The most common type of intraoperative complication in the abdominal group was bleeding requiring transfusion (34.6%), followed by bladder injury (11.5%). Only one patient in the laparoscopic group had intra-operative complication (bladder injury). As for post-operative complications, urinary retention and pyrexia related to wound infection were the most common in the abdominal group (7.7%). Seven patients in the laparoscopic group had post-operative complications. Most patients were readmitted to the hospital (98.8% vs. 100.0% vs. 95.7% in the abdominal vs. vaginal vs. laparoscopic groups respectively).
Conclusion: Laparoscopic hysterectomy is associated with less morbidity, and shorter hospital stay than the other techniques, but it has longer operating time and requires laparoscopic instrument and surgical skills. Advances in equipment, surgical techniques, and training make laparoscopic hysterectomy an efficient and well-tolerated technique.
Introduction
Hysterectomy is one of the most common gynecological surgery worldwide [1]. In the United States more than 433,000 hysterecto-mies were performed during 2010 [1]. Over 56,000 hysterectomies were done in the United Kingdom in 2012 and around 305,000 in Germany between 2005 and 2006 [2,3]. The decision for hyster-ectomy is based on several factors such as indications for surgery, surgeon’s training and preference, uterine size, presence and ab¬sence of any associated pelvic pathologies, and patient’s choice [4].
In spite of the advances in laparoscopic techniques for hysterec-tomy, total abdominal hysterectomy remains the most common surgical approach in many countries, and the laparoscopic hyster¬ectomy rate is relatively low, ranging from 6% to 23% [1,2,5]. In the United States during 2010, the distribution of the surgical technique was 54.2% abdominal, 16.7% vaginal, and 8.6% laparo¬scopic hysterectomies [1]. Similarly, in the United Kingdom 62% of hysterectomies were abdominal, 32% vaginal, and 6% laparo¬scopic [2].
Many studies comparing abdominal and vaginal hysterectomy concluded that the vaginal route was the preferred approach since it was associated with shorter hospitalization, less operative and post-operative complications, faster recovery, and early mobi¬lization in comparison to abdominal hysterectomy [6-9]. Never¬theless, trends are changing and there is a growing acceptance of laparoscopic hysterectomy by many surgeons [10]. Several studies have shown that laparoscopic hysterectomy was a safe and effec¬tive technique associated with low complication rates, less blood loss and post-operative pain, as well as shorter hospital stay and quicker return to normal activities [11-13].
In light of the above, the aim of this study was to evaluate the role of total laparoscopic, vaginal and abdominal hysterectomy in the management of gynecological conditions in terms of operative outcomes, such as operating time and estimated blood loss, as well as complication rates.
Material and Method
This was a retrospective cohort study carried out over a 5-year pe¬riod (2016-2020) at Zahraa University Hospital. Patients who un¬derwent abdominal vaginal, and laparoscopic hysterectomies per¬formed for the treatment of multiple gynecological disease during that period were included. Data were collected retrospectively from the patients’ medical records. The abstracted data included the following: demographics, intra- and post- operative outcomes of patients such as age, body mass index (BMI), parity, mode of delivery (vaginal or cesarean section), indications for surgery, op¬erative time, uterine size, post-operative hemoglobin levels, esti¬mated blood loss and complications. Blood loss was measured by recording the contents of the fluid extraction device, which was used during the vaginal step, without any surgical pads.
All operations were performed in the lithotomy position. The drain was only used when indicated. The laparoscopic hysterectomies that were performed were according to the definitions by Reich and Roberts and modified by Johnson et al. [14,15].
Total Laparoscopic Hysterectomy
The uterus, including the cervix, was removed through the inci-sions or through the vagina.
Laparoscopic Supracervical Hysterectomy
The upper portion of the uterus was removed in pieces through the incisions, but the cervix remained in place.
Total Laparoscopic Hysterectomy with removal of ovaries
The uterus, ovaries, and fallopian tubes were removed through the vagina or the incisions.
