
Journal of Clinical, Medical, and Diagnostic Research(JCMDR)
ISSN: 3065-9817 | DOI: 10.33140/JCMDR

Review Article - (2025) Volume 3, Issue 1
Combined Fractures of The Odontoid Process and Upper Thoracic Spine: A Case Report
2Zonguldak Bülent Ecevit University, School of Medicine, 67600 Zonguldak, Turkey
3Private Lösante children and adult hospital, Ankara, Turkey
Received Date: May 15, 2025 / Accepted Date: Jun 23, 2025 / Published Date: Jun 25, 2025
Copyright: ©Ã?©2025 Hasan Ali AYDIN, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: AYDIN, H, A. EDEBALI, N.(2025). Combined Fractures of The Odontoid Process and Upper Thoracic Spine: A Case Report. J of Cli Med Dia Research, 3(1), 01-03
Abstract
A 39-year-old male patient sustained a rare combination of a posteriorly displaced Type II odontoid fracture and a T5 rotational burst fracture after falling 4 meters. Despite the patient's significant spinal trauma, no neurological deficits were observed. The surgical intervention, which included anterior odontoid screw fixation and T1-T7 posterior fusion, was performed on the first post-injury day and was successfully completed. This case underscores the pivotal role of hyperextension and flexion-rotation forces in such injuries, while concurrently demonstrating the efficacy of combined surgical approaches in preserving neurological function in multilevel spinal trauma.
Keywords
Odontoid Fracture, Thoracic Fracture, Spinal Trauma, Surgical Stabilization
Introduction
