
Japanese Journal of Medical Science(JJMS)
ISSN: 2996-2536 | DOI: 10.33140/JJMS

Research Article - (2024) Volume 2, Issue 2
Challenges in Neurosurgery during Armed Conflict in Sudan
2Cardiac Center Sudan, Khartoum, Sudan
3Ebrahim Malik Hospital, Khartoum, Sudan
4Almobaruk Hospital, Kassala, Sudan
Received Date: Jun 04, 2024 / Accepted Date: Jun 28, 2024 / Published Date: Jul 05, 2024
Copyright: ©Â©2024 Sawsan A H Aldeaf, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Aldeaf, S. A. H., Ibrahim, H. A. M., Elabdin, M. M. Z., Ali, M. E. A., SalahEldin, A. et al. (2024). Challenges in Neurosurgery during Armed Conflict in Sudan. Japan J Med Sci, 2(2), 01-06.
Abstract
Introduction: Sudan armed conflict between rapid support force (RSF) and Sudanese army was one of the wicked wars, the conflict has a terrible physical, emotional, and economic costs for Sudanese, this war caused great traumatic injuries among civilians despite the number of affected persons, during the period of this armed conflict, there is no data or reports regarding affected civilians.
Material and Methods: This is descriptive experience based and cross sectional study done at Almubarak hospital, kassala town from July 2023 to March 2024. In fact, the study was designed to reflect our neurosurgical experience during the period of armed conflict between rapid supporting force (RSF) and Sudanese army, hence the war is still going on, also, this paper describe the neurosurgical circumstances in Sudan throughout the war compared with other war that occurring in the middle East and worldwide . Modification and replacement in neuro-anesthia was made to cope with this situation (war period).
Results: During the period of this study, we made some changes in techniques and treatment strategies for treating patients with neurosurgical problems. Our data revealed, 18 patients were presented with extra-dural haemorrhage (EDH), depressed fracture was detected in 42 of the patients, and hydrocephalus 12, abscess 5, tumor were 8, and sub-dural haemorrhage (SDH) was encountered in 41 patients.
Keywords
Armed Conflict, Neurosurgery, Almubarak Hospital, NCNS, Kassala
Introduction
War is a time of great destruction, losses, and change. War shapes many aspects of human history and contributes heavily to modern public structure. It is known that most war injuries have been inflicted in the form of head and spine trauma, making neurosurgeons play a fundamental role in wartime and obligated to participate in saving lives of the patients in war [1].
Although war is associated with large-scale physical and emotional damage, it has led to widespread of medical innovation and progress, for example during the World War 1 WWI (1914–1918), there was significant rate of neurotruma that create an opportunity improvement in neurologic care and neurosurgical treatment [2]. In this context, Harvey Cushing served as an army neurosurgeon in France from 1917 to 1918, during 1917-1918 Cushing made great changes in treating patients with neurosurgical problems.
His operative techniques and treatment strategies helped reduce mortality in cranial trauma from 50%–60% during the early years of the war to 29% [3].
Rational of the Study
There have been numerous wars in the Middle East in recent decades. These wars have put a heavy burden on the afflicted countries, numerous wars in consecutive years since 1980 have led to a decline in many health indicators and enforced a heavy burden on the country.
Sudan armed conflict between rapid support force (RSF) and Sudanese army was one of the wicked wars, the conflict has had terrible physical, emotional, and economic costs for Sudanese, this war caused great traumatic injuries among civilians despite the number of affected persons, during the period of this armed conflict, there is no data or reports regarding affected civilians. This war affected all aspects of people’s lives, including health facilities, in addition to this, most of the health professionals were enforced to displace from Khartoum, the displaced neurosurgical staff established a minimum neurosurgical setting in safe cities and towns. Regarding neurosurgeons, they were not dealing with neurotruma only, but with all other neurosurgical and neurological diseases. In some instance the neurotruma patients transported from the battle area to the town that he or she might find neurosurgical services.
