
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2016) Volume 1, Issue 1
Clinical Screening Strategies for Cervical Cancer, Chlamydia trachomatis Infection, and Bacterial Vaginosis in Pregnant Women in Hokkaido between 2004 and 2012: A Retrospective Study
2Department of Obstetrics and Gynecology, JCHO Hokkaido Hospital, Sapporo, Hokkaido, Japan
3Department of Public Health, Sapporo Medical University School of Medicine, Sapporo, Hokkaido, Japan
4Department of Obstetrics and Gynecology, Kushiro Red Cross Hospital, Kushiro, Hokkaido, Japan
5Department of Obstetrics and Gynecology, Kitami Red Cross Hospital, Kitami, Hokkaido, Japan
6Department of Obstetrics and Gynecology, Hokkaido University Graduate School of Medicine, Sapporo, H, Japan
Received Date: Sep 09, 2016 / Accepted Date: Sep 18, 2016 / Published Date: Sep 22, 2016
Copyright: ©Shimono S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: We previously conducted an anonymous survey on universal screening for uterine cervical cancer (UCC), genital Chlamydia trachomatis (CT), and bacterial vaginosis (BV) among pregnant women in Hokkaido (Japan) in 2004, and the screening rates were 87.5% (49/56), 87.5% (40/56), and 57.1% (32/56), respectively. According to the Japanese guidelines for obstetric practice published in 2008 and revised in 2011, universal screening for UCC and genital CT is recommended, but not for all asymptomatic BV patients. We investigated how the screening rates changed from 2004 to 2012.
Methods: The number of obstetric care facilities in Hokkaido was 113 in 2004 and 97 in 2012. We conducted an anonymous survey on universal screening for UCC, genital CT, and BV and compared the results of the 2004 and 2012 surveys. Our questionnaires in 2004 and 2012 were similar with the exception of the questions about timing of genital CT and BV screenings and diagnostic methods for BV in 2012.
Results: Survey response rates in 2004 and 2012 were 49.6% (56/113) and 72.9% (70/96), respectively. There were 44,020 deliveries in 2004 and 38,686 in 2012. In 2012, a total of 98.7% (69/70), 100% (70/70), and 67.1% (47/70) of facilities participated in universal screening for UCC, genital CT, and BV, respectively. Compared to 2004, screening rates significantly increased for UCC and genital CT, but did not show a significant difference for BV. However, the number of patients who participated in the screening test for BV significantly increased from 60.1% in 2004 to 75.4% in 2012 (P < 0.001).
Conclusions: Universal screening for UCC and genital CT followed the guidelines, but not for BV, which showed an increase when compared to the survey in 2004. Obstetricians in Hokkaido are now starting to consider the importance of BV screening and treatment in early pregnancy.
Keywords
Bacterial vaginosis, Chlamydia trachomatis, Uterine cervical cancer, Prenatal test, Screening test.
Abbreviations
UCC: uterine cervical cancer; CT: genital Chlamydia trachomatis; BV: bacterial vaginosis; GW: gestational weeks; JMHLW: Japanese Ministry of Health, Labor, and Welfare
Introduction
In common clinical practice, Japanese physicians screen pregnant women for uterine cervical cancer (UCC) and genital Chlamydia trachomatis (CT) [1]. In our previous study [1], more than 85% of the obstetric facilities that responded to the questionnaire employed a policy of universal screening for UCC and genital CT in 2004 in Hokkaido [1], the northernmost and second largest island in Japan with an approximate population of 5,500,000 and 40,000 births per year at and after gestational week (GW) 22.
Bacterial vaginosis (BV), characterized by complex bacterial flora dominated by diverse anaerobes, affects approximately 20% of Japanese women [2]. BV is associated with several adverse reproductive and health outcomes, including elevated risks of sexually transmitted diseases, transmission of HIV to male sex partners, pelvic inflammatory disease, cervicitis, and preterm delivery [3-7]. However, it is unclear whether a policy of universal screening for BV in all pregnant women would be helpful in avoiding preterm delivery. Therefore, currently universal screening for BV is not recommended in asymptomatic pregnant women worldwide [8-10]. Since the detection and treatment of BV at an early stage of the pregnancy may reduce the risk of preterm birth [11-13], the analysis of vaginal bacterial flora of pregnant women was relatively common in Hokkaido in 2004 [1]; Indeed, 57.1% of obstetric facilities in Hokkaido adopted a policy of universal screening for BV in 2004 [1].
