
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Review Article - (2020) Volume 2, Issue 2
Can we predict & prevent complications of pcnl?
2Vivek Joshi, Head, Department Of Urolog, Bt Savani Kidney Ospital, Rajkot, Gujarat, India
Received Date: Mar 30, 2020 / Accepted Date: May 01, 2020 / Published Date: May 16, 2020
Copyright: ©Aditya Yelikar et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Presently, percutaneous nephrolithotomy (PCNL) is preferred as a safe and effective way to remove large or multiple upper urinary tract calculi [1-7]. An increase in PCNL has been accompanied by variations in positions, techniques, and instruments and these may have led to increased complications [1, 2, 4, 5]. Following PCNL, 79.5% of patients may experience an uncomplicated postoperative period, although there are reports of an early complication rate of 50.8% [4, 5, 8].
Introduction
Presently, percutaneous nephrolithotomy (PCNL) is preferred as a safe and effective way to remove large or multiple upper urinary tract calculi [1-7]. An increase in PCNL has been accompanied by variations in positions, techniques, and instruments and these may have led to increased complications [1, 2, 4, 5]. Following PCNL, 79.5% of patients may experience an uncomplicated postoperative period, although there are reports of an early complication rate of 50.8% [4, 5, 8]. PCNL complications may occur during puncturing, access, or stone removal [4]. A standardized classification allows us to compare complications among different instruments, techniques, and centres [3, 4, 7, 9]. In 2004, the modified Clavien system (MC6) was introduced and allowed us to classify complications based on life-threatening conditions, interventions required, and disability [9]. In recent years, this classification has been used to report PCNL complications instead of using simply “minor” and “major” distinctions [3-8, 10-12]. In this study, we reported on the PCNL complications according to the 0&6 and identified the parameters affecting the severity of complications based on this classification.
Inclusion criteria and treatment protocol - Patients who were eligible for inclusion were all those who were candidates for percutaneous surgery as the primary indication or after failure of previous treatment. There were no specific exclusion criteria. All patients received IV antibiotic before surgery and for minimum 2 days post operatively. Initially patients were positioned in lithotomy position & a ureteric catheter was place retrogradely under fluoroscopy. Then patients were turned in prone position for pelvicalyceal system access. Access to the upper tract was guided by fluoroscopy after a RGP using air or non-ionic contrast. Once access was obtained, a guidewire was inserted and preferably manoeuvred toward the ureter. Dilation was performed with telescopic dilators and an Amplatz sheath was then positioned. The system was inspected by the rigid nephoscopy, and the stones were disintegrated by ballistic device or removed in toWR with graspers. The procedure was considered to have been completed when all removable stones had been taken out. Internal and/or external drain(s) were positioned according to the judgment of the surgeon. Post-operative complications were noted & graded according to the modified clavien grading system .Various pre & intra operative factors were compared against the clavien grading system to determine the most affecting factors.
Based on published literature, the relationship between Clavien score and the following patient characteristics and operative factors was analysed: age, sex, BMI, IHD status, diabetes status, Hypertension status, Chronic kidney disease status, History of previous stone surgery, stone surface area, stone distribution by Guy’s stone score, location of stone, access site, tract dilatation size ,surgery time, type of PCNL.