Objective
1/ To describe the neurosurgical situation in Almubarak hospital, kassala, Sudan, from July 2023 to March 2024 during armed conflict between rapid support forces (RSF) and Sudanese army.
2/ To explore surgical outcome of the patients during the war in Almubarak hospital, kassala, Sudan, from July 2023 to March 2024 during armed conflict between rapid support forces (RSF) and Sudanese army.
Materials and Methods
This is descriptive experience based and cross sectional study done at Almubarak hospital, kassala town from July 2023 to March 2024. In fact, the study was designed to reflect our neurosurgical experience during the period of armed conflict between rapid supporting force (RSF) and Sudanese army, hence the war is still going on, also, this paper describe the neurosurgical circumstances in Sudan throughout the war compared with other war that occurring in the middle East and worldwide . In the present study, our neurosurgical experierence integrated patients with neurosurgical conditions. The demographic data included age, gender, residence diagnosis, CT brain, type of operation and recovery from anesthesia were obtained from the record files. Regarding the neurosurgical instruments, in point of fact there was nothing to label as neurosurgical instruments, for instance, at one time electrical saw, which used for cutting Gypsum splint in orthopedics practice, was used in craniotomy in emergency hematoma evacuation, naso-gastric tube size 8 used for draining cerebrospinal fluid in patients with interventricular heamorrhge instead of using external ventricular drain (EVD). Surgical instruments were available in form of surgical blades, forceps, some self- retractors; sliver ruler was modified to function as brain retractor. Most of suture materials were not the appropriated for neurosurgical setting.
Taking the neuro anesthesia during this war, there was obvious deficiency in aneathesitic agent's which included Isoflurane, Nitrous oxide, medical air and opioids in a particular Fentanyle. Beside this, lack of patient circuit and functioning intensive care unit (ICU).
Modification and Replacement
In this study, isoflorane replaced by low Minimal Alveolar Concentration (MAC) halothane<0.6%, or total intravenous anesthesia (TIVA) (propofol continuous infusion). Instead of Nitrous oxide and medical air, 100% oxygen 4 litter flows was used. along with that, opioids ( fentanyle) replaced by Shiva regiment for the first time documented to be used in Sudan ( lidocain 2% intravenous 1.5mg/kg + paracetamol 1 gm intravenous + magnisum sulphate 50mmol/ kg or 2gm intravenous) (4). The aforementioned drugs were mixed in paracetamole bottle and infused slowly over 15 to 20 minutes. In this study, patient's circuit was reused after been cleaned and sterilized using sidex, but the filters were changed regularly every one month. Moreover, in induction phase we used propofol 2-3 mg/kg or midazolam according to the patient condition, morphine 0.05 mg/kg intravenous was used for analgesia, atracurium 0.5mg/kg was used for muscle relaxant, in addition to that, atropine, ondanseteron and antibiotic were used. In maintenance phase, 0.6% halothane or TIVA was used for hypnosis. In this phase, the analgesia was maintained using Shiv regiment, for muscle relaxants patient was kept on atracurrium, if not available we kept patient on spontaneous breathing. Recovery phase was proceeded as usual without modification [5].
