

Research Article - (2025) Volume 10, Issue 4
Cognitive Impairment Among Stroke Survivors at the University of Calabar Teaching Hospitalcalabar Cross River State, Nigeria
2Sam Remo Nursing and Rehabilitation Centre, USA
Received Date: Oct 29, 2025 / Accepted Date: Nov 19, 2025 / Published Date: Dec 01, 2025
Copyright: ©2025 Israel Ebubechukwu Okeke, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Okeke, I. E., Nwosu, P. C., Uma, U. A., Essien, E. A., Uwah, E. E. (2025). Cognitive Impairment Among Stroke Survivors at the University of Calabar Teaching Hospitalcalabar Cross River State, Nigeria. Int J Psychiatry, 10(4), 01-15.
Abstract
Background: Post-stroke cognitive impairment is very prevalent among stroke survivors but is often missed or underdiagnosed. Previous studies in Nigeria have focused more on post-stroke depression, leading to a shortage of information on cognitive impairment after stroke.
Aim: To investigate the occurrence of post-stroke cognitive impairment among stroke survivors at the University of Calabar Teaching Hospital (UCTH), Calabar, Nigeria.
Materials and Methods: This cross-sectional study was conducted among stroke survivors at the University of Calabar Teaching Hospital. All the stroke survivors had a CT-scan confirmed stroke. A consecutive sampling method was used to recruit respondents. The following questionnaires were administered to 122 stroke survivors. Sociodemographic/clinical questionnaire, National Institute of Health Stroke Scale (NIHSS), The Mini-International Neuropsychiatry Interview (MINI)-Depression module, Mini-Mental State Examination (MMSE), Oslo Social Support Scale (OSSS-3), and the Modified Rankin Scale (MRS). The data were analysed using SPSS version 25.
Results: The study recruited 122 stroke survivors. The mean age of the participants was 60.23 ± 13.0. The proportion of male respondents was 62.3%, while that of female respondents was 37.7%. Respondents with the right hemispheric stroke were 51.6%, while those with the left hemispheric stroke were 36.1%. The proportion of respondents with ischaemic stroke (87.1%) was higher than that of those with hemorrhagic stroke (12.3%). The prevalence of post-stroke cognitive impairment among the respondents was 41.8%. Respondents with left hemispheric stroke were more likely to have cognitive impairment than those with right cerebral stroke. Also, respondents with severe stroke-related disability were more likely to have cognitive impairment than those with mild stroke-related disability. However, respondents with a tertiary and secondary level of education were less likely to have cognitive impairment than those with a primary level of education.
Conclusion: The result of the study showed that post-stroke cognitive impairment is high among the study population. The condition is often neglected by the primary physicians managing these patients, leading to poor treatment outcomes. Efforts should be made to include cognitive assessment/ treatment in the routine care of stroke patients.
Keywords
Cognitive Impairment, Stroke, Stroke Survivors
List Of Abbreviations
NIHSS - National Institute of Health Stroke Scale
MINI - Mini-International Neuropsychiatry Inventory
MMSE - Mini-Mental State Examination
OSSS-3- Oslo Social Support Scale
MRS- Modified Rankin Scale
DSM5- Diagnostic Statistical Manual 5th Edition
VCI- Vascular Cognitive Impairment
ADL- Activities of Daily Living
SDQ- Socio Demographic Questionnaire
SPSS- Statistical Package for Social Sciences
MoCA- Monstreal Cognitive Assessment
PSCI- Post Stroke Cognitive Impairment
Chapter One
Introduction
Background
A stroke is a medical emergency that is currently defined as a sudden neurological impairment caused by a spontaneous bleeding or blockage in the central nervous system, leading to proof of tissue damage, regardless of how long the symptoms have been present [1]. The term stroke is believed to have been introduced into the medical literature only in the late seventeenth century [1]. Globally, 1 in 4 adults above 25 years will have a stroke in their lifetime. Over 110 million people around the globe have had a stroke and every minute, six Africans develop a stroke [2,3]. The recent prevalence rate of stroke in Nigeria is 1.14 per 1000, while the monthly fatality rate is as high as 40% [4]. In general, stroke is grouped into two main types, namely ischaemic and hemorrhagic [5]. Ischaemic stroke accounts for 87% of strokes, while hemorrhagic stroke accounts for 13% [5].
Stroke has been linked with mental disorders such as cognitive impairment, depression, anxiety and apathy [6]. Deficits in one or more domains of cognitive function are widespread after a stroke. Depression is the most common neuropsychiatric consequence of stroke, affecting about 33% of stroke patients [7]. Anxiety disorder is the second most common neuropsychiatric complication, with a prevalence rate of 25% [8]. Apathy without depression is linked with a loss of interest, while mania is rare in stroke patients. In addition, Out-of-proportion emotional outbursts characterize pathological affective disorder, while catastrophic reactions in stroke patients are associated with a burst of aggressive behaviors, anxiety, and crying [9,10].
Stroke is known as one of the important factors leading to cognitive impairment. It is associated with the onset of Alzheimer’s disease and vascular dementia [11]. According to DSM-5, this impairment is grouped under mild or major vascular neurocognitive disorder. Under this grouping, criterion A of neurocognitive disorder, which involves evidence of marked cognitive decline from the previous level of functioning in one or more cognitive domains, must be met based on
(1) Worry about a noticeable decrease in cognitive function expressed by an individual, an informed source, or a medical professional. (2) A significant dysfunction in cognitive functioning as recorded by standardized neuropsychological testing or another graded clinical evaluation. This is accompanied by the findings that stroke is the major, if not the exclusive, disease that is responsible for cognitive decline. Cognitive deficits in mild cognitive disorders do not affect one's capacity to carry out complex instrumental activities of everyday living, such as paying bills. However, more significant effort may be required. Cognitive deficit in major neurocognitive disorder affects one’s ability to perform everyday activities and needs help with complex instrumental activities, such as paying bills [12].Vascular cognitive dysfunction is a range that spans from mild impairment in a specific aspect to post-stroke dementia, with nearly 65% of stroke patients said to suffer from cognitive impairments and about 30% having dementia [13].
Post-stroke dementia is a clinical condition that encompasses all forms of dementia that occur after a stroke, regardless of whether it is related to vascular, neurodegenerative, or mixed causes 14. Many factors, such as stroke severity, nerve damage, history of cognitive dysfunction, and brain diseases, are associated with cognitive loss after a stroke [14].
Studies have shown that as the mortality rate from strokes decreases, there is an increase in patients with cerebral and cognitive impairment [15]. Stroke survivors now have an elevated risk of cognitive impairment. A study by Patel et al. on cognitive impairment post-stroke found that 38% of the participants experienced cognitive impairment three months following a stroke. The study identified several independent characteristics linked to cognitive impairment following a stroke, such as advanced age, ethnicity, poorer socio-economic status, left-sided stroke, visual field impairment, and incontinence from urine [16]. In a meta-analysis of 72 studies involving 21 hospital-based and eight population-based subjects, the overall rate of dementia in the first year following a first-time stroke was highly heterogeneous. The proportion of post-stroke dementia varied from 7% in population subjects to 41% in the hospital-based study. The occurrence of cognitive impairment 3 months after stroke and at one-year follow-up remained relatively stable at 22%. Risk factors identified for post-stroke cognitive impairment include older age, low socioeconomic class, patients with small vessel occlusion, and lacunar infarctions [17]. A recent systematic review of patients with PSCI showed a pooled prevalence rate of 53.4%, with mild and significant PSCI having prevalence rates of 36.4% and 16%, respectively [18].