Japanese guidelines for obstetric practice were published for the first time in 2008 and revised in 2011 [9]. Since these guidelines recommended screening strategies for UCC and genital CT, but not for asymptomatic BV patients, we expected improvements in the rates of these screening, no reports have been published yet.
We conducted a questionnaire survey to determine the rate of UCC, genital CT, and BV screenings among pregnant women in Hokkaido in 2012, and we compared the results of this study with those of our previous study performed in 2004 [1].
Materials and Methods
This study was conducted for the Hokkaido Study of Bacterial Vaginosis and approved by the institutional review board of Hokkaido University Hospital. In total 96 and 113 obstetric facilities provided maternity services, including antenatal care and childbirth, in Hokkaido in 2012 and 2004, respectively [1]. An anonymous questionnaire was sent to all 96 facilities in February 2013 regarding strategies employed for UCC, genital CT, and BV screening in 2012 (Table 1). The questionnaire form in Table 1 was similar to the one used in the previous study conducted in January 2005 [1]. The questionnaire used in 2005 did not include questions about the timing of the screenings for CT and BV and about diagnostic methods for BV. The diagnostic methods of BV were Nugent score, Amsel’s criteria, aerobic culture, or combined aerobic and anaerobic cultures [14,15].
|
Please provide information regarding your screening policies for uterine cervical cancer (UCC), genital Chlamydia trachomatis (CT), and bacterial vaginosis (BV) in 2012. Please tick one box in each of the following lists. |
|
|
|
3. Pregnancy stage when the screening test for genital CT was performed
|
|
|
5. Pregnancy stage when the screening test for genital BV was performed
|
|
|
7. How many women gave birth at GW ≥ 22 at your facility in 2012? Please provide number of women in the following parenthesis.
|
Table 1: Questionnaires given to the 96 obstetric facilities in Hokkaido.
Statistical analyses were performed using the SAS software package (version 9.3). The difference in the collection of questionnaires between 2004 and 2012 was analyzed using X2 tests, with a significance level set at P < 0.05
Results
Response rate of the questionnaire and data size
Seventy (72.9%) of the 96 facilities responded and completed the questionnaire form; this rate was significantly higher than in 2004 (49.6%, 56/113, P = 0.001) [1]. In 2012, a total of 28,956 deliveries were conducted at the 70 hospitals, ranging from 17 to 1,353 deliveries per hospital (mean, 413.6). The delivery numbers 1-199, 200 -399, 400-599, 600-799, 800-999, 1000-1199 and 1200-1399 were performed at 15, 23, 16, 11, 1, 2, and 2 hospitals, respectively. In 2004, 24,050 deliveries were conducted at 56 hospitals, ranging from 75 to 1,530 deliveries per hospital (mean, 429.5) [1]. Hokkaido had 38,686 and 44,020 neonates born at GW ≥ 22 in 2012 and 2004, respectively [16]. Although some of them were twins or triplets, we assumed that the number of neonates was equal to the number of pregnancies in 2004 and 2012.
Frequency of administration of the three screening tests
The universal screening policy for UCC was adopted in 98.6% (69/70) of the facilities in 2012, compared to the rate of 87.5% (49/56) in 2004 (P = 0.0141) (Table 2) (Figure 1). All facilities (70/70) performed CT testing in 2012, whereas in 2004 87.5% (49/56) of facilities performed this testing (P = 0.0027) (Table 2) (Figure 1). Screening tests for genital CT were performed in women at GW ≤ 12 and GW < 16 in 72.9% (51/70) and 94.3% (66/70) of facilities in 2012, respectively.
