



Research Article - (2019) Volume 4, Issue 1
Clinical Presentation and Prognosis in Heart Failure Patients with Reduced Ejection Fraction: A Prospective One-Year Follow Up Study in National Cardiovascular Center Harapan Kita, Indonesia
2Faculty of Medicine, Universitas, Indonesia
Received Date: Nov 13, 2018 / Accepted Date: Dec 17, 2018 / Published Date: Feb 22, 2019
Copyright: ©Mohammad Risandi P, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Systolic heart failure (HFrEF) is characterized by ejection fraction of <40% and causes significant mortality and morbidity rate. We seek to characterize Indonesian patients’ clinical presentation (low to middle income country), oneyear outcome and prognostic factors of HFrEF patients.
Methods and Results: Prospective cohort with consecutive sampling method was done in National Cardiovascular Center Harapan Kita (NCCHK), Jakarta from October 2013 to March 2014. NCCHK is a national heart referral center for 34 provinces in Indonesia. Data was obtained from medical records of HFrEF patients enrolled in ASIAN-HF study. Oneyear follow up was done via medical record or phone interview. Data was analyzed using SPSS version 23. Ninety HFrEF subjects (57.3±1.17 years) were obtained. Angina was more commonly seen in higher EF group (21-40%; p=0.016). At one-year, 22.2% died. Lower EF group had higher rate of death (p>0.05). Age, rales and elevated JVP were predictive of death regardless of EF (p<0.05).
Conclusions: Angina was more commonly seen in higher EF group. Signs of congestion are associated with poorer prognosis. Low EF (<20% vs 21-40%) had clinically high rate of death (26.7% vs 13.3%, p>0.05).
Keywords
heart failure, prognosis, clinical presentation, low ejection fraction, Indonesia
Introduction
Heart failure (HF), defined as the failure of the heart to deliver sufficient oxygen to meet the demands of the body [1]. Heart failure is a chronic slowly progressive disease affecting nearly half a million people every year. Heart failure causes significant morbidity and mortality [2]. Currently there are approximately 5.8 million cases in the US and 23 million worldwide [2].
Heart failure in Asia has become a major concern due to a lot of developing countries shifting lifestyles with increase of smoking, obesity, dyslipidemia, and diabetes mellitus [3]. In Singapore alone, heart failure has become the most common cardiac cause of hospitalization with 24% cases. Singapore also has lower 5-years survival rate of 32% compared to US which is 50%.
Socio-economic factor also plays role in the characteristic of heart failure patients. Countries such as Philippines and Indonesia, low to middle income countries, have younger patients with more severe clinical manifestation compared to other Asian countries or with Western countries [4]. Indonesia has the mean age of patients of 60 years old which is younger compared to the mean age in US which is 65 years of age [5]. Previous Acute Decompensated Heart Failure Registry (ADHERE) study showed that Indonesian patients have in-hospital mortality between 6-12% with 29% rehospitalization [5]. Despite these datas, the prognosis and risk factors for hospitalization in patients with HFeEF in Indonesia remains unclear. Clearly, the true extent of burden due to heart failure remains to be fully elucidated.
This study was conducted to evaluate the characteristics and prognosis of patients with heart failure in Indonesia, to give a clear picture of the 1-year survival rate and its related factors in patients with HF.
Methods
This study used a consecutive sampling at National Cardiovascular Center Harapan Kita (NCCHK), Jakarta, Indonesia from October 2013 to March 2014 with a study design using prospective cohort. NCCHK is a national heart center referral hospital of 34 provinces in Indonesia consisting of archipelago. Data was obtained from heart failure patients with reduced ejection fraction (EF≤40%) of non-valvular etiology enrolled in Asian Sudden Cardiac Death in Heart Failure Registry (ASIAN – HF). Protocols of the registry have been explained elsewhere [6]. Informed consent was obtained prior to data collection. Patients’ laboratory and physical examination data was obtained on hospital admission and patient’s personal information was obtained via questionnaires. Ejection fraction (EF) was measured using echocardiography by a third party. Data collected was validated by blinded third parties. Follow-up was obtained after 1 year via medical record and phone interview. Patients who cannot be contacted were presumed as lost to follow up. Data was analyzed with intention-to-treat protocol and statistical analysis was done using SPSS version 23 with appropriate statistical tests. Data presented as mean and median±SEM unless stated otherwise.