Results
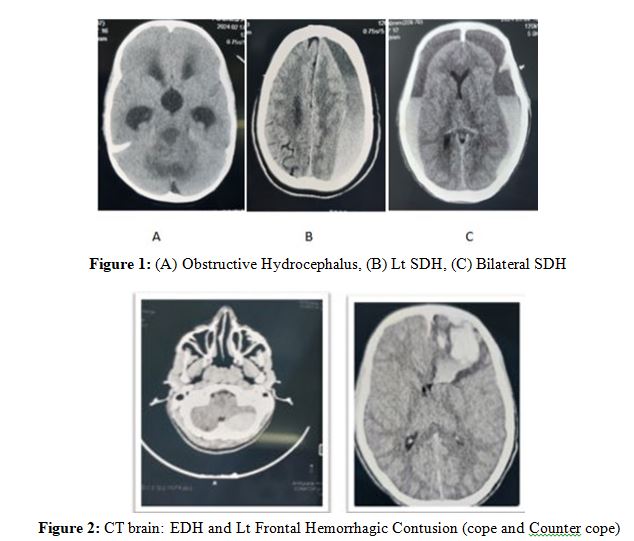
During the period of this study, we made some changes in techniques and treatment strategies for treating patients with neurosurgical problems. This study included 136 patients, male were 111 (81.6%), female were 25 (18.4%). The most frequent age group was ranging from 11 to 20 years which was detected in 18.4% of the patients (Table 1). Regarding diagnosis of the patients, sub-dural haemorrhage (SDH) was encountered in 41 patients (30.1%), the sub classes of SDH showed that, patients with acute SDH were 6 (14.6%), sub-acute were 17 (41.4%) and chronic were 19 (46.3%). Our data revealed, 18 patients were presented with extra-dural haemorrhage (EDH), depressed fracture was detected in 42 of the patients, and hydrocephalus 12, abscess 5 and tumor were 8 (Table 2). In this study 124 (91.1%) of the patients were recovered Immediately from anesthesia.
|
Gender |
|
|
Female |
Male |
|
111 |
25 |
|
Age group |
|
|
Groups |
Frequency |
|
|
14 |
|
1-10 years |
14 |
|
11-20 years |
21 |
|
21-30 years |
19 |
|
31-40 years |
14 |
|
41-50 |
5 |
|
51-60 |
17 |
|
61-70 |
20 |
|
71-80 |
11 |
|
>80 |
1 |
|
Total number |
136 |
Table 1: Frequency of Gender and Age in Groups in Patients during War in Sudan
|
Diagnosis |
|
|
SDH |
41 |
|
EDH |
18 |
|
Depressed fracture |
42 |
|
Hydrocephalus |
12 |
|
Brain tumor |
8 |
|
abscess |
5 |
|
Meningiocele |
5 |
|
Others |
5 |
|
Total |
136 |
Table 2: Types of Diagnosis in Patients during War in Sudan
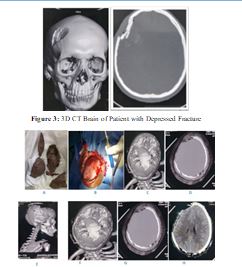
Figures 4: (A to H)| 14 years boy from Gedarif involve in Crash RTA, his Head was compressed between the 2 cars, thus 5 Pieces of Fragmented bone left on the road, the patients was presented with GCS 13/ 15
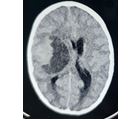
Figure 5: 6 Years boy from Port-Sudan, Presented with History of Rabidly Progressing Lt side Weakness that end in Deterioration level of consciousness (GSC 9/15), underwent Rt Fronto-Temporal Crainatomy and excision of the cystic part and nodular, patient showed Dramatic improvement in conscious level and weakness, the patient was Discharged home walking.

Figure 6(A to C:| 55 Years Male from white Nile, presented with History of scalp swelling, Rt side weakness and convulsions, intra- operative finding there was dilated scalp vessels (A), hence silk sutured was used for ligation, the bone was highly vascular and hyper osteotic, it was very difficult to be opened, the tumor was ill define capsule, resection was done.
Discussion
It is known that the development of neurological surgery throughout history has been obvious in the literature, and various neurosurgical management protocols have been reviewed and modified during wars time. Without a doubt, military neurosurgeons played a crucial role in the development of neurosurgery procedures, the procedures included; extensive decompression to prevent increased intracranial pressure (ICP) and secondary injuries, as the same time the transfer opportunity was provided to the patient who needs more advanced neurosurgical facilities (1). Unfortunately what is going on during Sudanese armed conflict, most of the neurosurgeons were enforced to leave their duties and displaced to other town or outside Sudan. The battle occurring in the capital of Sudan (Khartoum) and extended to other vital cities, indeed all the big military hospitals are located in the capital of Sudan (Khartoum) and some are scattered over other towns, the setting of these hospitals are not outfitted for neurosurgery, and till now there is no data available for patients.