There is a shortage of studies on cognitive impairment after stroke in Africa and Nigeria. A study by Sarfo et al. in Ghana revealed that 34% of stroke survivors in the study had vascular cognitive impairment (VCI) without dementia, while 13.6% had vascular dementia. Significant risk factors for VCI included lack of formal educational qualification, poor score on MRS, and advancing age for each 10-year increase consecutively [19]. Another study in the Benin Republic showed that about 58.3% of stroke survivors had a severe cognitive decline, and that cognitive decline was more in females(11.6%) and those with Ischaemic stroke [20]. A Nigerian study on cognitive function after stroke (COGFAST study) by Akinyemi et al. showed that among stroke patients, 8.4% were demented initially, and 39.9% had mild to moderate cognitive impairment. Factors associated with cognitive dysfunction after stroke included advanced age, poor educational status, history of cognitive decline before stroke, and atrophy of the medial temporal lobe [21]. Another study in Northern Nigeria by Aliyu et al. showed a high rate of PSCI at 67.14%, with 32.86% of cases mild, while 27.14% and 7.14% for moderate to severe PSCI [22]. A study by Fatoye et al. in southern Nigeria revealed a lower prevalence rate of 17.4%. Risk factors for cognitive deficits among the patients included paresis and low educational status [23].
Several researchers have looked at the association between depression and cognitive impairment among stroke survivors. An earlier study by Bolla-Wilson et al. looked at the link between depression and the mental domain. The study revealed that patients with depression with left hemispheric lesions did not perform well compared with non-depressed patients in four of the nine cognitive areas assessed. They made an impression that post-stroke depression seems to cause a decline in mental function owing to the laterality of the lesion [24].
Previously, studies in stroke epidemiology were more focused on mortality and recurrence, and not on long-term complications25 but currently, there is an increasing interest in the factors that could limit the quality of life and cause functional impairments among stroke survivors [25]. Studies have shown that cognitive impairment is among the strongest predictors of low quality of life among stroke patients.
Cognitive dysfunction in stroke has been linked with poor outcomes such as decreased functional recovery and increased death rate [26]. Decreased cognition has also been connected with reduced effectiveness in Activities of Daily Living(ADL) and low physical functioning at discharge [27]. About one-fifth of stroke survivors with cognitive impairment make progress, while others continue to decline [28]. Most improvement is recorded in the first three months after a stroke, although recovery may progress up to a year [29].
Statement of the Problem
Most studies on psychological complications of stroke in our environment focused on depression, anxiety, and quality of life of stroke survivors, with a shortage of studies on cognitive impairment [30,31]. Cognitive impairment is associated with poor stroke prognosis in terms of functional dependence and survival. Similarly, stroke survivors with cognitive impairment have difficulties recalling tasks, performing activities of daily living, and making sound judgments [32]. However, required attention is not given to cognitive impairment among stroke survivors [33].
Study Rationale
This study aims to justify the incorporation of mental health services into chronic care for stroke management, as the integration of psychiatric services into chronic care clinics is being considered globally [7].
Also, this study hopes to contribute to the body of evidence of the need for increased physicians' index of suspicion for cognitive impairment, as the study hopes to provide data on the extent of post-stroke cognitive impairment.
In addition, this research work looks forward to providing information on the factors associated with post-stroke cognitive impairment as there is little or no data on this in Southern Nigeria, which will help both to reduce and manage these conditions and also, this research work hopes to study the link between post-stroke cognitive impairment and depression, as they affect prognosis and are often co-morbid.
Aim
1. To determine the occurrence of post-stroke cognitive impairment among those who have suffered a stroke at the UCTH Calabar, Nigeria.
Objectives
1. To determine the prevalence rate post-stroke cognitive impairment among stroke survivors at UCTH.
2. To assess the association between post-stroke cognitive impairment and depression among stroke survivors at UCTH.
3. To determine the relationship between stroke type and cognitive impairment, among stroke survivors at the UCTH.
4. To assess the relationship between stroke severity, stroke-related disability, and social support with cognitive impairment.
Study Hypothesis
There is an association between post-stroke cognitive dysfunction and depression among stroke survivors.
Chapter Two
Methodology
Location of Study
Calabar is the capital of Cross River State and is located in southern Nigeria. It is situated between latitudes 4*55 and 5*04N of the equator and longitudes 8*18 and 8*21E of the Greenwich Meridian [34]. It covers 406 square kilometres (157 sq. mi) and has a population of 371,022 from the 2006 census. The Atlantic Ocean bounds the metropolis on the south, Odukpani L G A on the north, Akpabuyo L G A on the East, and the Calabar River on the west [35].
Administratively, it is divided into two—Municipal and South- and comprises three major tribes: Efik, Efut, and Qua. Its people are known for their rich cultural heritage, tourism, and hospitality. As a Cosmopolitan city, almost everyone understands and speaks English.
Calabar has three tertiary hospitals: the University of Calabar Teaching Hospital, the Navy Reference Hospital, and the Federal Neuropsychiatric Hospital.
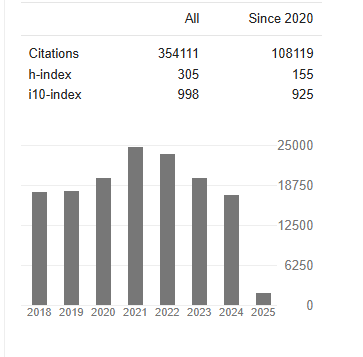
This study was done at the UCTH, established in 1979, to provide tertiary health care services [36]. The facility is a six-hundred-and- ten-bed space hospital located at Calabar in Calabar Municipality. Clinical services areavailable in all specialised medical departments, such as Surgery, Internal Medicine, Paediatrics, Orthopaedics and Trauma, Anaesthesiology, Obstetrics and Gynaecology, and Psychiatry [36]. The internal medicine department comprises Neurology, Cardiology, Nephrology, Endocrinology, Respiratory, Dermatology, and Rheumatology units [36]. This study was carried out at the Neurology clinic of the Internal Medicine department. Initially, the neurology clinic ran only on Mondays, but with the introduction of the Friday clinic, dedicated to stroke patients, it expanded its schedule. Data from the medical records in 2021 showed that the neurology clinic attended eight hundred and twelve patients, with stroke cases constituting the majority(about 609 stroke cases). With an average of 50 stroke cases per month, about 13 stroke cases per week were seen in 2021. Most of these cases were new (an average of 7 new cases per week), with others coming for follow-up visits. The stroke centre/clinic, which was commissioned in 2023, further increased the number of stroke cases seen by the neurologist (Friday clinic). Stroke patients must routinely have a CT scan report in the Neurology clinic.
Study Design
The study was a cross-sectional study.
Study Population
Participants were adult stroke survivors 18 years and above at the University of Calabar Teaching Hospital.
Inclusion Criteria
1. Brain CT-scan confirmed stroke survivors within 1 month to 5 years after stroke.
2. Patients who gave consent for the study.
Exclusion Criteria
1. Patients receiving treatment for dementia pre-stroke
2. Patients with previous history of depression.
3. Patients with severe language or physical impairment sufficiently enough to prevent assessment.
4. Those who cannot understand the English language.
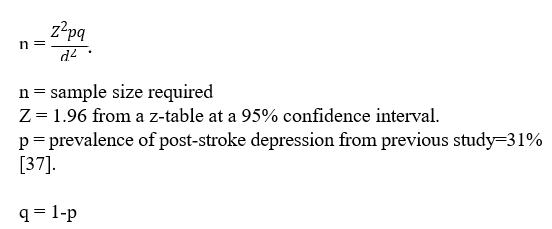
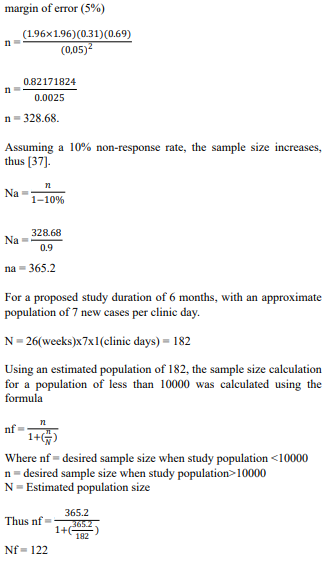
Sample Size Calculation
The study used the Cochran formula for calculating sample size for a known prevalence rate.