Results
Demographics We obtained 90 subjects with mean age of 57.3±1.17. 62.2% of the subjects were between 31-59 years old and 83.3% are male. Most of the subjects were obese (37.8%). Subjects were mostly diagnosed between 1-5 years ago prior to hospital admission (48.9%) with a previous history of CAD (71.1%). Etiology was found to be mostly ischemic (87.8%). These subjects were comprised of mostly ex-smokers (61.1%) and non alcohol drinker (78.9%). EF of subjects were between <11 (1.1%), 11-20 (32.2%), 21-30 (50%), 31-40 (16.7%). Cumulatively, EF was between 21-40% (66.7%) and ≤20% (33.3%).
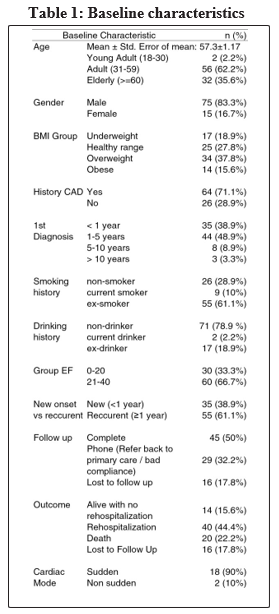
Clinical presentation Symptoms upon admission
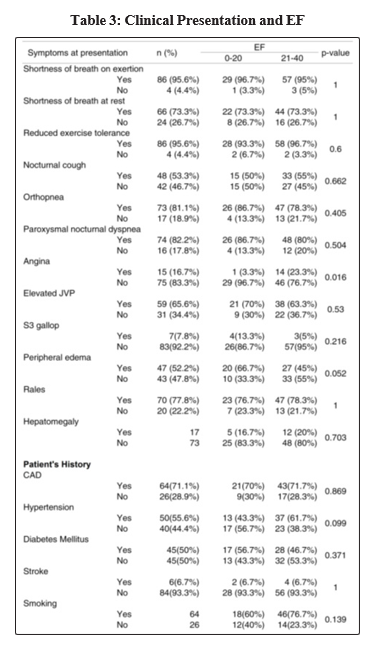
Almost all subjects had shortness of breath on exertion (95.6%), inability to do exercise (95.6%), shortness of breath at rest (73.3%), orthopnea (81.1%), Paroxysmal nocturnal dyspnea (82.2%), 53.3% had nocturnal cough and 16.7% reported previous angina. Upon physical examination, 65.5% had elevated JVP, 52.2% suffered from edema, 77.8% had pulmonary rales. No subjects had positive hepatojugular reflex and 18.9% had hepatomegaly. Angina was more likely in patients with EF 21-40% (23.3% vs 3.3%), p=0.016; Edema was more likely in patients with EF < 20% (66.7% vs 45%), p=0.052.
Upon further tests, 87.8% had chest X-ray abnormalities, 7.8% did not have an X-ray. Only 20% of the samples had ECG abnormalities. 36.7% had hyponatremia and 34.4% had hypokalemia. 57.8% of the subjects showed reduced GFR < 60.
Previous history
Half of the subjects recruited had history of hypertension (55.6%), diabetes mellitus (50%) and only 6.7% had history of previous stroke.
Lost to follow up and outcome
At the end of the 1 year follow up, 22.2% died, 60% were alive and 17.8% were lost to follow up. From the subjects alive, 32.2% did not return to the national cardiac centre Harapan Kita due to bad compliance or initiated alternative treatment. Fifty percent of the patients returned and had good compliance.