The management of head injuries during the war owes much to Harvey Cushing and his contribution to World War I The previous approach to penetrating head trauma included aggressive debridement of the penetration site and removal of the penetrating fragments [3]. Later, this method was proven to lead to worse outcomes compared with more conservative approaches [6].
Much of this progress is due to war-related experiences. Owing to the number and severity of war injuries and the limitations caused by war, surgeons have had to examine different methods and design special protocols for patient management. Our study providing the anesthesia protocol, we managed to anesthetize the patient by using Shiva regimen which used in emergency situation [5].
There have been various wars in the Middle East in recent decades. These wars have put a heavy burden on the afflicted countries one of the most important wars in this region in the late 20th century was the Iran-Iraq war, which led to publication of neurosurgical experiences regarding advancement in the management of related head trauma, including some aspects of minimal surgical debridement [7].
In the present study, our results providing surgical intervention, showed that, handling patients with different neurosurgical conditions of which head injured with depressed fracture that not only need elevation but debridement hence those patients taking a long journey to find a town in which neurosurgical services might be found. Nevertheless, throughout World War II (WWII) (1939–1945) [8]. Neurosurgeons required to provide treatment closer to places of battle, likely to decrease the time of operation and craniotomy, which is not the case in Sudan conflict, the handle and management of patients was taken in hospitals which situate in town far from Battles taking place.
Moreover most of the studies which held during war focusing on the surgical procedures and technique like the British and veterans who were involved in the war between 2005 and 2006 [9]. Likewise the aim of this study is to describe the neurosurgical situation during the armed conflict in Sudan and to explored the various neurosurgical conditions.
Declaration:
We declare that, this work was not submitted to any other institution and there is no conflict of interest.
References
1. Dowdy, J., & Pait, T. G. (2014). The influence of war on the development of neurosurgery: historical vignette. Journal of Neurosurgery, 120(1), 237-243.
2. Horswill, S. C., & Carleton, R. N. (2021). Changes in our understanding of trauma and the human psyche as a consequence of war: A brief history. In Handbook of Posttraumatic Stress (pp. 15-37). Routledge.
3. Birk, H., Stewart, C., & Kosty, J. A. (2022). The birth of modern military neurosurgery through the eyes of Harvey Cushing’s war memoir From a Surgeon’s Journal, 1915-1918. Neurosurgical Focus, 53(3), E8.
4. Piacevoli, Q., Minto, C., & Schnider, T. (2011). Total Intravenous Anaesthesia & Target Controlled Infusion. A Comprehensive Global Anthology. Springer Cham, 824.
5. Ballard, R. (2015). The Oxford Handbook of Sikh Studies: Reflections on the current State of Play in an Emergent Discipline.
6. Kinsman, M., Pendleton, C., Quinones-Hinojosa,A., & Cohen- Gadol, A. A. (2013). Harvey Cushing's early experience with the surgical treatment of head trauma. Journal of the History of the Neurosciences, 22(1), 96-115.
7. Maroufi, S. F., Sohrabi, H., Ohadi, M. A. D., Mohammadi, E., & Habibi, Z. (2022). Neurosurgery in 21st-Century Wars in the Middle East: Narrative Review of Literature. World Neurosurgery, 166, 184-190.
8. Stahnisch, F. W. (2016). German emergency care in neurosurgery and military Neurology during world war II, 1939-1945. In War neurology (Vol. 38, pp. 119-131). Karger Publishers.
9. Roberts, S. A. G., Toman, E., Belli, A., & Midwinter, M. J. (2016). Decompressive craniectomy and cranioplasty: experience and outcomes in deployed UK military personnel. British Journal of Neurosurgery, 30(5), 529-535.