|
Details |
Hospitals |
Cases |
||||||
|
2004 |
2012 |
2004 |
2012 |
|||||
|
Number |
% |
Number |
% |
Number |
% |
Number |
% |
|
|
Screening tests for Cervical cancer |
|
|
|
|
|
|
|
|
|
Universal screening |
49 |
87.5% |
69 |
98.6% |
22187 |
92.3% |
28666 |
99.0% |
|
Women at high risk |
3 |
5.4% |
1 |
1.4% |
725 |
3.0% |
290 |
1.0% |
|
No tests performed |
4 |
7.1% |
0 |
0.0% |
1138 |
4.7% |
0 |
0.0% |
|
Total |
56 |
100.0% |
70 |
100.0% |
24050 |
100.0% |
28956 |
100.0% |
|
Chlamydia trachomatis |
|
|
|
|
|
|
|
|
|
Universal screening |
49 |
87.5% |
70 |
100.0% |
21541 |
89.6% |
28956 |
100.0% |
|
Women at high risk |
7 |
12.5% |
0 |
0.0% |
2509 |
10.4% |
0 |
0.0% |
|
No tests performed |
0 |
0.0% |
0 |
0.0% |
0 |
0.0% |
0 |
0.0% |
|
Total |
56 |
100.0% |
70 |
100.0% |
24050 |
100.0% |
28956 |
100.0% |
|
Bacterial vaginosis |
|
|
|
|
|
|
|
|
|
Universal screening |
32 |
57.1% |
47 |
67.1% |
14596 |
60.7% |
21847 |
75.4% |
|
Women at high risk |
20 |
35.7% |
15 |
21.4% |
7943 |
33.0% |
4692 |
16.2% |
|
No tests performed |
4 |
7.1% |
8 |
11.4% |
1511 |
6.3% |
2417 |
8.3% |
|
Total |
56 |
100.0% |
70 |
100.0% |
24050 |
100.0% |
28956 |
100.0% |
Table 2: Frequency of gynecological screening tests in pregnant women
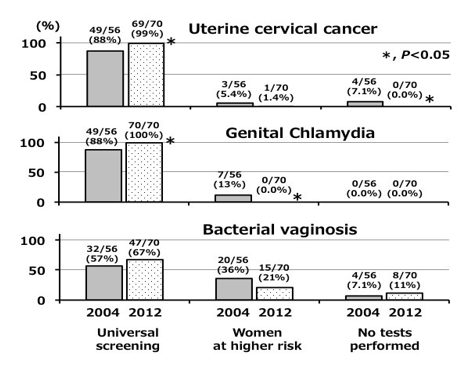
Figure 1: The percentage of facilities with different screening strategies for UCC, genital CT, and BV. The gray bars represent 2004 and the dot bar represent 2012. The three categories are (i) universal screening, (ii) women at high risk, and (iii) no test performed. The universal screenig rate for UCC and genital CT significantly increased between the two periods, but not significantly for BV.
The universal screening policy for BV was adopted in 67.1% (47/70) of the facilities in 2012 and in 57.1% (32/56) of the facilities in 2004 (P = 0.1665) (Table 2) (Figure 1). The number of pregnant women screened for BV significantly increased from 60.1% (14,596/24,050) in 2004 to 75.4% (21,847/28,956) in 2012 (P < 0.001) (Figure 2).
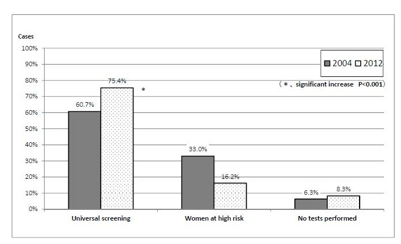
Figure 2: The percentage of cases for BV screening strategies in 2004 and in 2012. The gray bars represent 2004 and dot bars represent 2012. The three categories are (i) universal screening, (ii) women at high risk, and (iii) no test performed. The rate of universal screening for BV significantly increased from 60.7% (14,596/24,050) to 75.4% (21,847/28,956) (P < 0.001).