Further analysis of compliance showed that 50% of patients with EF < 20% returned to Harapan Kita, 43.3% had bad compliance or initiated alternative treatment and 6.7% were lost to follow up. In patients with EF 20-40%, similarly 50% had good compliance, 26.7% had bad compliance or initiated alternative treatment, 23.3% were lost to follow up.
Adverse effect
Out of the total subjects, 15.6% were alive without rehospitalization, 44.4% were alive with rehospitalization, 22.2% died. 17.8% were lost to follow up. In patients with EF ≤20%, only 6.6% were lost to follow up, 26.7% died, 46.7% were rehospitalized and 20% were alive without any rehospitalization.
In patients with EF between 21-40%, 23.3% were lost to follow up, 13.3% died, 43.3% were rehospitalized and similarly 20% did not suffer from rehospitalization. Causes of death were mostly heart failure (65%), cardiac arrest (15%), arrhythmia (5%), myocardial infarction (5%) and others (10%). Deaths were mostly sudden (90%) and non-procedure related (100%). In patients that were alive, 51.9% reported better functional class, 37% did not worsen or improve and 11.1% worsened. 66.7% had a decrease in the shortness of breath at rest. However, most patients felt similar symptoms of shortness of breath of exertion (83.3%), exercise intolerance (85.2%), nocturnal cough (44.4%), orthopnea (61.1%), PND (50%), angina (79.6%), peripheral edema (57.4%).
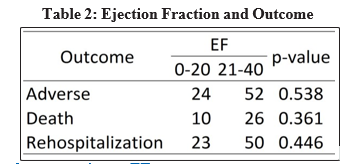
EF vs Outcome
Previously, Siswanto et al. showed EF < 20% was a predictor for mortality. We categorized the data into low (1-20%) and moderate (21-40%) ejection fraction and crossed it with outcome (adverse outcome, death and rehospitalization) [7]. We found no statistical significance was observed. However, raw data suggests increased mortality rate in ≤20% vs 21-40% group (26.7% vs 13.3%). Data is shown in Table 2.
Clinical presentation vs EF
We evaluated the presence of each sign and symptoms in the subjects to their ejection fraction. Surprisingly, we found little statistical significance in majority of the symptoms. Statistical significance was seen in angina and EF as well as age and EF.
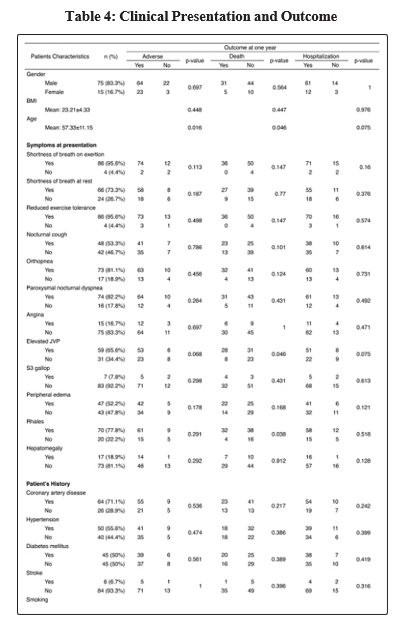
Clinical presentation vs outcome
As presented in table 4, we evaluated the presence of clinical manifestation against outcome (adverse outcome, death and hospitalization). We found statistical significance in age and adverse outcome (p=0.009), age and death (p=0.016). Rales and elevated JVP is associated with death (p=0.038, p=0.046).
Discussion
Patients were presented with shortness of breath upon exertion (95.6%), reduction in exercise tolerance (95.6%), paroxysmal nocturnal dyspnea (82.2%). Similar results were presented by Goldberg,et al. in 2014.8 They found that in 4,537 patients with heart failure, 93% presented with dyspnea. From physical examination, we found that the patients mostly had rales (77.8%), elevated JVP (65.6%), and edema (52.2%), also consistent with results presented by Goldberg, et al. [8].