During surgery, 10 mm laparoscope and advanced bipolar energy modalities were used. Including umbilicus 3 laparoscopic trocar were inserted. First, 10 mm trocar was inserted directly in 1 cm incision which was on sub umbilical area. The laparoscope was placed in abdomen after 3-4 L CO2 insufflation into the abdominal cavity. Second and third incisions were made on avascular right and left lower abdomen and two 5 mm trocars were placed in the abdomen.
Laparoscopic Hysterectomy Was Done Using Standard Technique with Few Specific Steps:
1. Mobilize the bladder: The anterior and posterior leaves of the broad ligament were separated with the help of Maryland for¬ceps (Figure 1a).
2. The vesicouterine peritoneal fold was identified and hydro dissection was done in which 20-30 ml of saline was intro-duced with needle in the vesicouterine space for dissection of bladder (Figure 1b).
(A) (B)


Figure 1: a) mobilizing the bladder, b) identifying vesicouterine peritoneal fold and performing hydro dissection
3. Identification of vesicouterine space and dissection of bladder with separation from uterus (Figure 2a).
4. we used LigaSure™ V 5 mm to seal and cut the uterine ves-sels and infundibulopelvic ligaments instead of using the bi-polar cautery (Figure 2b).
(A) (B)


Figure 2: a) dissection of bladder with separation from uterus, b) sealing and cutting the uterine vessels
5. In the vaginal step of the laparoscopic procedure, Ligasure Vmax was used. In total laparospic hysterectomy uterosacral and cardinal ligaments were also sealed and cut with the Li¬gasure followed by a circular incision of the vagina using the hook unipolar cautery and the uterus was removed (Figure 3 a, b, c)
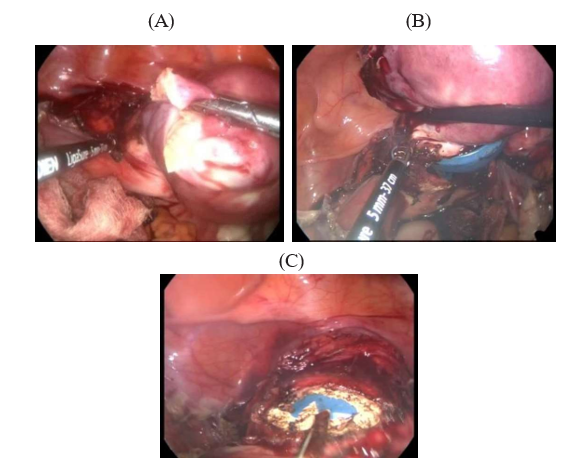
Figure 3: Uterosacral and cardinal ligaments were sealed and cut with the Ligasure followed by a circular incision of the vagina using the hook unipolar cautery
The vagina was also sutured laparoscopically. Vaginal cuff closure was done with the help of vicryl no 1 taking eight stitches one at each angle and one at the center.
As for vaginal surgery, it was performed to patients with uterine prolapse, unenlarged uterus, at least one vaginal birth, and without prior abdominal surgery. For large uteri, total abdominal hyster-ectomy was used. The techniques of total abdominal and vaginal procedures were similar to those described in TeLinde’s Operative Gynecology [16]. All surgeries were performed by attending and senior gynecologists. All cases were operated under spinal and epi¬dural or general anesthesia as decided by the anesthetist whichever was best for individual case. Post-operative management includ¬ed IV fluids for 24-36 hours to maintain hydration. Catheter was kept in situ for 24 hours in the majority of patients. Antibiotics were given parenterally for 2 days and then orally for 5 days to prevent infection. Adequate analgesics were given. Patients who underwent laparoscopic hysterectomy were discharged from the hospital after 24 hours, while those who had vaginal hysterectomy were discharged after 48 hours and those with abdominal hyster¬ectomy after 72 hours.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS, version 24) was used for analysis. Bivariate analysis was carried out by using the Chi square test for comparing categorical variables. Continuous variables were compared using One-way Anova. Categorical vari¬ables were presented as number and percent, whereas continuous variables were presented as mean and standard deviation. P-value of <0.05 was used to indicate statistical significance.