In 2012, BV was screened at GW < 20 in 28 (59.6%) of the 47 facilities with a universal screening policy. There were 15,182 childbirths in 28 facilities. For the detection of BV, aerobic cultures alone were used in 11 facilities with 5,341 childbirths, and methods other than aerobic culture alone were used in 17 of the 28 facilities, with BV screening at GW < 20. These 17 facilities had 9,841 childbirths, and at least 45.0% (9,841/21,847) of all pregnant women in Hokkaido underwent BV screening at GW < 20; the test was performed using either Nugent score based on Gram staining (7,944 women in 12 facilities), Amsel’s criteria (412 women in one facility), or combined aerobic and anaerobic cultures (1,485 women in 4 facilities). The number of pregnant women having the universal screening at inadequate period GW![]() 20 was 6,665 in 19 facilities
20 was 6,665 in 19 facilities
Discussion
In these three screening tests, since we cannot correctly diagnose UCC, genital CT and BV by visual inspection, universal screening tests need to be conducted. In this paper, we analyzed universal screening for UCC, genital CT, and BV in Hokkaido. The 99% (69/70) of the facilities that participated in this study adopted a policy of universal screening for UCC. More than 99% of Japanese women visit their physician for antenatal care during the early stages of pregnancy [17]. Screening cytology with Papanicolaou smear is effective in the reduction of mortality due to UCC [18]. The Japanese Ministry of Health, Labor, and Welfare (JMHLW) stated in 2010 that “performance of screening test for UCC in an early stage of pregnancy is standard care.” The results of the present study suggest that Japanese physicians followed the guideline of the JMHLW statement. Since there are more than one million maternities in Japan every year, the universal screening policy adopted in 98.6% of the facilities may have contributed to the reduction of mortality from UCC: the rate of class III or higher cytology in pregnant women was1.1% (321/28,616) in Japan (data from 1993 to 2002) [19].
All of the 70 facilities that participated in this study reported a policy of universal screening for genital CT, whereas in 2004 only 87.5% of the facilities did. This marked increase may have been due to the revised Japanese guidelines for obstetric practice published in 2011 [9]. Genital CT results in vertical transmission of CT to neonates [20] and the JMHLW announced in December 2010 the screening for genital CT as part of standard care for pregnant women with the cost of the test financially supported by the Japanese government. As the result, the 2011 guidelines [9] recommended universal screening for genital CT until GW 30. However, the screening for CT was conducted in the first trimester in 94 % of the facilities.
The number of facilities that adopted the universal screening for BV increased between 2004 and 2012, but not significantly. However, the number of the cases undergoing universal screening for BV significantly increased between the two periods.
Among 21,847 women screened for BV in 2012, 55.0% underwent BV screening at and after GW 20, or with aerobic culture alone. In a review on BV and pregnancy outcomes by McDonald et al. a low preterm birth rate was associated with BV treatment before GW 20 [12]. Aerobic culture of the vaginal flora alone is not suitable for diagnosis of BV [21]. In our previous study, the frequency of emergent cervical cerclage was lower in facilities with BV screening, suggesting that treatment of BV was effective to avoid mid-gestation labor consistent with the results of a recent study by Sangkomkamhang et al. and Farr et al. [1,13,22]. Among pregnant women, the main problem associated with BV is a risk of preterm birth [11]. Therefore, BV screening at GW < 20 with either Nugent score based on Gram staining, Amsel’s criteria, or combined aerobic and anaerobic cultures was considered adequate [14,15]. In Hokkaido, obstetricians think that the universal screening for BV is important for preventing preterm birth, because they recognize the risk of the ascending intrauterine infection to the fetus [23]. Although the number of pregnant women screened for BV has gradually increased, half of the women who underwent BV screening in Hokkaido were inadequately screened in 2012. It is important to advise the facilities to conduct the screening at GW < 20 using the Nugent score.
We are concerned about the change in preterm birth rate between 2004 and 2012 in Hokkaido. Since the JMHLW does not publish the number of preterm births including the GW in various prefectures of Japan, we don’t know the change in preterm birth rate in Hokkaido. In the future, we would like the JMHLW to let us know the number of preterm births including the GW in the different prefectures for a thorough study.
Conclusion
Universal screening test for UCC and genital CT was conducted in Hokkaido in 2012 as stated by the Japanese guidelines for obstetric practice. On the other hand, universal screening for BV was gradually adopted in clinical practice against the guidelines. Obstetricians in Hokkaido seem to consider BV screening and treatment during pregnancy very important.
Acknowledgements
We are grateful to Dr. Kiyoshi Choji from the Nakashibetsu Municipal Hospital and Dr. Hiroshige Mikamo from the Aichi Medical University Hospital for their thoughtful suggestions.
References
- Shimano S, Kawamura M, Sonoda T, Minakami H (2009) Possible association between screening BV at the prenatal visit and reduced cervical cerclage: Multi-center questionnaire in Hokkaido, Japan. J Obstet Gynaecol Res 35: 262-270.