Patients were assigned to groups according to these variables. The mean Clavien score for each group and the intergroup difference in mean Clavien scores was calculated. We used the absolute difference in mean Clavien score as a proxy for the impact of each risk factor. Thus, a risk factor that is associated with a larger absolute change in mean Clavien score has more impact on actual Clavien scores, and thus a greater increase in risk of postoperative complications. Conversely, variables that impart a lower mean difference in mean Clavien score have less impact on the actual grading score and are less likely to increase the risk of complications. An example of the calculation performed is as follows. Assuming the mean Clavien score for patients with IHD was 1.5 while for those without IHD, it was 0.6. This gives an absolute difference in the mean Clavien score of 0.9; the relative increase in Clavien score from the presence of CVD was therefore
L H [
Observations
Table A: Patient Demographics (mean +/- SD)
|
Mean age(years) |
38.15+/-13.84 |
|
Mean BMI(kg/m2) |
21.87+/-2.11 |
|
Sex (male) n (%) |
461 (69.3%) |
|
Laterality |
|
|
Left |
329 (49.5%) |
|
Right |
336 (50.5%) |
|
Mean kidney size (cm) |
|
|
Length |
9.97+/-1.38 |
|
Width |
4.93+/-0.79 |
|
Previous history of stone surgery |
|
|
1) Yes |
38 |
|
2) No |
627 |
|
Mean stone size (mm) |
20.7+/-4.94 |
|
Mean stone enhancement (HU) |
1208.33+/-318.06 |
|
Mean stone surface area (mm2) |
319.59+/-238.36 |
|
Mean Guy’s stone score |
1.56+/-0.82 |
|
Mean access time (seconds) |
38.98+/-17.11 |
|
Mean fluoroscopy time (seconds) |
228.2+/-28.58 |
|
Mean total surgery time (mins) |
32.94+/-9.73 |
|
Mean tract size (Fr) |
21.67+/-1.52 |
|
No. Of tracts |
|
|
1) one |
615 (92.5%) |
|
2) two |
48 (7.2%) |
|
3) three |
2 (0.3%) |
|
Access |
|
|
1) Supra costal |
381 (57.3%) |
|
2) Infra costal |
284 (42.7%) |
|
Mean pre op Hb(mg/dl) |
12.13 |
|
Mean post op Hb(mg/dl) |
11.41 |
|
Mean % drop in Hb |
5.94% |
|
Mean pre op creat |
1.04 |
|
Mean post op creat |
1.05 |
|
% change in creat |
0.83% |
|
Mean pain score |
3.65+/-1.22 |
|
Mean hospital stay(hours) |
51.25+/-10.17 |
Table B: &RPSOLFDWLRQ 'HPRJUDSKLFV
|
Grade |
Complications |
Number % (n) |
|
None |
None |
334 (50.2%) |
|
1 |
Fever |
34 (5.11%) |
|
Transient rise in serum creatinine |
210 (31.6%) |
|
|
2 |
Blood transfusion |
9 (1.4%) |
|
Urine leakage < 12 hours |
51 (7.66%) |
|
|
UTI |
28 (4.21%) |
|
|
Wound infection |
Nil |
|
|
3a |
DJS placement for urine leakage > 24 hours |
Nil |
|
DJS placement for PUJ or pelvic injury |
Nil |
|
|
DJS migration |
Nil |
|
|
Urinoma formation |
Nil |
|
|
Retention due to clots |
Nil |
|
|
Pneumothorax |
Nil |
|
|
Perirenal hematoma |
3 (0.5%) |
|
|
3b |
Ureter or bladder stone |
Nil |
|
Calyx neck stricture |
Nil |
|
|
Secondary puj stenosis |
Nil |
|
|
Intraoperative bleeding leading to abandoning procedure |
4 (0.6%) |
|
|
Arterio-venous fistula |
Nil |
|
|
4a |
Neighbouring organ injury |
Nil |
|
Myocardial infarction |
Nil |
|
|
4b |
Urosepsis |
6 (0.9%) |
|
5 |
Death |
1 (0.2%) |
Table C: Comparison of operative characteristics & mean Clavien Dindo score
|
Patient characteristics |
n |
Mean Clavien dindo score +/-SD |
Absolute increase in Clavien score (Relative increase) |
p value |
|
|
Total patients 665 |
|
0.65+/-0.78 |
|
|
|
|
1. Age- |
|
|
|
|
|
|
32 |
0.63+/-0.49 |
|
0.0005 |
||
|
<15 |
|||||
|
15-35 |
261 |
0.48+/-0.71 |
|
|
|
|
36-55 |
309 |
0.63+/-0.76 |
|
|
|
|
56-75 |
63 |
1.43+/-0.85 |
0.8(126.98%) |
|
|
|
2. BMI- |
|
|
|
|
|
|
<18.5 |
24 |
0.83+/- 0.38 |
|
|
|
|
18.5-25 |
549 |
0.58+/- 0.74 |
|