Results
A total of 222 patients were included in the study, 168 (75.7%) patients in the abdominal hysterectomy group, 7 (3.2%) in the vag-inal group, and 47 (21.1%) in the laparoscopic group. Patients’ characteristics are presented in Table 1. The mean age was sig-nificantly higher in the vaginal group compared to the other two groups (49.83±9.28 years for the abdominal, 67.14±13.79 for the vaginal, and 47.26±6.77 years for the hysterectomy groups, p-val-ue<0.0001). There were no significant differences in the parity and BMI between the groups. The majority of women were multipa-rous and were Lebanese. Around 49% had all previous delivery by NVD in the abdominal group, 85.7% in the vaginal group, and 68.1% in the laparoscopic group (p-value=0.09) (Table 1).
The most common indication for hysterectomy was the presence of uterine fibroids in the abdominal and laparoscopic groups (47.6% vs. 31.9% respectively). On the other hand, the indication for hysterectomy for all patients in the vaginal group was pelvic organ prolapse. Around 18% in the abdominal group had abnormal uterine bleeding compared to 6.4% in the laparoscopic group. En¬dometrial hyperplasia was the indication for 9.5% of the patients in the abdominal group whereas it was 25.5% for the laparoscopic group (Table 2).
Table 1: Patients’ characteristics
|
|
|
Abdominal (n=168) |
Vaginal (n=7) |
Laparoscopic (n=47) |
p-value |
|
Age |
Years |
49.83±9.28 |
67.14±13.79 |
47.26±6.77 |
<0.0001 |
|
BMI |
Kg/m2 |
29.85±7.37 |
29.10±2.94 |
31.07±7.92 |
0.57 |
|
Parity |
Nulli parous |
27 (16.1%) |
0 (0.0%) |
2 (4.3%) |
0.06 |
|
Multi parous |
141 (83.9%) |
7 (100.0%) |
45 (95.7%) |
||
|
Gravida |
0 |
27 (16.1%) |
0 (0.0%) |
2 (4.3%) |
0.07 |
|
1 |
10 (6.0%) |
0 (0.0%) |
2 (4.3%) |
||
|
2 |
16 (9.5%) |
0 (0.0%) |
8 (17.0%) |
||
|
3 |
29 (17.3%) |
0 (0.0%) |
7 (14.9%) |
||
|
4 |
28 (16.7%) |
2 (28.6%) |
9 (19.1%) |
||
|
5 |
24 (14.3%) |
0 (0.0%) |
9 (19.1%) |
||
|
≥6 |
34 (20.2%) |
5 (71.4%) |
10 (21.3%) |
||
|
Para |
0 |
29 (17.3%) |
0 (0.0%) |
2 (4.3%) |
0.17 |
|
1 |
12 (7.1%) |
0 (0.0%) |
3 (6.4%) |
||
|
2 |
27 (16.1%) |
0 (0.0%) |
9 (19.1%) |
||
|
3 |
32 (19.0%) |
1 (14.3%) |
14 (29.8%) |
||
|
4 |
34 (20.2%) |
2 (28.6%) |
11 (23.4%) |
||
|
5 |
16 (9.5%) |
1 (14.3%) |
3 (6.4%) |
||
|
≥6 |
18 (10.7%) |
3 (42.9%) |
5 (10.6%) |
||
|
Abortion |
0 |
112 (66.7%) |
3 (42.9%) |
29 (61.7%) |
0.47 |
|
1 |
29 (17.3%) |
1 (14.3%) |
2 (4.3%) |
||
|
2 |
14 (8.3%) |
2 (28.6%) |
9 (19.1%) |
||
|
3 |
6 (3.6%) |
1 (14.3%) |
2 (4.3%) |
||
|
4 |
1 (0.6%) |
0 (0.0%) |
1 (2.1%) |
||
|
5 |
3 (1.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
≥6 |
3 (1.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Nationality |
Lebanese |
168 (100.0%) |
7 (100.0%) |
44 (93.6%) |
0.003 |
|
Iraqi |
0 (0.0%) |
0 (0.0%) |
3 (6.4%) |
||
|
Previous delivery |
None |
29 (17.3%) |
0 (0.0%) |
2 (4.3%) |
0.09 |
|
NVD |
83 (49.4%) |
6 (85.7%) |
32 (68.1%) |
||
|
CS |
36 (21.4%) |
