
World Journal of Radiology and Imaging(WJRI)
ISSN: 2835-2440 | DOI: 10.33140/WJRI


Case Report - (2024) Volume 3, Issue 1
Cerebral Dermoid Cyst Ruptured Intraventricularly and in the Subarachnoid Spaces
Received Date: May 30, 2024 / Accepted Date: Jun 21, 2024 / Published Date: Jun 26, 2024
Copyright: ©Â©2024 H.Lamri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Lamri, H., Nuiakh, J., Remmal, A., Rachidi, S. A. (2024). Cerebral Dermoid Cyst Ruptured Intraventricularly and in the Subarachnoid Spaces. World J Radiolo Img, 3(1), 01-02.
Abstract
The intrcranial dermoid cyst is a benign congenital tumor, which generally develops in the posterior fossa, extra-axially. Its spontaneous rupture represents a rare event, with a difficult clinical diagnosis, requiring the use of imaging. We report a case of a left frontal cerebral dermoid cyst spontaneously ruptured in the ipsilateral lateral ventricle and subarachnoid spaces which manifested by electric shock type headaches and diagnosed by brain CT.
Keywords
Ruptured Dermoid Cyst, CT, Fat Density
Introduction
The intrcranial dermoid cyst is a benign congenital tumor, which generally develops in the posterior fossa, extra-axially. Its spontaneous rupture represents a rare event, with a difficult clinical diagnosis, requiring the use of imaging. We report a case of a left frontal cerebral dermoid cyst spontaneously ruptured in the ipsilateral lateral ventricle and subarachnoid spaces which manifested by electric shock type headaches and diagnosed by brain CT.
Observation
This is a 34-year-old patient with head trauma in childhood who consulted for acute electric shock-type headaches. The neurological examination was unremarkable. A brain CT performed urgently revealed the presence of a cerebral lesion, left basi frontal, polylobed, well limited, heterodense with fatty and calcium component arriving in contact with the base of the skull measuring 23.6 x 21.6mm. This lesion communicates with the ipsilateral lateral ventricle at the level of the frontal horn, thus creating a liquid-fat level, with the presence of multiple droplets of fatty density disseminated subarachnoidally.
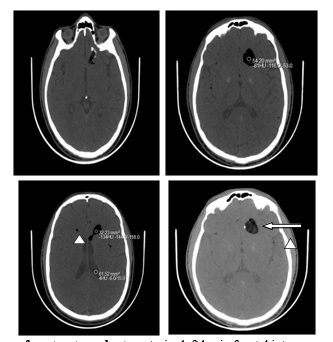
CT in axial sections without injection of contrast product : anterior left basi - frontal intra-parenchymal brain lesion , oval with finely heterogeneous fat density (white arrow) with calcified wall in places, ruptured in the ipsilateral lateral ventricle creating a liquid-fat level, with presence at the level of the subarachnoid spaces small droplets of fat density (arrowhead).
Discussion
The dermoid cyst is a benign, congenital lesion of the central nervous system. It is uncommon since it represents 0.04 to 0.7% of intracerebral tumors [1]. It develops at the expense of embryonic remnants of the ectoderm and mesoderm, explaining their location near the midline. They are preferentially located supra and parasellar , in the basi -frontal and in the posterior cerebral fossa [2]. Histologically Dermoid cysts are made up of a squamous epithelium, composed of different lipid elements (keratinized debris, sebaceous secretions, cholesterol crystals, etc.), which may contain within them hair, bone or cartilage while their walls can be the site of calcifications. Clinically, the symptoms vary depending on the location and size of the cyst; it can be asymptomatic or manifest as a syndrome of intracranial hypertension with headaches and visual disturbances, a cerebellar syndrome, or cranial nerve damage. The main complication is rupture, which can be spontaneous or post-traumatic [3], and can cause various symptoms such as headaches, epileptic seizures, sensory-motor deficits and aseptic meningitis.
Imaging based on CT and especially MRI allows the positive diagnosis of the rupture. On CT, the dermoid cyst appears as a well-defined, homogeneous hypodense process [4], not enhanced after injection, often the site of parietal calcifications [5]. The rupture is often proven by the demonstration of fine lipid droplets disseminated in the subarachnoid spaces and sometimes intraventricularly [6], responsible for the fat-liquid level which has a good diagnostic value. On MRI, the dermoid cyst is visible in the form of a well-defined mass, with a generally heterogeneous signal, hyper intense in T1, iso or hyper intense in T2 and hyper intense on T2 FLAIR sequences [7]. The heterogeneity of the signal within the mass is due to the fatty, sebaceous and hair content, and the T2 signal is a reflection of the abundance of one of these components compared to the others. [4 ]. Wall calcifications, when present, are hyposignal on T1 and T2 sequences and are generally better visualized on the scanner. Given the richness in lipids, the T1 sequence with saturation of the fatty signal makes it possible to confirm the diagnosis of rupture by showing the attenuation of the signal from the mass and the diffusion sequence shows a hyper signal within the lesion which would be due to at a low water content with a moderately decreased ADC [8]. The main differential diagnoses are : epidermoid cyst which can be differentiated from dermoid cyst by its signal which is close to that of the cerebrospinal fluid [8], intracranial lipoma, and immature intracranial teratoma.
Conclusion
The dermoid cyst is a rare and benign brain tumor, and its rupture is exceptional and often spontaneous. Its clinical presentation is polymorphic and requires radiological confirmation based on CT but especially MRI which makes it possible to specify the nature of the cyst, its location , the extent of its rupture, and to screen for possible complications.
References
- Rubin, G., Scienza, R., Pasqualin, A., Rosta, L., & Da Pian, R. (1989). Craniocerebral epidermoids and dermoids: A review of 44 cases. Acta neurochirurgica, 97, 1-16.
- Karabulut, N., & OÄ?uzkurt, L. (2000). Tetraventricular hydrocephalus due to ruptured intracranial dermoid cyst. European Radiology, 10, 1810-1811.
- Phillips, W. E., Martinez, C. R., & Cahill, D. W. (1994). Ruptured intracranial dermoid tumor secondary to closed head trauma. Journal of Neuroimaging, 4(3), 169-170.
- Venkatesh, S. K., Phadke, R. V., Trivedi, P., & Bannerji, D. (2002). Asymptomatic spontaneous rupture of suprasellar dermoid cyst: a case report. Neurology India, 50(4), 480-483.
- Rai, S. P. (2009). Ruptured intracranial dermoid cyst.Neurology India, 57(1), 98-99.
- Das, C. J., Tahir, M., Debnath, J., & Pangtey, G. S. (2007). Ruptured intracranial dermoid. Journal of Neurology, Neurosurgery & Psychiatry, 78(6), 624-625.
- Wilms, G., Casselman, J., Demaerel, P., Plets, C., De Haene, I., & Baert, A. L. (1991). CT and MRI of ruptured intracranial dermoids. Neuroradiology, 33, 149-151.
- Orakcioglu, B., Halatsch, M. E., Fortunati, M., Unterberg, A., & Yonekawa, Y. (2008). Intracranial dermoid cysts: variations of radiological and clinical features. Acta neurochirurgica, 150, 1227-1234.