|
|
|
26-30 |
92 |
0.99+/-1.01 |
0.41(70.68%) |
0.0005 |
|
3. DM- |
|
|
|
|
|
|
yes |
36 |
1.5+/-0.94 |
|
|
|
|
no Difference in mean score |
629 |
0.6+/-0.75 0.9 |
0.9 (150%) |
0.0005 |
|
|
4. HTN |
|
|
|
|
|
|
52 613 |
1.27+/-1.1 0.59+/-0.73 0.68 |
0.68(115.25%) |
0.0005 |
||
|
Yes No Difference in mean score |
|||||
|
5. IHD |
|
|
|
|
|
|
18 647 |
1.11+/-0.83 0.63+/-0.78 0.47 |
0.47(74.6%) |
0.011 |
||
|
Yes No Difference in mean score |
|||||
|
6. CKD |
|
|
|
|
|
|
Yes |
8 |
1.5+/-0.53 |
|
|
|
|
No Difference in mean score |
657 |
0.63+/-0.78 0.87 |
0.87(138.09%) |
0.002 |
|
|
7. Previous stone surgery |
|
|
|
|
|
|
Yes |
38 |
1+/-1.11 |
|
|
|
|
No Difference in mean score |
631 |
0.62+/-0.76 0.38 |
0.38 (61.29%) |
0.004 |
|
|
8. Stone surface area (mm2) |
|
|
|
|
|
|
>500 |
541 |
1+/-0.87 |
|
|
|
|
<500 Difference in mean score |
124 |
0.57+/-0.03 0.43 |
0.43(75.43%) |
0.0005 |
|
|
1. Location of stone |
|
|
|
|
|
|
Pelvis |
343 |
0.56 +/- 0.74 |
|
||
|
Single calyx |
120 |
0.69 +/- 0.88 |
|
||
|
Pelvis + single calyx |
115 |
0.62 +/- 0.68 |
|
||
|
Multiple calyces |
40 |
0.98 +/- 0.76 |
|
||
|
Partial staghorn |
19 |
0.68 +/- 0.74 |
|
||
|
Staghorn |
28 |
1.11 +/- 1.06 |
0.001 |
||
|
2. Guys stone score |
|
|
|
|
|
|
1 |
407 |
0.55 +/- 0.74 |
|
||
|
2 |
171 |
0.77 +/- 0.75 |
|
||
|
3 |
58 |
0.95 +/- 0.84 |
|
||
|
4 |
29 |
1.1 +/- 1.08 |
0.0005 |
||
|
3. Access site |
|
|
|
|
|
|
LP |
212 |
0.46+/-0.86 |
|
||
|
MP |
68 |
0.35+/-0.59 |
|
||
|
UP |
335 |
0.7+/-0.64 |
|
||
|
Multiple punctures |
50 |
1.5+/-0.95 |
0.005 |
||
|
4. Tract dilatation |
|
|
|
|
|
|
<20 |
13 |
0.4 +/- 0.67 |
|
||
|
20 |
214 |
0.44 +/- 0.69 |
|
||
|
22 |
315 |
0.69 +/- 0.77 |
|
||
|
24 |
125 |
0.85 +/- 0.92 |
0.0005 |
||
|
5. Surgery time |
|
|
|
|
|
|
<20 |
32 |
0 |
|
||
|
20-40 |
522 |
0.58+/-0.71 |
|
||
|
41-60 |
78 |
1.16+/-0.92 |
|
||
|
61-80 |
13 |
1.08+/-1.25 |
0.0005 |
||
|
6. Technique of pcnl |
|
|
|
|
|
|
Standard |
417 |
0.75 +/- 0.86 |
|
||
|
Tubeless |
166 |
0.37 +/- 0.53 |
|
||
|
Totally tubeless |
46 |
0.54 +/- 0.5 |
0.0005 |
Table D: Percentage of complications by Clavien (comparison with other studies) (table E)
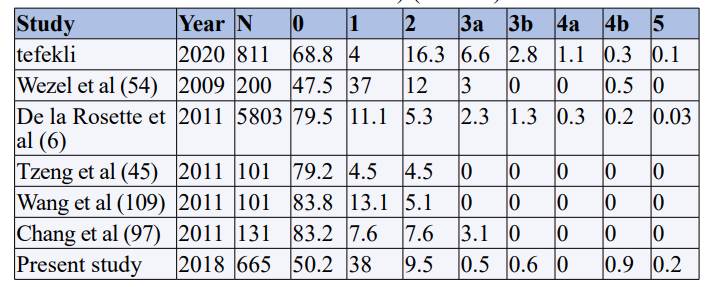
Table E: Percentage of selected complications
|
Study |
Year |
N |
Transfusion |
Hb drop |
Embolization |
Urinoma |
Fever |
Sepsis |
Thoracic |
Organ injury |
Death |
|
Wezel et al (54) |
2009 |
200 |
20 |
NA |
NA |
NA |
NA |
NA |
NA |
1 |
0 |
|
Resorlu et al (112) |
2010 |
192 |
5.6 |
1.6 |
0 |
NA |
5.6 |
0.5 |
1.1 |
0 |
0 |
|
Gupta et al (113) |
2009 |
90 |
4.4 |
2.1 |
0 |
NA |
15.6 |
NA |
3.3 |
0 |
0 |
|
De la Rosette et al (6) |
2011 |
5803 |
5.7 |
NA |
NA |
NA |
10.5 |
NA |
1.8 |
0 |
0 |
|
Semins et al |
2011 |
197 |
NA |
NA |
0 |
1 |
NA |
NA |
11.6 |
NA |
NA |
|
Present study |
2018 |
665 |
1.4 |
0.72 |
0 |
0 |
5.11 |
0.9 |
0 |
0 |
0.2
|
Statistical Analysis
The collected data were analysed with IBM.SPSS statistics software 23.0 Version .To describes about the data descriptive statistics frequency analysis, percentage analysis were used for categorical variables and the mean & S.D were used for continuous variables. To find the significant difference between the bivariate samples in Paired groups the Paired sample t-test was used & for Independent groups the unpaired sample t-test was used. For the multivariate analysis the one way ANOVA with Tukey’s Post-Hoc test was used. To find the significance in categorical data Chi-Square test was used. In all the above statistical tools the probability value .05 is considered as significant level.
Results