1 (14.3%) |
10 (21.3%) |
||
|
NVD & CS |
20 (11.9%) |
0 (0.0%) |
3 (6.4%) |
Table 2: Indications for hysterectomy
|
|
Abdominal (n=168) |
Vaginal (n=7) |
Laparoscopic (n=47) |
p-value |
|
Uterine fibroids |
80 (47.6%) |
0 (0.0%) |
15 (31.9%) |
<0.0001 |
|
Endometrial cancer |
9 (5.4%) |
0 (0.0%) |
1 (2.1%) |
|
|
Ovarian cancer |
5 (3.0%) |
0 (0.0%) |
1 (2.1%) |
|
|
BRCA 1 & 2 + |
1 (0.6%) |
0 (0.0%) |
0 (0.0%) |
|
|
Cervical cancer |
4 (2.4%) |
0 (0.0%) |
0 (0.0%) |
|
|
Cervical high grade lesion |
1 (0.6%) |
0 (0.0%) |
2 (4.3%) |
|
|
Pelvic organ prolapse |
2 (1.2%) |
7 (100.0%) |
2 (4.3%) |
|
|
Endometrial hyperplasia |
16 (9.5%) |
0 (0.0%) |
12 (25.5%) |
|
|
Abnormal uterine bleeding |
30 (17.9%) |
0 (0.0%) |
3 (6.4%) |
|
|
Adenomyosis |
11 (6.5%) |
0 (0.0%) |
7 (14.9%) |
|
|
Adnexal mass |
5 (3.0%) |
0 (0.0%) |
0 (0.0%) |
|
|
Endometrial polyp |
2 (1.2%) |
0 (0.0%) |
4 (8.5%) |
|
|
Abnormally adherent placenta |
2 (1.2%) |
0 (0.0%) |
0 (0.0%)
|
Regarding the outcomes, surgery duration was significantly the shortest for abdominal hysterectomy (2.30±0.92 hours), fol¬lowed by vaginal hysterectomy (2.86±0.24 hours), and the lon¬gest was for laparoscopic hysterectomy (4.14±0.90 hours) (p-val-ue<0.0001) (Table 3). The size of the uterus was slightly larger in the abdominal hysterectomy group though the difference was not significantly different.
There were no significant differences in pre-and post-operative hemoglobin, or in estimated blood loss among the groups (Table 3). There were no complications in the vaginal group. The rate of complications was similar between the abdominal and laparo-scopic groups (15.5% vs. 17.0% respectively) (Table 3). The most common type of intraoperative complication in the abdominal group was bleeding requiring transfusion (34.6%), followed by bladder injury (11.5%), ovarian torsion (3.8%), sigmoid injury (3.8%), rectal injury (3.8%) requiring surgeon intervention and treatment with appendectomy. On the other hand, only one patient in the laparoscopic group had intra-operative complication (blad¬der injury) (Table 3).
As for post-operative complications, urinary retention and pyrexia related to wound infection were the most common in the abdomi¬nal hysterectomy group (7.7%), followed by ilius (3.8%), oliguria (3.8%), subcutaneous hematoma (3.8%), vault hematoma (3.8%), vesicovaginal fistula (3.8%), and intestinal perforation (3.8%). Subcutaneous hematoma was conservatively managed with an¬ti-inflammatory drugs while vault hematoma required surgical intervention (suturing the vaginal route). On the other hand, 7 pa¬tients in the laparoscopic group had post-operative complications. These were ileus (25.0%), oliguria (25.0%), pyrexia (12.5%), atonic bladder (12.5%), and vesicovaginal fistula (12.5%) (Ta¬ble 3). Most patients were readmitted to the hospital (98.8% vs. 100.0% vs. 95.7% in the abdominal vs. vaginal vs. laparoscopic groups respectively) (Table 3).