In our study, the mean age of 57 years showed a younger population suffering from heart failure compared to other studies conducted in Europe and America. Regardless, age was proven to have significant association to adverse events and mortality (p=0.016 and p=0.046). From a systematic review by Rahimi, et al. age was proven to be a valuable risk predictor for patients with heart failure [9]. This was found consistently throughout studies from the year 1955 to 2013. Age could serve as predictor of mortality and hospitalization consistent to our findings.
Heart failure patients with reduced ejection fraction (HFrEF) are more likely to suffer from previous history of ischemic etiology of heart failure (HF). We found that patients in higher EF group (EF of 21 – 40%) had higher prevalence of angina. This result is in concordance to previous findings. It is believed that these patients had more viable myocardial tissue thus patients can still report the complaints of angina. Angina itself is a symptom commonly present in patients with impaired cardiovascular diseases. This mainly emerges due to imbalance of blood supply to the myocardial tissue. Lack of oxygen delivery to the viable tissue will result in anaerobic metabolism and ischemia in which ATP will be broken down to adenosine and triggers the A1 receptors in cardiac nerve endings. Thus, it is only logical to conclude that patients with viable tissues are more likely to suffer from angina in comparison to those with non – functioning myocardial tissues. In patients with heart failure, especially those resulting from ischemic etiologies, the impaired blood flow to the tissue will result in angina while also reducing the ability of the heart to pump the blood to the tissues thus augmenting the effects.
Mentz et al followed up 2376 patients with EF less than 40% for 4.5 years and found that patients experiencing angina were less likely to suffer from adverse events such as death, myocardial infarction (MI), or revascularization with 5 – year risk of 85% in comparison to 87% in patients without angina (p=0.01) [10]. However, study by Badar, et al. which followed up 4870 patients from the Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA) found that patients with angina is linked with higher risk of re-hospitalizations and coronary events [11]. Patients with angina were associated with higher ejection fraction although worse functional class status [11]. The increased hospitalization was due to heart failure symptoms [11]. Similar result was presented in patients with ischaemic cardiomyopathy experiencing persistent angina who had higher hospitalization but also death in comparison to patients without [12]. We found that patients who experienced angina were associated with higher EF (23.3% vs 3.3%, p=0.016) but we found no significant association to rehospitalization nor death. Similar result was found in the Surgical Treatment for Ischaemic Heart Failure (STITCH) trial in which angina was not found to predict all-cause mortality in patients with LV dysfunction and history of coronary artery disease (CAD) [13]. Regarding hospitalization, we consider the result was due to the local culture in which patients would not go to the hospital up until the symptoms were severe enough. Patients were also given medications to relieve chest pain when it occurred thus it is not impossible that these patients took symptom of angina lightly and did not go to hospital for its relief.
As it has been mentioned above, patients experiencing angina are often associated to the history of coronary artery disease (CAD). However, in this study history of coronary artery disease (CAD) was not significantly related to ejection fraction nor adverse effects, death, and rehospitalization. Most of the patients enrolled in the study had history of CAD (71%) but from these patients, only 16% experienced angina. We also did not find any association between history of CAD and anginal symptoms (p = 0.757). Similar result was also found by Kureshi, et al. from the ACC PINACLE registry [14]. It was found that from 1154 patients enrolled, 67.7% reported no angina symptoms and more than half of the total subjects had already received optimal medical treatment.