The demographic data of the study in shown in table A .There was significant increase in the number of complication as the age increased with minimum complications in the age group 16-35 years (37.4%) & maximum complications in the age group of 56-75 years (88.89%). There were significantly more complications in cases with BMI > 25 as compared to BMI <25 (65.22% vs 47.13%). Stone surface area was calculated by multiplying the longest length & width of the calculus (L×B) .The number of complications were more in cases where stone surface area was more than 500mm2 as compared to those with area <500mm2.
There were no complications in the group where surgery time was less than 20 mins as against 46.15% complications in cases with surgery time of >60 mins.
There was significant increase in the number of complications as the tract dilatation size increased (table B). There were least complications in the group with tract dilatation size of 20 Fr.
The number of complications was significantly higher in the group with co-morbidities like DM, HTN, IHD, and CKD.
The number of complications were least in the totally tubeless (no nephrostomy & Double J stent) group as compared to standard & tubeless PCNL groups.
There was significant increase in the number of complications in patients with history of previous stone surgery as compared to those with no history of stone surgery (21.1% vs 18.25).
The number of complications increased as the Guy’s stone score increased with least complications in Guy’s stone score 1 and maximum complications in Guy’s stone score 4.
As concerned with the access site there were least complications when the access was from middle calyx (29.42%) as against when it was from upper calyx (60.4%). The number of complications was obviously more when there were multiple punctures (82%).
The factors which did not affect the number of complications were sex, laterality & whether access is supra or infra costal. The mean clavien score in our study was 0.65+/-0.78.
The mean clavien score for various factors is shown in table D. The factors associated with an increase in the mean clavien score were age > 56 years ,history of previous stone surgery, DM, HTN, IHD, CKD, stone location (multiple calyces, partial staghorn & staghorn), Guy’s stone score > 1, access site (upper calyx & multiple access), tract dilatation of ≥ 22 Fr, surgery time of more than 40mins & standard technique of PCNL. The factors which did not affect the mean clavien score were sex, BMI, laterality.
As shown in table E the percentage of patients without any complications in our study was (50.2%) which was less as compared to other studies. This may be because we included transient elevation of serum creatinine as grade 1 complication which was not included in most of the other studies. However grade 3 and 4a complications were less in our study, whereas grade 4b complications were comparable to other studies (table E).
Comparing with results of other studies in literature (table F) the need for blood transfusion was very less (1.4%) in our study. The most common complication in other studies was fever whereas in our study the most common complication was transient elevation of serum creatinine (31.6%). In our study fever was reported in 5.11% of the cases. There was no case in our study with thoracic complications (hydro or pneumothorax). Others studies report no death, however there was one death in our study due to severe sepsis leading to acute renal failure & multi organ dysfunction.
Discussion
Postoperative complications directly impact patient quality of life, but there is currently no disease-specific quality of life instrument [13].