Table 3: Patients’ outcomes
|
|
|
Abdominal (n=168) |
Vaginal (n=7) |
Laparoscopic(n=47) |
p-value |
|
Surgery duration |
Hours |
2.30±0.92 |
2.86±0.24 |
4.14±0.90 |
<0.0001 |
|
Size of uterus |
cm |
11.88±3.14 |
10.14±1.07 |
10.94±1.22 |
0.05 |
|
Pre-operative hemoglobin |
g/dl |
11.80±2.24 |
12.60±1.65 |
12.40±1.87 |
0.17 |
|
Post-operative hemoglobin |
g/dl |
10.82±1.47 |
11.00±2.02 |
10.90±1.41 |
0.90 |
|
Estimated blood loss |
ml |
199.70±206.88 |
135.71±80.18 |
174.47±131.41 |
0.53 |
|
Complications |
No |
142 (84.5%) |
7 (100.0%) |
39 (83.0%) |
0.50 |
|
Yes |
26 (15.5%) |
0 (0.0%) |
8 (17.0%) |
|
Intra-operative complication type |
Bleeding/transfusion |
9 (34.6%) |
0 (0.0%) |
0 (0.0%) |
0.23 |
|
Bladder injury |
3 (11.5%) |
0 (0.0%) |
1 (12.5%) |
||
|
Ovarian torsion |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Appendicitis |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Sigmoid injury |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Rectal injury |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Hypertensive crisis needed ICU |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Post-operative complication type |
Urinary retention |
2 (7.7%) |
0 (0.0%) |
0 (0.0%) |
|
|
Ileus |
1 (3.8%) |
0 (0.0%) |
2 (25.0%) |
||
|
Oliguria |
1 (3.8%) |
0 (0.0%) |
2 (25.0%) |
||
|
Pyrexia (>380C) related to wound infection |
2 (7.7%) |
0 (0.0%) |
1 (12.5%) |
||
|
Subcutaneous hematoma |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Vault hematoma |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Atonic bladder |
0 (0.0%) |
0 (0.0%) |
1 (12.5%) |
||
|
Vesicovaginal fistula |
0 (0.0%) |
0 (0.0%) |
1 (12.5%) |
||
|
Intestinal perforation |
1 (3.8%) |
0 (0.0%) |
0 (0.0%) |
||
|
Admission |
Once |
166 (98.8%) |
7 (100.0%) |
45 (95.7%) |
0.35 |
|
Twice |
2 (1.2%) |
0 (0.0%) |
2 (4.3%) |
Discussion
The results of the present study showed that during the past five years, 222 patients underwent hysterectomy at our institution. Of those, 75.7% had abdominal, 21.1% had laparoscopic and 3.2% had vaginal hysterectomy. Studies have shown that there are dif-ferences in the medical and economic outcomes of abdominal, vaginal, and laparoscopic hysterectomies [4,15]. Usually, the type of surgery depends on the experience of the operating surgeon and on underlying pathology [12]. The decision should be the optimal one for a given patient under specific circumstances [17]. In the present study the mean age was significantly the highest in the vaginal group (67.14±13.79 years), followed by 49.83±9.28 years in the abdominal, and 47.26±6.77 years in the hysterectomy groups (p-value<0.0001). Nevertheless, most hysterectomies are done in peri-menopausal age group. In a study conducted by Panda et al, the mean age for patients who underwent abdominal, vaginal and laparoscopic hysterectomy was 40.84 years, 41.44 years and 44.57 years respectively [18]. In the current study, parity and BMI were comparable in all three groups. In a study conducted by Er-can et al, the mean BMI was 26.1, 26.6 and 26.2 in the laparoscop-ic, abdominal, and vaginal groups respectively [19].