Sampling Technique
Those who satisfied the inclusion criteria were consecutively recruited into the study as they came for clinic visits.
Study Instruments
The Socio-Demographic/Clinical Questionnaire
The SDQ was an interviewer-administered pro forma questionnaire involving SDQ parameters like gender, marital status, tribe, denomination, employment level, educational attainment, and monthly earnings. The clinical variables, like stroke location and type, were obtained from the CT-scan report. In contrast, the number of stroke episodes and co-morbid disease conditions was obtained from the participant’s case file.
Mini International Neuropsychiatric Interview (Mini Version 7.0)
MINI was produced in 1990 by clinicians in the US and Europe for DSM-III-R and ICD-10 psychiatric disorders and is a quick, structured diagnostic interview with an administrative time of about 15 minutes [38].The MINI is an organised mental health questionnaire to assess and monitor epidemiological studies and drug experiments. Psychiatrists and health organisations use it widely in over 100 countries [39]. MINI is updated regularly and currently covers DSM-IV and DSM-5 psychiatric disorders with MINI versions 6.0 and 7.0, respectively. Its reliability score is high (kappa score more than 0.75) for major depressive disorder [39]. Compared with other diagnostic instruments, like the structured clinical interview for DSMIII, MINI does not take much time to administer [40]. It has been widely used in Nigerian studies [41,42]. The depression module of the MINI will be used in this study. The MINI have been validated for use in Nigeria [43].
Mini-Mental State Examination(MMSE)
MMSE is used to evaluate for cognitive impairment, grade the severity of cognitive impairment at any particular time, follow up fluctuations in patients' cognition, and note patients' response to treatment [44].The Mini-mental state examination is graded on a scale of 0-30, with values equals to or higher than 24 interpreted as normal cognition. A score range of 0-17 means severe cognitive impairment, while a score of 18-23 equals mild impairment. When interpreting the MMSE, consider the patient's native language, educational level, and culture, as these factors affect performance [45]. It has a sensitivity of 81% (95%CL, 78%to 84%) and specificity of 89% (95%CL, 87%to91%) [46]. It has been widely used in Nigerian studies [41,47]. It has also been validated for use in Nigeria [48].
National Institute of Health Stroke Scale (NIHSS)
The NIHSS is a tool used to measure the severity of stroke. It is typically used in clinical settings to assess and monitor the neurological status of acute stroke patients, determine appropriate care, and facilitate communication between healthcare providers. Additionally, the NIHSS can help predict both immediate and long- term outcomes for stroke survivors [49].The NIHSS comprises assessments graded on a scale, and patients can be evaluated quickly in less than 10 minutes. The grading system ranges from zero, indicating some level of dysfunction. The average total score is 42, with the lowest score being 0. The grading system is as follows: no stroke symptoms are graded at zero, mild symptoms at 1-4, and average symptoms at 5-15. Average to severe stroke symptoms at 16-20, and severe symptoms at 21-42. This tool has been used in several studies in Nigeria [41,50]. It has also been validated for use in Nigeria [51].
Modified Rankin Scale (MRS)
The MRS is a rating scale used to assess stroke patients’ functional independence level compared to their pre-stroke functions rather than evaluate their ability to perform a specific task. It is a single- item scale administered by an interviewer. Based on the following scoring, a single MRS score should be given: no symptoms 0, no significant disability despite symptoms = 1, minor dysfunction: not able to perform all previous functions but can take care of oneself without assistance = 2, average dysfunction: needs a certain level of support but can ambulate without support = 3, average-severe dysfunction: can’t ambulate and take care of oneself without support = 4, severe dysfunction: urinating on oneself, permanently bedridden with the need for regular nursing attention = 5 [50,52]. MRS has a kappa score of 0.78 [53]. It has been widely used in Nigerian studies [53,54]. It has been validated for use in Nigeria [54].
Oslo Social Support Scale (OSSS-3).
The OSSS-3 is a short questionnaire used to measure the amount of social support received [55]. It contains only three items that ask about the number of firm friends, the feeling of care from other individuals, and the association among neighbors to get feasible help. The overall scoring can be grouped into three primary levels of social support: 1) 3-8 low help, 2) 9-11 medium help, and 3) 12- 14 vital help [56]. It has a Cronbach alpha value of 0.640, and has been used in many studies in Nigeria [56,57]. It has been validated for use in Nigeria [58].
Pre-Testing
A pre-test was conducted with 10% of the sample size (12 participants) at the diabetic clinic of UCTH. The study was conducted by the researcher and two research assistants (health personnel) who were properly trained.
Ethical Consideration
Ethical clearance was obtained from the research committee of the University of Calabar Teaching Hospital. Patients were informed that their participation was voluntary and that there would be no foreseeable risk. They could withdraw their consent at any point during the study. Written informed consent was obtained from the patients. Referral for treatment was offered to those who screened positive for any domains assessed in the study.
Procedure
This study was carried out by the researcher and two research assistants. The research assistants were health personnel who were properly trained by the supervising consultants. Using the Neurology registry of the records department of UCTH, case notes of patients present for clinic each Monday and Friday were obtained. The case files of each patient were assessed to ascertain those that met the inclusion criteria. Those who met the inclusion criteria were taken into a separate clinic room, where the study was properly explained to them; thereafter, a written informed consent was obtained from the patients.
Afterwards, the patients were facilitated to see their doctors for treatment, and then the study instruments were administered. An interviewer from the research team administered the Socio- Demographic Questionnaire. The trained research assistants administered the Modified Ranking Scale Questionnaire, the NIHSS, the OSSS-3, and the MMSE. Thereafter, the researcher administered the depression module of the MINI version 7.0 Questionnaire. Codes were used to identify the questionnaires, and the case notes of participants were marked discreetly to avoid assessing twice. The filled questionnaires were collected for analysis.
An average of ten to twelve stroke patients were recruited per week, and the study lasted for 3 months.
Data Management
Completed questionnaires were entered into the Statistical Package for Social Sciences (SPSS) version 25 software. The significance level was set at a P-value less than 0.05
Chapter Three
Results
This study was a cross-sectional study done among stroke patients with 122 participants. The study aimed to assess post-stroke cognitive impairment and depression among stroke survivors at UCTH. The following results will be discussed in line with the study objectives.
|
Variable |
Frequency |
Percentage (%) |
|
Age |
|
|
|
18-34 |
5 |
4.1 |
|
35-49 |
24 |
19.7 |
|
50-64 |
49 |
40.2 |
|
65 and above Mean(±SD) 60.23±13.0 |
44 |
36.0 |
|
Gender |
|
|
|
Male |
76 |
62.3 |
|
Female |
46 |
37.7 |
|
Marital Status |
|
|
|
Married |
112 |
91.8 |
|
Single |
10 |
8.2 |
|
Ethnicity |
|
|
|
Efik |
30 |
24.6 |
|
Ibibio |
17 |
13.9 |
|
Igbo |
18 |
14.8 |
|
Yoruba |
1 |
0.8 |
|
Others |
56 |
45.9 |
|
Level Of Education |
|
|
|
Primary |
14 |
11.5 |
|
Secondary |
41 |
33.6 |
|
Tertiary |
67 |
54.9 |
|
Religion |
|
|
|
Christianity |
120 |
98.4 |
|
Islam |
1 |
0.8 |
|
Traditional |
1 |
0.8 |
|
Occupation |
|
|
|
Employed |
28 |
23.0 |
|
Self-employed |
48 |
39.3 |
|
Unemployed |
46 |
37.7 |
|
Monthly Income |
|
|
|
30000 Naira and Less |
13 |
10.7 |
|
31000 to 99000 Naira |
66 |
54.1 |
|
100000 Naira and Above |
43 |
35.2 |
|
SD-Standard deviation |
||
Table 1: Sociodemographic Characteristics of the Respondents
Sociodemographic Characteristics of the Respondents
A total of 122 patients were recruited for the study, comprising 76 males (62.3%) and 46 females (37.7%). Most respondents were married (91.8%), Christians (98.4%), and above 50 years of age (40.2%). They were mainly self-employed (39.3%) and unemployed (37.7%), with an income of thirty-one thousand naira and above (54.1%). Furthermore, more than half of the population had tertiary education (54.9%). A greater percentage of the respondents (45.9%) were from other tribes in Cross River State, with 24.6% from the Efik tribe (Table 1).