The CROES PCNL Global Study is the largest database of patients who were treated with PCNL to be reported to date [5]. The AUA guidelines (2017) recommend PCNL as first line therapy in symptomatic patients with renal stone size of ≥ 20mm (Grade B evidence). It also recommends that PCNL has a greater stone free rate & greater morbidity in lower pole stones > 10mm .Reporting a surgical outcome requires not only success rates, but also complication rates. Modified Clavien Dindo classification was used first time to classify pcnl complications by tefekli et al [10].
In their series of 811 PCNLs, Tefekli et al reported overall complications in 29.2% (vs. 50.2% in our study) [14]. Total complication rates after PCNL vary widely,with reported rates of between 29% and 83%.[14,15,16,17,18]. The high increased number of complications in our study was mainly because of the increased grade 1 complication (transient elevation of serum creatinine -31.6%,whereas other grades of complications were either similar or less in our study. Recently, de la Rosette et al collected prospective data from the Clinical Research Office of the Endourological Society (CROES) for 5,803 consecutive patients & showed the distribution of scores in the modified Clavien (grade table D) which we have compared with the distribution of complications in other studies including the present study. In their report, however, the number of specific complications in each grade was not provided.
While it is accepted that obesity generally places surgical patients at greater risk of complications, several studies indicate that complication rates after PCNL in obese patients are similar to those in non-obese patients and are independent of body mass index [19-21]. Assmy et al stratified 1121 PNL patients into four groups according to the World Health Organization classification of body mass index (BMI) [22]. The complication rate, need for auxiliary procedures, and hospital stay were not significantly different between BMI groups, where as in our study the number of complications were more in cases with BMI > 26 as compared to those with BMI <26 (65.21% vs 47.13%).
There was no significant difference in the complications with respect to sex. Tefekli et al found that success rates of PCNL were not significantly influenced by DM, HT, serum lipid abnormalities, obesity, or metabolic syndrome [24]. Major complications after PCNL have been reported to be at least 2.5 times more common in patients with diabetes mellitus [24]. In our study similarly complications in cases with DM were 94.59% whereas in cases with no co-morbidities complications were seen in 44.52%.
Unsal et al showed that the patients with CCI (Charlston comorbidity index) ≥ 2 had a 4.4767 times higher risk of medical complication compared with the patient with CCI ≤ 0 score (95% CI 2.1866-9.1655, P _.0001) [25].
Similarly in our study the absolute increase in mean clavien score in cases with HTN, IHD & CKD were 0.68, 0.47 & 0.87. However the PCNL global study by Labate et al showed that DM, IHD, age & BMI were not associated with an increased risk of severe or major complications [8].
Studies have shown that stone surface area or stone size significantly affected complications, mean Clavien score & surgery time [3, 26]. Similarly in our study when the stone size was more than 500 mm2 the relative increase in the complications was 75.43%.
Perhaps the most significant complication of PCNL, bleeding requiring transfusion has been reported to have an incidence as high as 23% [27, 28]. In the CROES study, transfusion was administered in 5.7% of patients [5]. In our study need for blood transfusion was very low (1.4%). Postoperative blood transfusion was done when hemoglobin dropped below 8 gm/dl. In a study by Stoller et al the incidence of extensive post-PCNL haemorrhage was 1% [27]. A similar study by Srivastava et al reported that 1.4% of patients required angiography or embolization for bleeding control [29]. They concluded that only stone size was a significant risk factor. In our study angiography/ embolization was not needed in any case.
Muslumanoglu et al observed bleeding in 39.1% and7.5% of patients managed with supracostal versus subcostal access, respectively (p< 0.01) [30]. In our study there was no significant difference in the number of complications between supracostal vs subcostal access. Studies report 3-7% risk of pleural injury in supra-costal punctures [31-33].
The major and most difficult step seems to be the ability to obtain appropriate access [8]. The mean access time in our study was 38.98+/-17.11 seconds.
Multiple access points significantly increased the bleeding risk, which was seen in 7.6% of patients with one access point versus 18.5% of cases with two or more access points ( p < 0.05) [32].
Netto and colleagues reported higher complication rates for multiple accesses versus upper pole and lower/middle calices accesses in staghorn stones [34]. Similarly in our study multiple access points lead to increased complications as compared to single access points (82% vs 47%).