Concomitant fractures of the odontoid process and upper thoracic spine are exceptionally rare, with few reports in the literature [1,2]. The odontoid process, a critical stabilizer of the atlantoaxial joint, is vulnerable to high-energy trauma, while the upper thoracic spine, reinforced by the rib cage, typically requires significant force to fracture [3]. This particular case under consideration presents a unique combination of a Type II odontoid fracture and a T5 burst fracture-dislocation. Notably, these injuries were managed successfully without neurological compromise. This case offers insights into injury biomechanics and the role of tailored surgical strategies in complex spinal injuries.
Case Report
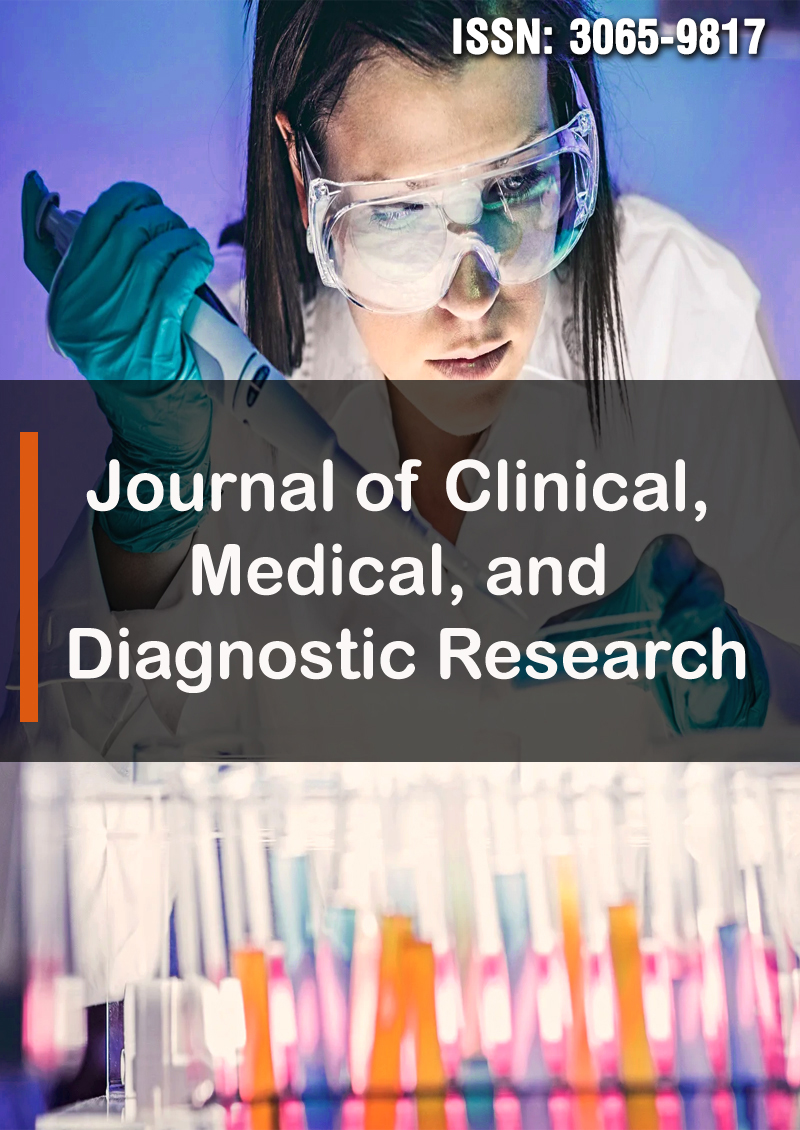
A 39-year-old male presented to the emergency department after sustaining a 4-meter fall from a roof on June 3, 2013. On arrival, the patient was conscious with a Glasgow Coma Score of 15 and exhibited no neurological deficits. Cervical and thoracic imaging revealed a posteriorly displaced Type II odontoid fracture (Anderson and D'Alonzo classification) and a T5 rotational burst fracture-dislocation [4]. Cervical CT imaging confirmed posterior displacement of the odontoid (see Figure 1), while thoracic CT imaging revealed a T5 rotational burst fracture with minimal canal encroachment. (see Figures 2 and 3). No additional fractures were identified.
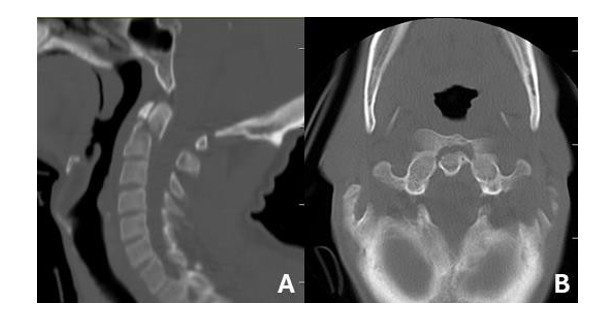
Figure 1: (A) sagittal and (B) axial CT showing a posteriorly displaced Type II odontoid fracture
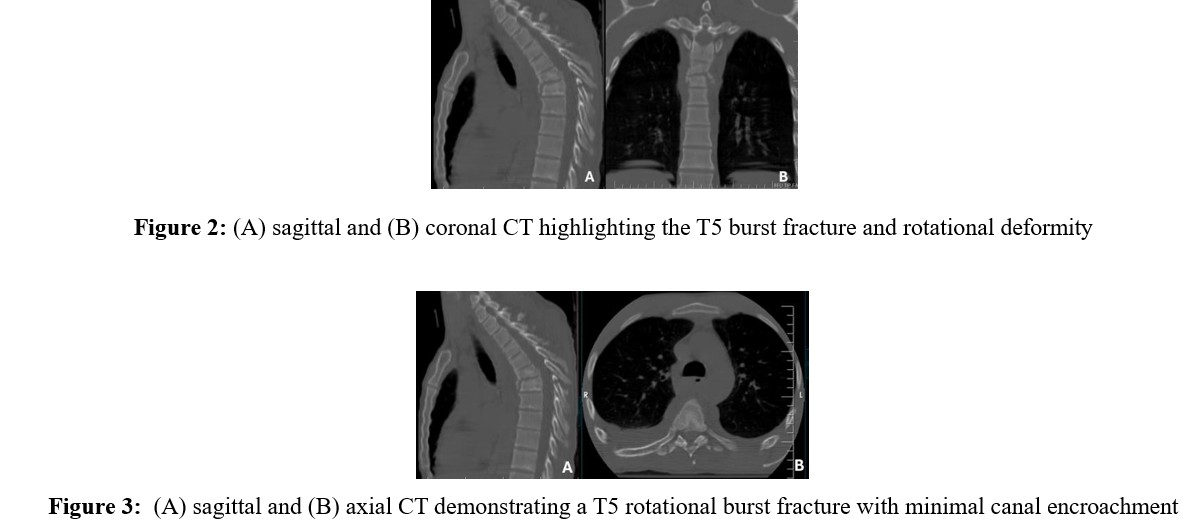
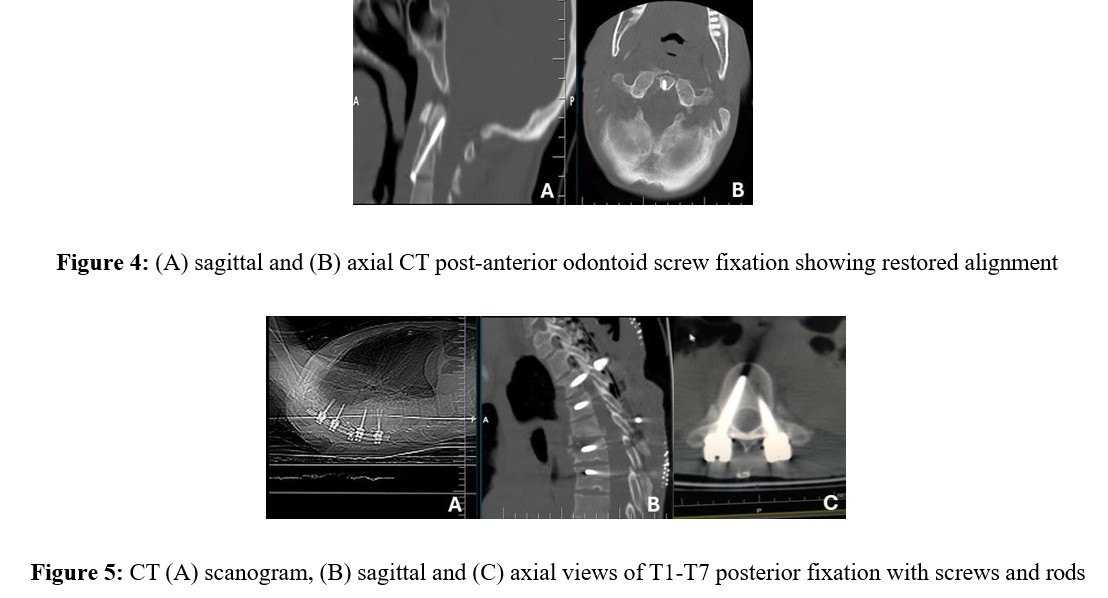