|
Variable |
Frequency |
Percentage (%) |
|
Stroke Location |
|
|
|
Right Cerebral Hemisphere |
63 |
51.6 |
|
Left Cerebral Hemisphere |
44 |
36.1 |
|
Others |
15 |
12.3 |
|
Stroke Type |
|
|
|
Hemorrhagic |
15 |
12.3 |
|
Ischemic |
107 |
87.7 |
|
Number Of Stroke Episodes |
|
|
|
1 |
104 |
85.2 |
|
2 |
15 |
12.3 |
|
3 or more |
3 |
2.5 |
|
Duration of Stroke |
|
|
|
Less than 1 Year |
95 |
77.9 |
|
1 Year To 3 Years |
15 |
12.3 |
|
More than 3 years |
12 |
9.8 |
|
Comorbidities |
|
|
|
Hypertension |
93 |
76.2 |
|
Diabetes Mellitus |
7 |
5.7 |
|
Hypertension And Diabetes |
13 |
10.7 |
|
None |
9 |
7.4 |
Table 2: Clinical Variables of the Respondents
Clinical Variables of the Respondents
The table shows the clinical variables of stroke location, stroke type, number of stroke episodes, stroke duration, and comorbidities of the respondents. Those with the right hemispheric stroke constituted more than half (51.6%) of the study population, while those with left hemispheric stroke were 36.1%. Participants with stroke lesions affecting other areas of the brain (i.e., the ‘others’ category), which include both cerebral hemispheres (3.3%), cerebellum (4.1%), basal ganglia (2.2%), brainstem (0.8%), multifocal (0.8%) and the subarachnoid space (0.8%), were less than 15%. Most of the respondents had Ischemic stroke (87.7%), with only 12.3% having hemorrhagic stroke. In addition, more respondents presented within the first year of stroke (77.9%), while the fewest were those who presented within 3 to 5 years of stroke (9.8%). Furthermore, most of the respondents were hypertensive (76.2%), with about 11% having both diabetes and hypertension. Participants with diabetes constituted about 6% of the study population.
|
Variables |
Male |
Female |
Total |
Statistics |
d |
p-value |
|
Cognitive impairment |
|
|
|
|
|
|
|
None |
41 (33.6) |
30 (24.6) |
71 (58.2) |
χ2 = 4.05 |
2 |
0.13 |
|
Mild to Moderate |
20 (16.4) |
13 (10.7) |
33 (27.0) |
|
|
|
|
Severe |
15 (12.3) |
3 (2.5) |
18 (14.8) |
|
|
|
Table 3: Prevalence of Post-Stroke Cognitive Impairment by Gender
Prevalence of Post-Stroke Cognitive Impairment in Relation to the Gender of the Respondents
The overall prevalence rate of cognitive impairment among the respondents was 41.8%. The prevalence rate of mild to moderate cognitive impairment among the respondents was 27%, while the rate of severe cognitive impairment was 14.8%. Comparing the gender distribution of cognitive impairment among the respondents, more males had both mild to moderate cognitive impairment (16.4%) and severe cognitive impairment (10.7%). The relationship between cognitive impairment and gender was not statistically significant (p = 0.13)
|
Cognitive impairment |
|||||
|
Depression |
Yes |
No |
Statistics |
df |
p-value |
|
Yes n (%) |
23(51.1%) |
22(48.9%) |
χ2 = 3.55 |
1 |
0.05 |
|
No n (%) |
26(33.8%) |
51(66.2%) |
|
|
|
Table 4: Association Between Post-Stroke Cognitive Impairment and Depression
Association Between Post-Stroke Cognitive Impairment and Depression
The table below shows the association between post-stroke cognitive impairment and depression among the study participants. The prevalence rate of depression was higher among those with cognitive impairment (51.1%) than those without cognitive impairment (48.9%). However, the association between cognitive impairment and depression was not statistically significant (p = 0.05).
|
Cognitive Impairment |
|||||
|
Variables |
Yes |
No |
Statistics |
df |
p-value |
|
Stroke Type |
|
|
|
|
|
|
Hemorrhagic |
9(18.4) |
6(8.2) |
χ2 = 2.80 |
1 |
0.09 |
|
Ischaemic |
40(81.6) |
69(9.8) |
|
|
|
|
Stroke location |
|
|
|
|
|
|
Right Hemisphere |
22(55.0) |
41(61.2) |
χ2 = 0.39 |
1 |
0.52 |
|
Left Hemisphere |
18(45.0) |
26(38.8) |
|
|
|
Table 5: Relationship between Cognitive impairment, Stroke type and location Cognitive Impairment
Relationship Between Cognitive Impairment, Stroke Type and Location
The prevalence rate of cognitive impairment among the respondents was higher in those with ischaemic (8.1.6%) hemorrhagic stroke while those with right hemispheric stroke (55%) had more cognitive impairment than those with left hemispheric stroke (45%). However, the relationship between stroke type and location with cognitive impairment was not statistically significant.
|
Cognitive Impairment |
|||||
|
Variables |
Yes |
No |
Statistics |
Df |
p-value |
|
Stroke Severity |
|
|
|
|
|
|
Mild |
22(39.3) |
34(60.7) |
|
|
|
|
Moderate |
21(35.0) |
39(65.0) |
χ2 = 9.62 |
2 |
0.01* |
|
Severe |
6(100.0) |
0(0.00 |
|
|
|
|
Stroke related disability |
|
|
|
|
|
|
Mild |
1(7.7) |
12(92.3) |
|
|
|
|
Moderate |
22(30.1) |
51(69.9) |
χ2 = 24.5 |
2 |
0.00* |
|
Severe |
26(72.2) |
10(27.8) |
|
|
|
|
Social support |
|
|
|
|
|
|
Poor |
14(41.2) |
20(58.8) |
|
|
|
|
Moderate |
15(34.1) |
29(65.9) |
χ2 = 0.97 |
2 |
0.61 |
|
Strong |
19(44.2) |
24(55.8) |
|
|
|
|
*Statistically significant |
|||||
Table 6: Relationship Between Cognitive Impairment, Stroke Severity, Stroke Related Disability and Social Support
Relationship Between Cognitive Impairment, Stroke Severity, Stroke Related Disability and Social Support
The table showed that respondents with severe stroke severity had the highest prevalence of cognitive impairment (100%) and the relationship between stroke severity and cognitive impairment was statistically significant (p = 0.01). Also, respondents with severe stroke related disability had the highest rate of cognitive impairment (72.2%) and the relationship between strike related disability with cognitive impairment was statistically significant (p = 0.00). The relationship between cognitive impairment and social support was not statistically significant(p = 0.61).