Studies have shown fever accounted for 2.8-10.5% of complications [5, 14, and 35]. In our study fever was found in 5.11% of cases. They attributed such a low incidence of fever to the use of prophylactic antibiotics and the separate classification of other complications that may cause fever (i.e., blood transfusion, sepsis, etc.). In the CROES study fever of more than 38.5 degrees occurred in 10.5% of case [5]. In literature, fever is reported in up to 32% of cases after PCNL [35]. Both the AUA and EAU guidelines recommend antibiotic prophylaxis for all patients who are undergoing PCNL which was followed in our study [36, 37].
Another parameter that influences the complication rate is the reduction in operative time that comes with experience and specialization of the whole team.
An estimated 45–60 case is necessary to achieve competence in PCNL. This is based on three single surgeon studies [9-11]. Labate et al showed that patients whose operations lasted longer than 75 minutes (76-115 minutes) had statistically significant more severe postoperative complications (odds ratio 1.58) compared with those whose operative time was shorter than 50 minutes [8]. The mean operative time in our study was 32.94+/-9.73 mins. Similarly in our study complications increased when the operative time was more than 40 mins. The absolute & relative increase in the mean clavien score when the operative time was more than 40 mins was 0.54 & 93.1%.
Leakage periods >12 hours are reported to occur in 1.5–4.6% [38, 39]. We found a leakage of > 12 hours in 7.66% of cases.
Another meta-analysis study revealed no significant difference between tubeless and standard PCNL regarding complication rate [40]. In our study the absolute increase in the mean clavien score for standard PCNL was 0.75 compared to 0.37 for tubeless PCNL & 0.54 for totally tubeless PCNL which was statistically significant.
In a study by Labate et al Operative procedures were considered uneventful in4922 (85.5%) patients [8]. In other patients, complications included significant bleeding (7.8%), renal pelvis perforation (3.4%), hydrothorax (1.8%), and failure to complete the procedure in 99 cases. In our study the procedure was uneventful in 96.2%. In other patients there was significant bleeding in 0.6% and failure to complete procedure in 3.2%. In the same study in 4336 (75.7%) patients, the urologist confirmed that the patient had become stone free [8]. The stone-free rate was based on evaluation either by radiography or renal ultra sonography. In our study stone free rate after 1st procedure was 94.43% & after 2nd procedure was 95.93%. In the same study majority of patients did not receive any further treatment for renal stones ( 84.5%), whereas ureteroscopy, repeat PCNL, and SWL were performed in 1.4%, 6.9%, and6.2%, respectively [8]. In our study 2nd procedure (PCNL) was performed in 3.2% of cases. No patient in our study required ureteroscopy or SWL.
Duvdevani et al reported a major complication rate of 3.7% in very experienced centres, which is much lower than usually reported [7, 41]. The CROES PCNL study group reported major complications in 20%. In our study major complications occurred in 2.2%.
De la Rosette and Skolarikos et al have reported that the frequency of major complications after PCNL was 0.9% to 4.7% for septicaemia, 0.6% to 1.4% for renal haemorrhage necessitating intervention, 2.3% to 3.1% for pleural injury, and 0.2% to 0.8%for colonic injury [5, 18]. In our study septicaemia occurred in 0.9%, peri-renal haematoma occurred in 0.5%, pleural complications, adjacent organ or colonic injury did not occur in any case.
However, we admit that there are some weak points when using the modified Clavien grading System in classifying complications of PNL. First of all, it is not clear how to grade the presence of clinically significant or insignificant residual fragments because they cannot be defined as complications but rather as failures, increasing the morbidity. Therefore, we did not include them in the present classification. There are also controversies in grading auxiliary treatments, such as re-PCNL, SWL treatment, and ureteroscopy because they are not real complications but part of the stone management [27]. A total of 3.2% of patients in the present series underwent auxiliary treatments. Because re-PCNL and ureteroscopy required anaesthesia, they may be classified as grade 3b. Besides this, SWL treatment may be considered as a grade 3a complication because it is generally not done under anaesthesia.
Conclusion
Though PCNL is safe & has the best stone free rate among the available options for the treatment of renal calculi, surgeons must remember that serious complications may occur .The incidence of complications increases with risk factors like age > 55 , BMI > 25 , presence of co-morbidities (DM,HTN,CKD,IHD), history of previous stone surgery , increasing Guy’s stone score , stone surface area > 500mm2 , multiple punctures , tract dilatation size > 20 Fr & surgery time > 40mins . These factors should be considered while anticipating complications after PCNL.