In the present study, the most common indication for hysterectomy was the presence of uterine fibroids in the abdominal and laparo¬scopic groups (47.6% vs. 31.9% respectively). Around 18% in the abdominal group had indication abnormal uterine bleeding com- pared to 6.4% in the laparoscopic group, while 9.5% had hyperpla¬sia as an indication in the abdominal group compared to 25.5% in the laparoscopic group. A study by Aboulfotouh et al reported that the most frequent indications for hysterectomy in the laparoscop¬ic group were endometrial hyperplasia (43.9%), fibroids (24.4%), and abnormal uterine bleeding (9.8%). While in the abdominal hysterectomy group, the most common indications were fibroids (62%), abnormal uterine bleeding (18.9%), and endometrial hy¬perplasia (6.3%) [12], Regarding the outcomes, surgery duration was significantly the shortest for abdominal hysterectomy (2.30±0.92 hours), followed by vaginal hysterectomy (2.86±0.24 hours), and the longest was for laparoscopic hysterectomy (4.14±0.90 hours) (p-value<0.0001). Panda et al also reported that the mean operating time was the longest in the laparoscopic group (124.56±19.49 min), followed by (64.14±10.69 min) in the vaginal group, and (61.26±10.49 min) in the abdominal hysterectomy group [18]. Patel et al mentioned that surgery duration was 190 min for laparoscopic, 97.28 min for abdominal and 97.71 min for vaginal hysterectomy [20]. However, their surgery duration was shorter than the duration in our study.
In the current study, the size of the uterus was slightly larger in the abdominal hysterectomy group though the difference was not significantly different (11.88±3.14 cm vs. 10.14±1.07 cm vs. 10.94±1.22 cm for the abdominal, vaginal, and laparoscopic groups respectively). In the study by Aboulfotouh et al, size of the uterus was significantly smaller in the laparoscopic group com¬pared to the abdominal group (7.38 ± 1.92 vs 10.25 ± 3.84 cm, respectively). This could be due to selection bias by the gynecolo¬gists since many prefer performing laparoscopic hysterectomy on small uteri while those with larger uteri will be more likely to have their hysterectomies done via abdominal route [12].
In the present study, there were no significant differences in the post-operative hemoglobin among the groups (10.82±1.47 g/dl, 11.00±2.02 g/dl, 10.90±1.41 g/dl for abdominal, vaginal and lapa¬roscopic groups respectively). These results were similar to those reported by Aboulfotouh et al and Tomov et al. [12,21]. More¬over, there were no significant differences in estimated blood loss among the groups of our study though the loss was slightly higher in the abdominal group (199.70±206.88 ml) compared to the vag¬inal (135.71±80.18 ml) and laparoscopic group (174.47±131.41 ml). A study by Uikey and colleagues reported that the estimated blood loss was 328.0±70.1ml, 192.0±21.1 ml, and 120.5± 43.7 ml in the abdominal, vaginal and laparoscopic groups respectively, indicating that the blood loss was greater in the abdominal group than the other groups [22].
In the current study, some intraoperative complications occurred in the abdominal and laparoscopic hysterectomy groups. Nine (34.6%) patients in the abdominal group had bleeding requiring blood transfusion compared to none in the laparoscopic group, whereas 3 (11.5%) cases in the abdominal group had bladder in-jury compared to 1 case (12.5%) in the laparoscopic group. Other reported complications in the abdominal group were bowel inju-ries. In the study by Uikey et al, blood transfusion was required intraoperatively in 6 cases of the abdominal group, 1 case of the vaginal group, and 2 cases of the laparoscopic group. Unlike our study, they did not report bladder, bowel or ureteric injury [22]. In a study by Panda et al, 3 cases in the abdominal group had hemor¬rhage requiring blood transfusion compared to 2 cases in the lapa¬roscopic group. A single case in the laparoscopic group had bowel injury while urinary tract injury occurred in one case in the abdom¬inal group and another case in the vaginal group [18]. Tomov and colleagues described that 5 cases in the laparoscopic group had bladder injury and 9 cases had bleeding compared to 1 and 2 cases in the abdominal group respectively [21]. Karaman et el concluded that the laparoscopic route is safe and effective in the prevention of ureteral, vesical, and vascular injuries [23].