|
|
|
|
|
|
|
|
95% CI |
|
|
Variable |
B |
S E |
Wald |
df |
p-value |
Odds Ratio |
Lower |
Upper |
|
Age (Years) |
|
|
|
|
|
|
|
|
|
60 and above |
0.51 |
0.60 |
0.71 |
1 |
0.39 |
1.67 |
0.50 |
5.50 |
|
18 to 59 |
|
|
|
|
|
|
|
|
|
Gender |
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
Male |
-0.67 |
0.62 |
1.16 |
1 |
0.28 |
0.51 |
0.15 |
1.73 |
|
Stroke location |
|
|
|
|
|
|
|
|
|
Left Cerebral Hemisphere |
1.17 |
0.59 |
3.86 |
1 |
0.04* |
3.22 |
1.00 |
10.3 |
|
Right Cerebral Hemisphere |
|
|
|
|
|
|
|
|
|
Stroke Type |
|
|
|
|
|
|
|
|
|
Ischaemic |
-1.48 |
1.09 |
1.83 |
1 |
0.17 |
0.22 |
0.02 |
1.94 |
|
Hemorrhagic |
|
|
|
|
|
|
|
|
|
Depression |
|
|
|
|
|
|
|
|
|
No |
-0.51 |
0.59 |
0.76 |
1 |
0.38 |
0.59 |
0.18 |
1.90 |
|
Yes |
|
|
|
|
|
|
|
|
|
Social Support |
|
|
|
|
|
|
|
|
|
Strong |
0.30 |
0.72 |
0.17 |
1 |
0.67 |
1.35 |
0.32 |
5.62 |
|
Moderate |
1.27 |
0.81 |
2.46 |
|
0.11 |
3.58 |
0.72 |
17.5 |
|
Poor |
|
|
|
|
|
|
|
|
|
Level of Education |
|
|
|
|
|
|
|
|
|
Tertiary |
-1.47 |
0.70 |
4.40 |
1 |
0.03* |
0.22 |
0.05 |
0.90 |
|
Secondary |
-2.27 |
1.02 |
4.93 |
|
0.02* |
0.10 |
0.01 |
0.76 |
|
Primary |
|
|
|
|
|
|
|
|
|
Monthly Income (Naira) |
|
|
|
|
|
|
|
|
|
100000 and above |
-0.37 |
0.69 |
0.29 |
1 |
0.58 |
0.68 |
0.17 |
2.66 |
|
50000 and above |
-1.81 |
1.04 |
3.02 |
|
0.08 |
0.16 |
0.02 |
1.25 |
|
30000 and less |
|
|
|
|
|
|
|
|
|
Post-Stroke Duration |
|
|
|
|
|
|
|
|
|
More Than Three years |
-0.39 |
1.34 |
0.08 |
1 |
0.76 |
0.67 |
0.04 |
9.38 |
|
One To Three Years |
-0.94 |
1.12 |
0.70 |
|
0.40 |
0.38 |
0.04 |
3.53 |
|
Less than 1 year |
|
|
|
|
|
|
|
|
|
Comorbidities |
|
|
|
|
|
|
|
|
|
Hypertension And Diabetes |
0.32 |
1.57 |
0.04 |
1 |
0.83 |
1.37 |
0.06 |
30.1 |
|
Diabetes |
-0.09 |
0.86 |
0.01 |
|
0.91 |
0.90 |
0.16 |
4.91 |
|
Hypertension |
|
|
|
|
|
|
|
|
|
Stroke-Related Disability |
|
|
|
|
|
|
|
|
|
Moderately severe |
2.13 |
0.62 |
11.0 |
1 |
0.00* |
8.48 |
2.40 |
29.9 |
|
Mild |
|
|
|
|
|
|
|
|
|
Stroke Severity |
|
|
|
|
|
|
|
|
|
Moderately severe |
-0.16 |
0.82 |
0.06 |
1 |
0.79 |
0.85 |
0.25 |
2.89 |
|
Mild |
|
|
|
|
|
|
|
|
|
*Statistically Significant |
||||||||
Table 7: Binary Logistic Regression Showing the Predictors of Post-Stroke Cognitive Impairment
Binary Logistic Regression Showing the Predictors of Post- Stroke Cognitive Impairment
The table shows the result of a binary logistic regression aiming to identify the predictors of post-stroke cognitive impairment. Respondents with left hemispheric stroke were 3 times more likely to develop cognitive impairment than those with right cerebral stroke. In addition, participants with primary levels of education were more likely to develop cognitive impairment than those with secondary and tertiary levels of education. Furthermore, participants who had moderately severe stroke-related disabilities been 8 times more likely to develop cognitive impairment than those with mild disabilities. The other variables, like age, stroke type, depression, stroke duration, and social support, did not predict cognitive impairment among the respondents.
Chapter Four
Discussion
This study assessed the presence of cognitive impairment among stroke survivors at UCTH. Among the respondents, 51.6% had right hemispheric stroke, while 36.1% had left hemispheric stroke; most of the respondents had ischaemic stroke (87.7%) compared to hemorrhagic stroke (12.3%). The prevalence of post- stroke cognitive impairment was 41.8%. The study results will be discussed in harmony with the study objectives.
Prevalence of Post-Stroke Cognitive Impairment Among the Respondents
The overall prevalence of cognitive impairment among the participants was 41.8%. This finding is similar to previously reported rates of cognitive impairment, which can vary from approximately 30% to 70% depending on the follow-up time [22,59,60]. Among the respondents with cognitive impairment, 27% had mild to moderate cognitive impairment, while 14.8% had severe mental impairment. A study done by Akinyemi et al. (CogFAST) in Ibadan got a slightly higher prevalence rate of 39.9% for mild to moderate cognitive impairment [21]. Three different diagnostic instruments were used to assess cognitive function, which might have accounted for the higher prevalence rate in the study. Another study by Sarfo et al. in Ghana had a prevalence rate of 34% for vascular cognitive impairment with no dementia 19Cognitive function was assessed using the Montreal Cognitive Assessment (MOCA) and the Vascular Neuropsychological Battery, which might have accounted for the higher rate of mild to moderate cognitive impairment. The prevalence rate of 27% for mild to moderate cognitive impairment is also comparable to studies done in London (22%) and Newcastle (24%) [61,62]. The London study was prospective community-based research, and data were collected from the stroke register. This might have accounted for the lower prevalence rate. The Newcastle study is a work done by Stephen et al. on the neuropsychological characteristics of mild vascular cognitive impairment and dementia after stroke. The Cambridge Assessment of Mental Disorders in the Elderly (CAMCOG-R) was used to assess cognitive function, which might have accounted for the variation in the prevalence rate.
Participants with severe cognitive impairment were 14.8%, which is slightly higher than the rate in Ibadan (8.4%) but comparable to work done in Ghana, where 13.8% had severe cognitive impairment [19]. This is also slightly higher than the rate in Newcastle (8.6%), but within the pooled prevalence of 7% to 41.3% for severe cognitive impairment [18]. These discrepancies could be due to variations in the cognitive assessment tool used, the cut-off point for diagnosis, or sample sizes across the studies.
The predictors of cognitive impairment among the respondents include left hemispheric stroke, primary/ low level of education, and moderate to severe stroke-related disabilities. A study by Patel et al. showed that patients with left hemispheric stroke are more prone to develop cognitive impairment [16]. Similar studies done by Madureira et al. and Filler et al. showed similar associations between left hemispheric stroke and cognitive impairment [63,64]. There were no Nigerian studies that showed a similar association between left hemispheric stroke and cognitive impairment. In addition, Participants with primary or low levels of education are more predisposed to cognitive impairment. This is comparable to several studies done both locally and globally on cognitive impairment in stroke survivors [19,21,60,63]. Furthermore, respondents with moderate to severe stroke-related disabilities were associated with cognitive impairment. This is similar to studies done by Sarfo et al. and Kaddu et al [19,60]. There were no Nigerian studies that showed a similar association between stroke- related disability and cognitive impairment.