The surgical intervention was performed on the first post-injury day. The odontoid fracture was stabilized by means of anterior odontoid screw fixation (Figure 4). The upper thoracic spine was addressed via a posterior approach, with the placement of polyaxial screws and rods at T3, T4, T6, and T7, spanning T1- T7 (Figure 5). T5 was not instrumented. Postoperative imaging confirmed satisfactory alignment and fixation. Informed consent was obtained from the patient for the publication of this report.
Discussion
The occurrence of combined fractures of the odontoid process and upper thoracic spine is an uncommon phenomenon, indicative of distinct biomechanical forces. The posterior displacement of the Type II odontoid fracture suggests cervical hyperextension, which is consistent with the mechanisms described by Rogers et al. [1]. These researchers reported associated cervical injuries in 35 upper thoracic fracture cases. Conversely, the T5 rotational burst fracture is hypothesized to have resulted from sudden flexion-rotation forces, a pattern associated with high-energy trauma [3,5]. The stability of the upper thoracic spine, which is facilitated by the rib cage, typically necessitates substantial energy for injury, often leading to neurological deficits in 85% of cases [6]. The patient's remarkable resilience in maintaining neurological integrity in the face of such a severe injury is noteworthy.The absence of spinal cord injury despite the narrow upper thoracic canal may be attributed to limited canal intrusion by fracture fragments, akin to osteoporotic vertebra plana. Biomechanical studies suggest that axial loading in burst fractures can be mitigated by degenerated discs or reduced bone mass, decreasing canal encroachment [9]. In this case, the rotational component and minimal fragment displacement likely spared the cord, aligning with findings from modern imaging analyses of thoracic trauma [10].