- Shimano S, Nishikawa A, Sonoda T, Kudo R (2004) Analysis of the prevalence of bacterial vaginosis and Chlamydia trachomatis infection in 6083 pregnant women at a hospital in Otaru, Japan. J Obstet Gynaecol Res 30: 230-236.
- Schwebke JR, Desmond R (2005) Risk factors for bacterial vaginosis in women at high risk for sexually transmitted diseases. Sex Transm Dis 32: 654-658.
- Cohen CR, Lingappa JR, Baeten JM, Ngayo MO, Spiegel CA, et al. (2012) Bacterial vaginosis associated with increased risk of female-to-male HIV-1 transmission: a prospective cohort analysis among African couples. PLoS Med 9: e1001251.
- Haggerty CL, Hillier SL, Bass DC, Ness RB; PID Evaluation and Clinical Health study investigators (2004) Bacterial vaginosis and anaerobic bacteria are associated with endometritis. Clin Infect Dis 39: 990-995.
- Marrazzo JM, Wiesenfeld HC, Murray PJ, Busse B, Meyn L, et al. (2006) Risk factors for cervicitis among women with bacterial vaginosis. J Infect Dis 193: 617-624.
- Hillier SL, Krohn MA, Cassen E, Easterling TR, Rabe LK, et al. (1995) The role of bacterial vaginosis and vaginal bacteria in amniotic fluid infection in women in preterm labor with intact fetal membranes. Clin Infect Dis 20 Suppl 2: S276-278.
- Brocklehurst P, Gordon A, Heatley E, Milan SJ (2013) Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst Rev: CD000262.
- Minakami H, Hiramatsu Y, Koresawa M, Fujii T, Hamada H, et al. (2011) Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2011 edition. J Obstet Gynaecol Res 37: 1174-1197.
- United Heathcare (2007) Summary of ACOG Guidelines for perinatal care.
- Leitich H, Bodner-Adler B, Brunbauer M, Kaider A, Egarter C, et al. (2003) Bacterial vaginosis as a risk factor for preterm delivery: a meta-analysis. Am J Obstet Gynecol 189: 139-147
- McDonald H, Brocklehurst P, Gordon A (2007) Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst Rev 24: CD000262
- Sangkomkamhang US, Lumbiganon P, Prasertcharoensuk W, Laopaiboon M (2015) Antenatal lower genital tract infection screening and treatment programs for preventing preterm delivery. Cochrane Database Syst Rev: CD006178.
- Nugent RP, Krohn MA, Hillier SL (1991) Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol 29: 297-301.
- Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, et al. (1983) Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med 74: 14-22.
- Kamiya K (2013) Maternal and Child Health Statistics of Japan 2013. Editorial assistance provided by Mothers’ & Children’s Health & Welfare Association, Tokyo, 2013.
- Yamada T, Cho K, Endo T, Hanatani K, Minakami H (2009) Pregnancy outcome in women with no antenatal care in Hokkaido, Japan 2008. J Jpn Soc Perinat Neonat Med 45: 1448-1455.
- http://www.cancer.org/acs/groups/content/@editorial/ documents/document/acspc-044552.pdf
- Abe Y, Ito K, Okumura C, Niikura H, Terada Y, et al. (2004) Cervical cytologic examination during physical checkup of pregnant women: cervical cancer screening in women under the age of thirty. Tohoku J Exp Med 204: 221-228.
- Hammerschlag MR, Cummings C, Roblin PM, Williams TH, Delke I (1989) Efficacy of neonatal ocular prophylaxis for the prevention of chlamydial and gonococcal conjunctivitis. N Engl J Med 320: 769-772.
- Hillier S, Marrazzo J, Holmes KK (2008) Bacterial vaginosis. Sexually transmitted diseases, 4th edn. New York: Mc Graw Hill Medical 747.
- Farr A, Kiss H, Hagmann M, Marschalek J, Husslein P, et al. (2015) Routine Use of an Antenatal Infection Screen-and-Treat Program to Prevent Preterm Birth: Long-Term Experience at a Tertiary Referral Center. Birth 42: 173-180.
- Romero R, Mazor M (1988) Infection and preterm labor. Clin Obstet Gynecol 31: 553-584.