References
- Mirheydar HS, Palazzi KL, Derweesh IH, Ithaar H Derweesh, David C Chang, et al. (2013) Percutaneous nephrolithotomy use is increasing in the United States: An analysis of trend sand complications. J Endourol 27: 979-983.
- Ghani KR, Sammon JD, Bhojani N, Karakiewicz PI, Sun M, et al. (2013) Trends in percutaneous nephrolithotomy use and outcomes in the United States. J Urol 190: 558-564.
- de la Rosette JJ, Zuazu JR, Tsakiris P, Elsakka AM, Zudaire JJ, et al. (2008) Prognostic factors and percutaneous nephrolithotomy morbidity: A multivariate analysis of a contemporary series using the Clavien classification. J Urol 180: 2489-2493.
- Michel MS, Trojan L, Rassweiler JJ (2007) Complications in percutaneous nephrolithotomy. Eur Urol 51: 899-906.
- De la Rosette J, Assimos D, Desai M, Gutierrez J, Lingeman J, et al. (2011) The Clinical Research Office of the Endourological Society Percutaneous Nephrolithotomy Global Study: Indications, complications, and outcomes in 5803 patients. J Endourol 25: 11-17.
- Shin TS, Cho HJ, Hong SH, Ji Youl Lee, Sae Woong Kim, et al. (2011) Complications of percutaneous nephrolithotomy classified by the modified Clavien grading system: A single center’sexperience over 6years. Korean J Urol 52: 769-775.
- Seitz C, Desai M, Häcker A, Hakenberg OW, Liatsikos E, et al. (2012) Incidence, prevention, and management of complications following percutaneous nephrolitholapaxy. Eur Urol 61: 146-158.
- Labate G, Modi P, Timoney A, Luigi Cormio, Xiaochun Zhang, et al. (2011) The percutaneous nephrolithotomy global study: Classification of complications. J Endourol 25: 1275-1280.
- Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240: 205-213.
- Tefekli A, Ali Karadag M, Tepeler K, Sari E, Berberoglu Y, et al. (2008) Classification of percutaneous nephrolithotomy complications using the modified Clavien grading system: Looking for a standard. Eur Urol 53: 184-190.
- Morgan M, Smith N, Thomas K (2009) Is Clavien the new standard for reporting urological complications? BJU Int 104: 434-436.
- De la Rosette JJ, Opondo D, Daels FP, Giusti G, Serrano A, et al. (2012) Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy. EurUrol 62: 246-255.
- Keeley FX, Assimos DG (2009) Clinical trials of the surgicalmanagement of urolithiasis: Current status and futureneeds. Adv Chronic Kidney Dis 16: 65-69.
- Tefekli A, Ali Karadag M, Tepeler K, Sari E, Berberoglu Y, et al. (2008) Classification of percutaneous nephrolithotomy complications using the modified Clavien grading system: looking for a standard. EurUrol 53: 184-190.
- Osman M, Wendt-Nordahl G, Heger K, Michel MS, Alken P, et al. (2005) Percutaneous nephrolithotomy with ultrasonography-guided renal access: Experience from over 300 cases. BJU Int 96: 875-878.
- Michel MS, Trojan L, Rassweiler JJ (2007) Complications in percutaneous nephrolithotomy. Eur Urol 51: 899-906.
- Turna B, Nazli O, Demiryoguran S, Mammadov R, Cal C, et al. (2007) Percutaneous nephrolithotomy: Variables that influence hemorrhage. Urology 69: 603-607.
- Skolarikos A, de la Rosette J (2008) Prevention and treatment of complications following percutaneous nephrolithotomy. Current Opinion in Urology18: 229-234.
- Sergeyev I, Koi PT, Jacobs SL, Godelman A, Hoenig DM, et al. (2007) Outcome of percutaneous surgery stratified according to body mass index and kidney stone size. Surg Laparosc Endosc Percutan Tech 17: 179-183.
- El-Assmy AM, Shokeir AA, El-Nahas AR, Shoma AM, Eraky I, et al. (2007) Outcome of percutaneous nephrolithotomy: Effect of body mass index. Eur Urol 52: 199-204.
- Tomaszewski JJ, Smaldone MC, Schuster T, Jackman SV, Averch TD, et al. (2010) Out comes of percutaneous nephrolithotomy stratified by body mass index. J Endourol 24: 547-550.
- El-Assmy AM, Shokeir AA, Mohsen T, El-Tabey N, El-Nahas AR, et al. (2007) Renal access by urologist or radiologist for percutaneous nephrolithotomy-is it still an issue? J Urol 178: 916-920.