A surgical approach that combines anterior odontoid fixation with posterior thoracic stabilization is recommended, as supported by recent literature on multilevel spinal injuries [11]. Anterior screw fixation effectively restores C1-C2 stability in Type II odontoid fractures, while posterior fusion addresses the instability and rotational deformity at T5 [12]. This dual approach stands in contrast to single-level fixation studies, underscoring the necessity for individualized treatment in complex cases [13]. The postoperative outcomes further substantiate the efficacy of this strategy, with no complications observed.This case contributes to the understanding of multilevel spinal trauma by illustrating a rare injury pattern and its successful management. It underscores the protective role of biomechanical factors in neurological preservation and the value of combined stabilization techniques, aligning with contemporary trends in spinal surgery [14].
Conclusion
This exceptional instance of concomitant odontoid and T5 fractures exemplifies the viability of combined anterior-posterior stabilization and underscores the necessity of comprehending injury biomechanics to enhance outcomes in intricate spinal trauma cases [7,8].
References
- Rogers, L. F., Thayer, C., Weinberg, P. E., & Kim, K. S. (1980). Acute injuries of the upper thoracic spine associated with paraplegia. American Journal of Roentgenology, 134(1), 67-73.
- Suh, B. G., Uh, J. H., Park, S. H., & Lee, G. W. (2015). Repair using conventional implant for ruptured annulus fibrosus after lumbar discectomy: surgical technique and case series. Asian spine journal, 9(1), 14.
- Vialle LR, Vialle EN, Santoro SM, et al. Biomechanics of thoracic spine fractures: an update. Eur Spine J. 2018;27(Suppl 1):12-8.
- Anderson, L. D., & D'ALONZO, R. T. (1974). Fractures of the odontoid process of the axis. JBJS, 56(8), 1663-1674.
- Denis, F. (1983). The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. spine, 8(8), 817-831.
- Bohlman, H. H., Freehafer, A., & Dejak, J. (1985). The results of treatment of acute injuries of the upper thoracic spine with paralysis. JBJS, 67(3), 360-369.
- Kim KC, Lee HS, Cho BK. Anatomical considerations of the thoracic spinal canal in trauma. Spine J. 2016;16(9):1055-61.
- Kaneda, K., Asano, S., Hashimoto, T., Satoh, S., & Fujiya, M. (1992). The treatment of osteoporotic–posttraumatic vertebral collapse using the Kaneda device and a bioactive ceramic vertebral prosthesis. Spine, 17, 295-303.
- Tran NT, Watson NA, Tencer AF, et al. Mechanism of thoracolumbar burst fractures: a biomechanical study. Spine. 2014;39(16):E964-70.
- Rajasekaran, S., Kanna, R. M., & Shetty, A. P. (2015). Management of thoracolumbar spine trauma: An overview. Indian journal of orthopaedics, 49(1), 72-82.
- Joaquim AF, Patel AA, Schroeder GD, et al. Multilevel spinal injuries: evaluation and treatment. Neurosurg Clin N Am. 2021;32(3):377-86.
- Apfelbaum, R. I., Lonser, R. R., Veres, R., & Casey, A. (2000). Direct anterior screw fixation for recent and remote odontoid fractures. Neurosurgical Focus, 8(6), 1-10.
- Kepler CK, Vaccaro AR, Fleischman AN, et al. Treatment of axis fractures: current concepts. Spine J. 2019;19(5):917-25.
- Phan K, Mobbs RJ. Evolution of spinal trauma management: a review of current practices. J Clin Neurosci. 2020;74:1-6.