It may also be the reason to what we found in this study in which patients had given optimal medical treatment. Signs of congestion, such as elevated jugular venous pressure (JVP), peripheral edema, and pulmonary rales were also found to be significant in few parameters that we are looking at. In patients with heart failure, congestion is the most common cause of admission [15]. Patients with heart failure develop congestive symptoms such as above by the high left ventricular (LV) pressure thus trigger further subendocardial ischemia which will alter the structure of the chambers and causing secondary mitral regurgitation, activation of renin – angiotensin – aldosterone system (RAAS), inflammatory mediators, and decrease of renal function. In our study, 85.6% of patients presented with signs of congestion such as above, in average with 2 symptoms. We found that peripheral edema had no association to ejection fraction, adverse events, hospitalizations, or death. However, patients who lower EF tend to develop peripheral edema compared to those with higher EF (66.7% vs 45%, p=0.05). While we also found that increased jugular venous pressure (JVP) and rales are significantly associated to death after 1-year follow – up period (p<0.05). These results support Damman, et al. in proving that symptoms of congestion are markers of worse prognosis [16].
Among our participants, 44.4% were readmitted during the course of 1-year period. This result was also in concordance with previous studies. Previous studies surveyed rehospitalization for 30 days and 60 to 90 days post discharge. Twenty seven percent of patients were rehospitalized within 30 days and more than 30% of the cause was worsening HF [17]. In another trial, Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST), 24% of patients with HF were rehospitalized within 30 – days post – discharge with more than 40% were due to HF [18]. For longer period of follow up which was 60 to 90 days, the rate of hospitalization was 30% [19]. ADHERE - Asia Pacific study also exhibited that Asian patients had longer hospital stay and higher in – hospital mortality [4].
Death occured in 22.2% of all subjects and from which was due to sudden cardiac death (SCD), taking 90% account of all-cause mortality in our study. Previous study has found that mortality rate of patients with HF is 20% over 4 to 5 years and 30% of those were due to sudden cardiac death, supportive of findings of this study [20]. Previous studies have accounted patients with EF of 35% or less to be patients in high risk group of SCD [21]. However, in this study, all patients enrolled had EF of 40% or less and after divided into lower (≤20%) and higher (21-40%) EF group, there was no significant association to death nor hospitalization. This result might be due to limited amount of participants. It is also possible that after patients had EF lower than 35% there will be no difference in mortality or adverse events. Clinically, mortality rate of lower EF group was roughly double the rate observed in the higher EF group (26.7% vs 13.3%) but rehospitalization rate was found to be similar.
Our study has several limitations. First, the number of participants in this study might be insufficient to show statistically significant result in various factors. Secondly, gender-wise our study is too male-dominated. However, our study is also one of the very few studies that investigate and showed the rate of loss to follow up in Indonesia, where barriers to effective tracking and follow up exist. While our study had low number of participants compared to larger trials, we were able to show several factors of significance in this pilot study, serving as probable points of interest for larger trials. Lastly, we were able to show clinical presentation of patients admitted with HFrEF of both low and moderate ejection fraction.
Conclusion
Angina is more commonly found in HF patients with higher EF. Although not statistically significant, patients with lower EF had more signs of congestion. In addition, we also found that signs of congestion are associated to poorer prognosis at 1-year follow-up. We also found high readmission and mortality with sudden death as the most common mode of death. The extensive burden of HF in Indonesia has shown that prevention and lifestyle modifications are significant.
Acknowledgements
We would like to thank all the Cardiologist staffs, Research and Development Unit, and Institutional Review Board at National Cardiovascular Center Harapan Kita, Jakarta, Indonesia who have aided authors in the course this study.
References
- McMurray JJV, Adamopoulos S, Anker SD, Auriccio A, Bohm M, et al. Acute and chronic heart failure. ESC 2012; 33: 1787- 1847.
- Roger VL. Epidemiology of heart failure. Circ Res 2013; 113: 646-659.
- Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, MurphyA. Growing epidemic of coronary heart disease in low- and middle- income countries. Curr Probl Cardiol. 2010: 35(2): 72-115.
- Atherton JJ, Hayward CS, Wan Ahmad WA, Kwok B, Jorge J, Hernandez AF, et al. Patient characteristics from a regional multicenter database of acute decompensated heart failure in Asia Pacific (ADHERE International - Asia Pacific). J Card Fail 2012;18(1): 82-8.