Association Between Post-Stroke Cognitive Impairment and Depression
The association between cognitive impairment and depression showed that respondents who were depressed had lower cognitive scores on the Mini-Mental State Examination (MMSE) than those who were not depressed. The association between cognitive impairment and depression was not statistically significant. Most Nigerian studies showed a statistically significant relationship between cognitive impairment and depression [23,65]. However, a study done by House et al.in the UK on the relationship between cognitive impairment and depression showed a negative correlation between scores on the MMSE and symptom levels of depression. This relationship between cognitive impairment and depression was not statistically significant [66]. Another study by Andersen et al. compared the course of cognitive impairment in depressed and non-depressed stroke patients [67]. The results showed that an improvement in intellectual performance did not accompany an improvement in mood score, therefore showing no correlation between mood symptoms and cognitive function [67]. In contrast, a study by Ojagbemi et al. showed a statistically significant relationship between cognitive dysfunction and major depression among stroke survivors [65]. This might be because the survey had a larger sample size. Similar studies done by Fatoye et al., Adewuya et al., and Nys et al also showed that cognitive impairment and depression were statistically related among stroke survivors [23,41,68]. The variations in the cut-off point for the diagnosis of cognitive impairment on the MMSE and the different instruments used for the diagnosis of depression might have accounted for the discrepancies in results across studies.
Relationship Between Cognitive Impairment and Stroke Type
Respondents with ischaemic stroke were more cognitively impaired than those with haemorrhagic stroke. However, the relationship between stroke type and cognitive impairment was not statistically significant. This is comparable to studies done in Ibadan and Uganda among stroke survivors, which showed no statistical relationship between stroke type and cognitive impairment [21,60].
Relationship Between Cognitive Impairment and Stroke Severity
Respondents with severe stroke had the highest prevalence of cognitive impairment, and the relationship between stroke severity and cognitive impairment was statistically significant (p = 0.01). This is comparable to a study by Elendu et al., which showed that stroke severity played a significant role in determining the specific cognitive deficits experienced by individuals [69]. Also, a study done by Filler et al. showed that respondents with severe stroke, evidenced by widespread white matter hyperintensities, are associated with cognitive impairment [64].
Relationship Between Cognitive Impairment and Stroke- Related Disability
Respondents with severe stroke-related disability had the highest prevalence rate of cognitive impairment, and the relationship between cognitive impairment and stroke-related disability was statistically significant (p = 0.00). A study by Sarfo et al. on the burden and predictors of post-stroke cognitive impairment shows that severe functional disability was associated with cognitive impairment [19]. Another study by Kaddumukasa et al. and Aytenew et al.showed that poor functional recovery is associated with cognitive impairment [60,70].
Relationship Between Social Support and Cognitive Impairment
The association between social support and cognitive impairment was not statistically significant; however, respondents with strong social support had the highest prevalence of cognitive impairment. A study by Li et al. on the relationship between social and psychological factors with cognitive impairment after stroke observed a significant association between the Social Support Rating Scale scores (SSRI) and PSCI [71]. However, a study by Macarra et al. on the association between social support and cognitive function in Mexican adults aged 50 and older showed that while there was an inverse relationship between cognitive impairment and social support for patients aged 71-80years, the same association was not observed for adults of other ages [72]. Patients younger than 70years did not show an association between social support and cognitive impairment, while those above 80 years, social networks were not enough to help diminish the negative impact of cognitive impairment. This shows that the relationship between social support and cognitive impairment might be related to age and not necessarily to the size of the social network. However, the study was among general adult patients in the community, which might have accounted for the variability in these results obtained. In addition, people with cognitive impairment tend to be more dependent on relatives, which may explain the reciprocal increase in social support, especially in our environment. There were no local studies on the relationship between social support and cognitive impairment among stroke patients to the best of my knowledge from my search
Limitations
1. The study design was cross-sectional, which limits the inference of causality between the associations found.
2. Using the Mini-Mental State Examination (MMSE) to assess cognitive function in respondents with different educational backgrounds might have introduced some bias into the study. Respondents with higher educational levels are more likely to complete the questionnaire than those with lower levels of education.
3. The exclusion of severe aphasic patients, an important study population, might have limited the study's generalizability.
Chapter Five
Conclusion
Conclusion
The prevalence of post-stroke cognitive impairment and depression is high among the study participants. Stroke survivors with cognitive impairment are more likely to have left hemispheric stroke, a low level of education, and moderately severe stroke- related disability. Stroke survivors with depression are more likely to have comorbid conditions such as hypertension and diabetes mellitus. Hence, the screening of stroke survivors for cognitive impairment and depression using identifiable risk factors as an integral part of their management may have potential benefits.
Recommendations
1. There should be an increased awareness and high index of suspicion among the managing physicians for the presence of cognitive impairment and depression among stroke survivors.
2. Psychological assessment and screening should be integral to stroke management to detect these conditions early.
3. Future research should consider longitudinal studies to help establish a causal relationship(s) between post-stroke cognitive impairment and depression.
4. The government should fund further research on the psychological aspect of stroke management to aid in a better understanding of the impact of these conditions on stroke survivors.
Declarations
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the research committee of the University of Calabar Teaching Hospital and the research was conducted in accordance with the ‘Helsinki’ declaration. Patients were informed that their participation was voluntary and that there would be no foreseeable risk. An informed verbal /written c, consent was obtained from the patients. Referral for treatment was offered to those who screened positive for any domains assessed in the study.
Clinical trial number not applicable.
Availability of Data and Materials
The data set used and/or analyzed during the current study are available from the corresponding Author on reasonable request.
Competing Interest
The Authors declare they have no competing interests.
Funding
There is no funding for this research.
Authors Contribution
IO- Conceptualized the research, carried out recruitment of study participants and was involved in the analysis of the results.
PN- Involved in the recruitment process and writing of the literature review.
UU- Involved in supervising and analyzing data.
EE-Involved in supervising and analysis of data
EU-Involved in supervising and analysis of data.
All authors read and approved the final manuscript
Acknowledgement
None
References
- Theofanidis, D. (2014). From apoplexy to brain attack, a historical perspective on stroke to date. J Nurs Care, 4, e121.
- Feigin, V. L., Brainin, M., Norrving, B., Martins, S., Sacco, R. L., Hacke, W., ... & Lindsay, P. (2022). World Stroke Organization (WSO): global stroke fact sheet 2022. International journal of stroke, 17(1), 18-29.
- Akinyemi, R. O., Ovbiagele, B., Adeniji, O. A., Sarfo, F. S., Abd-Allah, F., Adoukonou, T., ... & Owolabi, M. O. (2021). Stroke in Africa: profile, progress, prospects and priorities. Nature Reviews Neurology, 17(10), 634-656.
- Wahab, K. W. (2008). The burden of stroke in Nigeria. International journal of stroke, 3(4), 290-292.
- Hachinski, V., Iadecola, C., Petersen, R. C., Breteler, M. M., Nyenhuis, D. L., Black, S. E., ... & Leblanc, G. G. (2006). National Institute of Neurological Disorders and Stroke– Canadian stroke network vascular cognitive impairment harmonization standards. Stroke, 37(9), 2220-2241.
- Robinson, MD, R. G. (1997). Neuropsychiatric consequences of stroke. Annual review of medicine, 48(1), 217-229.
- Gyagenda, J. O., Ddumba, E., Odokonyero, R., Kaddumukasa, M., Sajatovic, M., Smyth, K., & Katabira, E. (2015). Post- stroke depression among stroke survivors attending two hospitals in Kampala Uganda. African Health Sciences, 15(4), 1220-1231.
- Robinson, R. G. (2006). The clinical neuropsychiatry of stroke: Cognitive, behavioral and emotional disorders following vascular brain injury. Cambridge University Press.
- Nemani, K., & Gurin, L. (2021, February). Neuropsychiatric complications after stroke. In Seminars in neurology (Vol. 41, No. 01, pp. 085-100). Thieme Medical Publishers, Inc..