With regards to overall postoperative complications, in the abdom-inal group, 2 patients had urinary retention, 2 had pyrexia relat¬ed to wound infection, 1 had ilius, 1 oliguria, 1 vault hematoma and 1 intestinal perforation. Whereas in the laparoscopic group, 2 cases had ilius, 2 had oliguria, 1 pyrexia, 1 atonic bladder and 1 vesicovaginal fistula. Tomov et al mentioned that 8 patients in the abdominal group had wound infection [21]. Uikey et al reported that fever and wound discharge were more common in the abdom-inal group. None of their patients had urinary retention or vault hematoma [22]. Panda et al had 6 cases of wound sepsis and 2 cas¬es of vault hematoma in the abdominal group [18]. Laparoscopic hysterectomy was found to be associated with a lower risk of vault dehiscence compared with abdominal hysterectomy [24].
With respect to hospital stay, patients who underwent laparoscop¬ic hysterectomy had the least hospitalization duration since they were discharged after 24 hours while patients who had abdominal hysterectomy had the longest stay as they were discharged after 48 hours. Hospital stay would be shorter when surgery is performed by the minimally invasive route [11,25]. Pather et al. reported that hospital stay was shorter in the laparoscopic group versus the ab¬dominal group (1.82 vs 2.62 days respectively) [25]. Aboulfotouh et al also concluded that laparoscopic hysterectomy group had significantly less length of stay compared to the abdominal group (3.63 ± 1.28 vs 5.22 ± 4 days, respectively) [12]. In the study by Panda et al, the mean duration of hospital stay was 4.78 days in the laparoscopic group, 5.08 days in the vaginal and 8 days in the abdominal group [18]. As for post-operative pain, although it was not assessed in this study, several studies have shown that laparo¬scopic hysterectomy was associated with lower pain and analgesic consumption compared to abdominal hysterectomy [12,13,26].
Conclusion
Laparoscopic hysterectomy is associated with small scar, less morbidity, and shorter hospital stay than the other techniques. It could be a better route of surgery in obese patients in whom vag¬inal hysterectomy may be difficult. It could be an alternative to abdominal hysterectomy for those in whom the vaginal route is not feasible. It may be comparable to vaginal hysterectomy in terms of post-operative parameters, but it has longer operating time and requires laparoscopic instrument and surgical skills. In order to in¬crease the use of the laparoscopic route in Lebanon, improvement in terms of surgical training and mentorship is required. Advances in equipment, surgical techniques, and training make laparoscopic hysterectomy an efficient and well-tolerated technique.
References
- Wright JD, Herzog TJ, Tsui J, Ananth CV, Lewin SN, et al (2013). Nationwide trends in the performance of inpatient hysterectomy in the United States. Obstetrics and Gynecology 122: 233-241.
- Allam M, Ewies AA (2016) Centres that do not offer TLH as their primary method of hysterectomy should be considered outdated and not fit for purpose: FOR: it is a patient’s right to be offered laparoscopic surgery as an informed choice. BJOG: British Journal of Obstetrics & Gynaecology 123: 1192.
- Stang A, Merrill RM, Kuss O (2011) Hysterectomy in Germany: a DRG-based nationwide analysis, 2005–2006. Deutsches Ärzteblatt International 108: 508.
- Aarts JW, Nieboer TE, Johnson N, Tavender E, Garry R, et al.(2015) Surgical approach to hysterectomy for benign gynae-cological disease. Cochrane Database of Systematic Reviews8.
- Edler KM, Tamussino K, Fülöp G, Reinstadler E, Neunteufel W, et al. (2017) Rates and routes of hysterectomy for benign indications in Austria 2002–2014. Geburtshilfe und Frauen-heilkunde 77: 482-486.
- Chen B, Ren DP, Li JX, Li CD (2014) Comparison of vaginal and abdominal hysterectomy: A prospective non-randomized trial. Pakistan Journal of Medical Sciences 30: 875-879.
- Shanthini NF, Poomalar GK, Jayasree M, Bupathy A (2012) Evaluation of complications of abdominal and vaginal hysterectomy. International Journal of Reproduction, Contraception, Obstetrics & Gynecology 1: 7-11.
- Balakrishnan D, Dibyajyoti G (2016) A comparison between non-descent vaginal hysterectomy and total abdominal hysterectomy. Journal of Clinical and Diagnostic Research 10: 11-14.