- Siswanto BB, Radi B, Kalim H, Santoso A, Suryawan R, Erwinanto, Antono E, Santoso T. Heart Failure in NCVC Jakarta and 5 hospitals in Indonesia. CVD Prevention and Control. 2010;5(1): 35-38. doi: 10.1016/j.cvdpc.2010.03.005.
- Lam CS, Anand I, Zhang S, Shimizu W, Narasimhan C, Park SW, et al. Asian Sudden Cardiac Death in Heart Failure (ASIAN-HF) Registry. Eur J Heart Fail 2013;15(8): 928-36.
- Siswanto BB, Sunanto, Munawar M, Kusmana D, Hanafiah A, Waspadji S, et al. Predictor of mortality and rehospitalization of acute decompensated heart failure at six months follow up. Crit Care & Shock 2006; 9(3): 61-7
- Goldberg RJ, Spencer FA, SZklo-Coxe M, Tisminetzky M, Yarzebski J, Lessard D, et al. Symptom presentation in patients hospitalized with acute heart failure. Clin Cardiol 2010; 33(6): E73-80.
- Rahimi K, Bennett D, Conrad N, Williams TM, Basu J, Dwight J, et al. Risk Prediction in patients with heart failure: a systematic review and analysis. J Am Coll Cardiol HF 2014; 2: 440-6.
- Mentz RJ, Fuzat M, Shaw LK, Philips HR, Borges – Neto S, Felker GM, et al. Comparison of clinical characteristics and long– term outcomes of patients with ischemic cardiomyopathy with versus without angina pectoris (from the Duke Databank for Cardiovascular Disease). Am J Cardiol 2012;109: 1272 –1277.
- Badar AA, Perez-Moreno AC, Jhund PS, Wong CM, Hawkins NM, Cleland JGF, et al. Relationship between angina pectoris and outcomes in patients with heart failure and reduced ejection fractionL an analysis of the controlled rosuvastatin multinational trial in heart failure (CORONA). Eur Heart J 2014; 35: 3426– 3433.
- Mentz RJ, Broderick S, Shaw LK, Chriswell K, Fiuzat M, O’Connor CM. Persistent angina pectoris in ischaemic cardiomyopathy: increased hospitalization events. Eur J Heart Fail 2014; 16: 854-860.
- Joliceour EM, Dunning A, Castelvecchio S, Dabrowski R, Waclawiw MA, Petrie MC, et al. Importance of angina in patients with coronary disease, heart failure, and left ventricular systolic dysfunction: insight from STITCH. J Am Coll Cardiol 2015; 66: 2092-2100.
- Kureshi F, Shafiq A, Arnold SV, Gosch K, Breeding T, Jones PG, et al. he Prevalence and Management of Angina Among Stable CAD Patients in Outpatient Cardiology Practices in the United States: Insights From the Angina Prevalence and Provider Evaluation of Angina Relief (APPEAR) Study. Circulation 2015; A111.
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol 2013; 61(4): 391- 403.
- Damman K, Voors AA, Hillege HL, Navis G, Lechat P, van Veldhuisen DJ, et al. Congestion in chronic systolic heart failure is related to renal dysfunction and increased mortality. European Journal of Heart Failure 2010;12: 974-982.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360: 1418 -28
- O’Connor CM, Miller AB, Blair JE, et al. Causes of death and rehospitalization in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction: results from Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST) program. Am Heart J 2010; 159: 841-9.
- Fonarow GC, Stough WG, Abraham WT, et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF registry. J Am Coll Cardiol 2007; 50: 768 -77.
- Buxton AE, Lee KL, Fisher JD, et al. Multicenter Un- sustained Tachycardia Trial Investigators. A random- ized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med 1999; 341:1882-90.
- Houmsse M, Franco V, Abraham WT. Epidemiology of sudden cardiac death in patients with heart failure. Heart Failure Clin 2011; 7: 145-155.