- Chemerinski, E., & Robinson, R. G. (2000). The neuropsychiatry of stroke. Psychosomatics: Journal of Consultation and Liaison Psychiatry, 41(1), 5-14.
- Lo Coco, D., Lopez, G., & Corrao, S. (2016). Cognitive impairment and stroke in elderly patients. Vascular health and risk management, 105-116.
- Ayres, J. L. (2015). Diagnostic and Statistical Manual Of Mental Disordes, Fifth Edition.
- Cullen, B., O’Neill, B., Evans, J. J., Coen, R. F., & Lawlor,B. A. (2007). A review of screening tests for cognitive impairment. Journal of Neurology, Neurosurgery & Psychiatry, 78(8), 790-799.
- Bevan, S., Traylor, M., Adib-Samii, P., Malik, R., Paul, N. L., Jackson, C., ... & Markus, H. S. (2012). Genetic heritability of ischemic stroke and the contribution of previously reported candidate gene and genomewide associations. Stroke, 43(12), 3161-3167.
- Allan, L. M., Rowan, E. N., Firbank, M. J., Thomas, A. J., Parry,S. W., Polvikoski, T. M., ... & Kalaria, R. N. (2011). Long term incidence of dementia, predictors of mortality and pathological diagnosis in older stroke survivors. Brain, 134(12), 3716- 3727.
- Patel, M. D., Coshall, C., Rudd, A. G., & Wolfe, C. D. (2002). Cognitive impairment after stroke: clinical determinants and its associations with longâ?term stroke outcomes. Journal of the American Geriatrics Society, 50(4), 700-706.
- Pendlebury, S. T., & Rothwell, P. M. (2009). Prevalence, incidence, and factors associated with pre-stroke and post- stroke dementia: a systematic review and meta-analysis. The Lancet Neurology, 8(11), 1006-1018.
- Sun, J. H., Tan, L., & Yu, J. T. (2014). Post-stroke cognitive impairment: epidemiology, mechanisms and management. Annals of translational medicine, 2(8), 80.
- Sarfo, F. S., Akassi, J., Adamu, S., Obese, V., & Ovbiagele,B. (2017). Burden and predictors of poststroke cognitive impairment in a sample of Ghanaian stroke survivors. Journal of Stroke and Cerebrovascular Diseases, 26(11), 2553-2562.
- Gnonlonfoun, D. D., Ossou-Nguiet, P. M., Diallo, L. L., Adjien, C., Avlessi, I., Goudjinou, G., ... & Avode, G. D. (2014). Post-Stroke Cognitive Disorders and Associated Factors in French Speaking West Africa, Benin Case. Neuroscience & Medicine, 2014.
- Akinyemi, R. O., Allan, L., Owolabi, M. O., Akinyemi, J. O., Ogbole, G., Ajani, A., ... & Kalaria, R. N. (2014). Profile and determinants of vascular cognitive impairment in African stroke survivors: the CogFAST Nigeria Study. Journal of the neurological sciences, 346(1-2), 241-249.
- Abba, M. A., & Usman, M. Y. (2020). Prevalence and pattern of post-stroke cognitive impairment in Kano, Nigeria. Archives of Physiotherapy and Global Researches, 24(1), 7-11.
- Fatoye, F. O., Komolafe, M. A., Eegunranti, B. A., Adewuya,O., Mosaku, S. K., & Fatoye, G. K. (2007). Cognitive impairment and quality of life among stroke survivors in Nigeria. Psychological reports, 100(3), 876-882.
- Bolla-Wilson, K., Robinson, R. G., Starkstein, S. E., Boston, J., & Price, T. R. (1989). Lateralization of dementia of depression in stroke patients. The American journal of psychiatry, 146(5), 627-634.
- Chaturvedi, P., Tiwari, V., Singh, A. K., Qavi, A., & Thacker,K. (2020). Depression impedes neuroplasticity and quality of life after stroke. Journal of Family Medicine and Primary Care, 9(8), 4039-4044.
- Tatemichi, T. K., Desmond, D. W., Stern, Y., Paik, M., Sano, M., & Bagiella, E. (1994). Cognitive impairment after stroke: frequency, patterns, and relationship to functional abilities. Journal of Neurology, Neurosurgery & Psychiatry, 57(2), 202-207.
- Paker, N., BuÄ?daycı, D., TekdöÅ?, D., Kaya, B., & Dere, C. (2010). Impact of cognitive impairment on functional outcome in stroke. Stroke Res Treat.
- Al-Qazzaz, N. K., Ali, S. H., Ahmad, S. A., Islam, S., & Mohamad, K. (2014). Cognitive impairment and memory dysfunction after a stroke diagnosis: a post-stroke memory assessment. Neuropsychiatric disease and treatment, 1677- 1691.
- Cumming, T. B., Marshall, R. S., & Lazar, R. M. (2013). Stroke, cognitive deficits, and rehabilitation: still an incomplete picture. International Journal of stroke, 8(1), 38-45.
- Khedr, E. M., Abdelrahman, A. A., Desoky, T., Zaki, A. F., & Gamea, A. (2020). Post-stroke depression: frequency, risk factors, and impact on quality of life among 103 strokepatients—hospital-based study. The Egyptian Journal ofNeurology, Psychiatry and Neurosurgery, 56(1), 66.
- Uwayezu, M. G., Gishoma, D., Sego, R., Mukeshimana, M., & Collins, A. (2019). Anxiety and depression among cancer patients: prevalence and associated factors at a Rwandan referral hospital. Rwanda Journal of Medicine and Health Sciences, 2(2), 118-125.
- Levine, D. A., Wadley, V. G., Langa, K. M., Unverzagt, F. W., Kabeto, M. U., Giordani, B., ... & Galecki, A. T. (2018). Risk factors for poststroke cognitive decline: the REGARDS study (reasons for geographic and racial differences in stroke). Stroke, 49(4), 987-994.
- Melkas, S., Jokinen, H., Hietanen, M., & Erkinjuntti, T. (2014). Poststroke cognitive impairment and dementia: prevalence, diagnosis, and treatment. Degenerative neurological and neuromuscular disease, 21-27.
- Ele, I. E., & Nkang, M. O. (2014). Structure and efficiency of crayfish marketing in major markets in Calabar, Cross River State, Nigeria. Journal of Business and Management, 16(4), 26-32.
- Eko Jimmy, E., Kalu, O., & Osuchukwu Nelson, C. (2013). Prevalence of contraceptive use among women of reproductive age in Calabar Metropolis, Southern Nigeria. Int J Humanit Soc Sci Invent, 2, 27-34.
- Mkpanam ne. Comparison of knowledge, attitude and utilization of the national health insurance by workers in the teaching and general hospitals in calabar. Public Health. Published online in 2012.
- Ojagbemi, A., Akpa, O., Elugbadebo, F., Owolabi, M., & Ovbiagele, B. (2017). Depression after Stroke in Subâ?Saharan Africa: A Systematic Review and Metaâ?Analysis. Behavioural neurology, 2017(1), 4160259.
- Pinninti, N. R., Madison, H., Musser, E., & Rissmiller, D. (2003). MINI International Neuropsychiatric Schedule: clinical utility and patient acceptance. European psychiatry, 18(7), 361-364.
- Black, D. W., Arndt, S., Hale, N., & Rogerson, R. (2004). Use of the Mini International Neuropsychiatric Interview (MINI) as a screening tool in prisons: results of a preliminary study. Journal of the American Academy of Psychiatry and the Law Online, 32(2), 158-162.
- Mordal, J., Gundersen, Ø., & Bramness, J. G. (2010). Norwegian version of the Mini-International Neuropsychiatric Interview: feasibility, acceptability and test-retest reliability in an acute psychiatric ward. European Psychiatry, 25(3), 172- 177.