- Fatania K, Vithayathil M, Newbold P, Yoong W (2014) Vaginal versus abdominal hysterectomy for the enlarged non-pro-lapsed uterus: a retrospective cohort study. European Journal of Obstetrics & Gynecology and Reproductive Biology 174: 111-114.
- Jonsdottir GM, Jorgensen S, Cohen SL, Wright KN, Shah NT, et al. (2011) Increasing minimally invasive hysterectomy: effect on cost and complications. Obstetrics & Gynecology 117: 1142-1149.
- Yi YX, Zhang W, Zhou Q, Guo WR, Su Y (2011) Laparoscopic-assisted vaginal hysterectomy vs abdominal hysterectomy for benign disease: a meta-analysis of randomized controlled trials. European Journal of Obstetrics & Gynecology and Reproductive Biology 159: 1-18.
- Aboulfotouh ME, Chaalan F, Mohammed AF (2020) Laparoscopic hysterectomy versus total abdominal hysterectomy: a retrospective study at a tertiary hospital. Gynecological Surgery 17: 1-5.
- Mallick R, English J, Waters N (2016) Total laparoscopic hysterectomy versus total abdominal hysterectomy in the treatment of benign gynecological disease: a retrospective review over 5 years. Gynecological Surgery 13: 359-364.
- Reich H, Roberts L (2003) Laparoscopic hysterectomy in current gynecological practice. Reviews in Gynaecological Practice 3: 32-40
- Johnson N, Barlow D, Lethaby A, Tavender E, Curr L, et al.(2005) Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials. British MedicalJournal 330: 1478.
- Rock JA, Jones HW, editors. TeLinde’s Operative Gynecology. 9th ed. Philadelphia
- Kovac R (2013) Evidence based hysterectomy. Gynecology &Obstetrics 3: e110.
- Panda S, Behera AK, Jayalakshmi M, Rao TN, Indira G (2015) Choosing the route of hysterectomy. The Journal of Obstetrics and Gynecology of India 65: 251-254.
- Ercan Ö, Özer A, Köstü B, Bakacak M, Kıran G, et al. (2016) Comparison of postoperative vaginal length and sexual function after abdominal, vaginal, and laparoscopic hysterectomy. International Journal of Gynecology & Obstetrics 132: 39-41.
- Patel R, Chakravarty N (2014) Comparative study of laparoscopic hysterectomy versus vaginal hysterectomy. International Journal of Medical Science and Public Health 3:335-337.
- Tomov ST, Gortchev GA, Tantchev LS, Dimitrov TI, Tzvet-kov CA, et al. (2015) Perioperative Outcomes of Laparoscopic Hysterectomy: Comparison with Abdominal, Vaginal, And Robot-Assisted Surgical Approaches. Journal of Biomedical and Clinical Research 8: 52-60.
- Uikey P, Wankhede TM, Tajne MP (2018) The route of hysterectomy: a comparative study between abdominal hysterectomy (AH), non-descent vaginal hysterectomy (NDVH), and laparoscopic assisted vaginal hysterectomy (LAVH). International Journal of Reproduction, Contraception, Obstetrics & Gynecology 7: 4022-4028.
- Karaman Y, Bingol B, Gunenc Z (2007) Prevention of complications in laparoscopic hysterectomy: experience with 1120 cases performed by a single surgeon. Journal of Minimally Invasive Gynecology 14: 78-84.
- Koo YJ, Kim DY, Kim JH, Kim YM, Kim YT, et al. (2013) Vaginal cuff dehiscence after hysterectomy. International Journal of Gynecology & Obstetrics 122: 248-252.
- Pather S, Loadsman JA, Mansfield C, Rao A, Arora V, et al. (2011) Perioperative outcomes after total laparoscopic hysterectomy compared with fastâ?track open hysterectomy–A retrospective case–control study. Australian and New Zealand Journal of Obstetrics and Gynaecology 51: 393-396.
- Ghezzi F, Uccella S, Cromi A, Siesto G, Serati M, et al. (2010) Postoperative pain after laparoscopic and vaginal hysterectomy for benign gynecologic disease: a randomized trial. American Journal of Obstetrics and Gynecology 203: 118.e1-8.