- Tiselius HG, Ackermann D, Alken P, Buck C, Conort P, et al. (2001) Guidelines on urolithiasis. EurUrol 40: 362-371.
- Tefekli A, Kurtoglu H, Tepeler K, Karadag MA, Kandirali E, et al. (2008) Does the metabolic syndrome or its components affect the outcome of percutaneous nephrolithotomy? J Endourol 22: 35-40.
- Unsal A, Resorlu B, Atmaca AF, Akif Diri A, Goktug HN, et al. (2012) Prediction of morbidity and mortality after percutaneous nephrolithotomy by using the Charlson Comorbidity Index. Urology 79: 55-60.
- Akman T, Binbay M, Akcay M, Tekinarslan E, Kezer C, et al. (2011) Variables that influence operative time during percutaneous nephrolithotomy: An analysis of 1897 cases. J Endourol 25:1269-1273.
- Stoller ML, Wolf JS, St Lezin MA (1994) Estimated blood loss and transfusion rates associated with percutaneous nephrolithotomy. J Urol 152: 1977-198.
- El-Nahas AR, Shokeir AA, El-Assmy AM, Mohsen T, Shoma AM, et al. (2007) Post-percutaneous nephrolithotomy extensive hemorrhage: a study of risk factors. J Urol 177: 576-579.
- Srivastava A, Singh KJ, Suri A, Dubey D, Kumar A, et al. (2005) Vascular complications after percutaneous nephrolithotomy: are there any predictive factors? Urology 66:38-40.
- Muslumanoglu AY, Tefekli A, Karadag MA, Tok A, Sari E, et al. (2006) Impact of percutaneous access point number and location on complication and success rates in percutaneous nephrolithotomy. Urol Int 77: 340-346.
- Raza A, Moussa S, Smith G, Tolley DA (2008) Upper-pole puncture in percutaneous nephrolithotomy: A retrospective review of treatment safety and efficacy. BJU Int 101: 599-602.
- Aron M, Yadav R, Goel R, Kolla SB, Gautam G, et al. (2005) Multi-Tract Percutaneous Nephrolithotomy for Large Complete Staghorn Calculi. Urol Int 75: 327-332.
- Gupta R, Kumar A, Kapoor R, Srivastava A, Mandhani A, et al. (2002) Prospective evaluation of safety and efficacy of the supracostal approach for percutaneous nephrolithotomy. BJU Int 90: 809-813.
- Netto NR, Ikonomidis J, Ikari O, Claro JA (2005) Comparative study of percutaneous access for staghorn calculi. Urology 65:659-662.
- Dogan HS, Sahin A, Cetinkaya Y, Akdogan B, Ozden E, et al. (2002) Antibiotic prophylaxis in percutaneous nephrolithotomy: Prospective study in 81 patients. J Endourol 16: 649-653.
- Wolf JS, Bennett CJ, Dmochowski RR, Hollenbeck BK, Pearle MS, et al. (2008) Urologic Surgery Antimicrobial Prophylaxis Best Practice Policy Panel. Best practice policy statement on urologic surgery antimicrobial prophylaxis. J Urol 179: 1379-1390.
- Grabe M, Bishop MC, Bjerklund-Johansen TE, Botto H, Cek M, et al. (2009) Guidelines on Urological Infections. European Guidelines Office 2009.
- Tefekli A, Altunrende F, Tepeler K, Tas A, Aydin S, et al. (2007) Tubeless percutaneous nephrolithotomy in selected patients: a prospective randomized comparison. Int Urol Nephrol 39:57-63.
- Liatsikos EN, Kapoor R, Lee B, Jabbour M, Barbalias G, et al. (2005) ‘‘Angular percutaneous renal access’’. Multiple tracts through a single incision for staghorn calculus treatment in a single session. Eur Urol 48: 832-837.
- Ni S, Qiyin C, Tao W, Hailong Hu, Chunyang Wang, et al. (2011) Tubeless percutaneous nephrolithotomy is associated with less pain and shorter hospitalization compared with standard or small bore drainage: A meta-analysis of randomized, controlled trials. Urology 77: 1293-1298.
- Duvdevani M, Nott L, Ray AA, Ko R, Denstedt JD, et al. (2009) Percutaneous nephrolithotripsy in patients with diabetes mellitus. J Endourol 23: 21-26.