- Olibamoyo, O., Coker, O., Ola, B., Adewuya, A., & Atilola, O. (2019). Prevalence and correlates of depression among Nigerian stroke survivors. South African journal of psychiatry, 25(1), 1-7.
- Popoola, A. O., & Adewuya, A. O. (2012). Prevalence and correlates of depressive disorders in outpatients with breast cancer in Lagos, Nigeria. Psychoâ?Oncology, 21(6), 675-679.
- Opakunle, T., Aloba, O., Nwozo, C., Adesanya, D. D., & Adebimpe, O. (2023). Psychometric adaptation of the hospital anxiety and depression scale as a self-rated suicide risk assessment instrument among Nigerian surgical patients. International Journal of Medicine and Health Development, 28(4), 330-336.
- Huang, Y. P., Singh, A., Chen, S., Sun, F. J., Huang, C. R., & Liu, S. I. (2019). Validity of a novel touch screen tablet-based assessment for mild cognitive impairment and probable AD in older adults. Assessment, 26(8), 1540-1553.
- Galea, M., & Woodward, M. (2005). Mini-mental state examination (MMSE). Australian Journal of Physiotherapy, 51(3), 198.
- Fan, T., & Rossi, C. (2015). Screening for cognitive impairment in older adults. American Family Physician, 92(2), 125-126.
- Baiyewu, O., Smith-Gamble, V., Akinbiyi, A., Lane, K. A., Hall, K. S., Ogunniyi, A., ... & Hendrie, H. C. (2003). Behavioral and caregiver reaction of dementia as measured by the neuropsychiatric inventory in Nigerian community residents. International Psychogeriatrics, 15(4), 399-409.
- Adebusoye, L. A., Arinola, G., Amaefula, G., Hunter, S., Jenkins, H., & Pitt, V. (2021). Comparison of the Rowland University dementia assessment scale and mini-mental state examination cognitive screening tools among older people in Nigeria.
- Brott, T., Adams Jr, H. P., Olinger, C. P., Marler, J. R., Barsan,W. G., Biller, J., ... & Hertzberg, V. (1989). Measurements of acute cerebral infarction: a clinical examination scale. Stroke, 20(7), 864-870.
- Ekeh, B., Ogunniyi, A., Isamade, E., & Ekrikpo, U. (2015). Stroke mortality and its predictors in a Nigerian teaching hospital. African health sciences, 15(1), 74-80.
- Dawodu, C. O., & Olaniyan, K. A. (2012). The Predictive Value of the National Institute of Health Stroke Scale (NIHSS) For Haemmorhagic Stroke Patients in a Non–Interventional Study. Online Journal of Medicine and Medical Science Research, 1(3), 42-48.
- De Haan, R., Limburg, M., Bossuyt, P., Van der Meulen, J., & Aaronson, N. (1995). The clinical meaning of Rankin ‘handicap’grades after stroke. Stroke, 26(11), 2027-2030.
- Wilson, J. L., Hareendran, A., Hendry, A., Potter, J., Bone, I., & Muir, K. W. (2005). Reliability of the modified Rankin Scale across multiple raters: benefits of a structured interview. Stroke, 36(4), 777-781.
- Owolabi, M. O., & Ogunniyi, A. (2009). Profile of healthâ? related quality of life in Nigerian stroke survivors. European Journal of Neurology, 16(1), 54-62.
- Van Lente, E., Barry, M. M., Molcho, M., Morgan, K., Watson, D., Harrington, J., & McGee, H. (2012). Measuring population mental health and social well-being. International journal of public health, 57(2), 421-430.
- Nosikov, A., & Gudex, C. (2003). Development of a common instrument for. EUROHIS: Developing common instruments for health surveys, 57, 121.
- Kocalevent, R. D., Berg, L., Beutel, M. E., Hinz, A., Zenger, M., Härter, M., ... & Brähler, E. (2018). Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC psychology, 6(1), 31.
- Abiola, T., Udofia, O., & Zakari, M. J. M. J. P. (2013).Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malaysian journal of psychiatry, 22(2), 32-41.
- Patel, M., Coshall, C., Rudd, A. G., & Wolfe, C. D. (2003). Natural history of cognitive impairment after stroke and factors associated with its recovery. Clinical rehabilitation, 17(2), 158-166.
- Kaddumukasa, M. N., Kaddumukasa, M., Katabira, E., Sewankambo, N., Namujju, L. D., & Goldstein, L. B. (2023). Prevalence and predictors of post-stroke cognitive impairment among stroke survivors in Uganda. BMC neurology, 23(1), 166.
- Douiri, A., Rudd, A. G., & Wolfe, C. D. (2013). Prevalence of poststroke cognitive impairment: South London stroke register 1995–2010. Stroke, 44(1), 138-145.
- Stephens, S., Kenny, R. A., Rowan, E., Allan, L., Kalaria, R. N., Bradbury, M., & Ballard, C. G. (2004). Neuropsychological characteristics of mild vascular cognitive impairment and dementia after stroke. International journal of geriatric psychiatry, 19(11), 1053-1057.
- Madureira, S., Guerreiro, M., & Ferro, J. M. (2001). Dementia and cognitive impairment three months after stroke. European journal of neurology, 8(6), 621-627.
- Filler, J., Georgakis, M. K., & Dichgans, M. (2024). Risk factors for cognitive impairment and dementia after stroke: a systematic review and meta-analysis. The Lancet Healthy Longevity, 5(1), e31-e44.
- Ojagbemi, A., Akinyemi, R., & Baiyewu, O. (2014). Cognitive dysfunction and functional limitations are associated with major depression in stroke survivors attending rehabilitation in Nigeria. NeuroRehabilitation, 34(3), 455-461.
- House, A., Dennis, M., Warlow, C., Hawton, K., & Molyneux,(1990). The relationship between intellectual impairment and mood disorder in the first year after stroke. Psychological medicine, 20(4), 805-814.
- Andersen, G., Vestergaard, K., Riis, J. Ø., & Ingemanâ?Nielsen,M. (1996). Dementia of depression or depression of dementia in stroke?. Acta Psychiatrica Scandinavica, 94(4), 272-278.
- Nys, G. M. S., Van Zandvoort, M. J. E., Van der Worp, H. B., De Haan, E. H. F., De Kort, P. L. M., & Kappelle, L. J. (2005). Early depressive symptoms after stroke: neuropsychological correlates and lesion characteristics. Journal of the neurological sciences, 228(1), 27-33.
- Elendu, C., Amaechi, D. C., Elendu, T. C., Ibhiedu, J. O.,Egbunu, E. O., Ndam, A. R., ... & Temilade, A. V. (2023). Stroke and cognitive impairment: understanding the connection and managing symptoms. Annals of Medicine and Surgery, 85(12), 6057-6066.
- Aytenew, T. M., Kefale, D., Birhane, B. M., Kebede, S. D., Asferie, W. N., Kassaw, A., ... & Asnakew, S. (2024). Poststroke cognitive impairment among stroke survivors in Sub-Saharan Africa: a systematic review and meta-analysis. BMC Public Health, 24(1), 2143.
- Li, Y., Tang, A., Ge, L., Zhang, L., Chen, L., Xu, Y., ... & Wu,Q. (2024). The relationship between social and psychological factors with cognitive impairment after stroke: a prospectivestudy. Frontiers in Psychiatry, 15, 1403027.
- Zamora-Macorra, M., de Castro, E. F. A., Ávila-Funes, J. A., Manrique-Espinoza, B. S., López-Ridaura, R., Sosa-Ortiz, A. L., ... & Del Campo, D. S. M. (2017). The association between social support and cognitive function in Mexican adults aged 50 and older. Archives of Gerontology and Geriatrics, 68, 113-118.