
Insights of Herbal Medicine(IHM)
ISSN: 2834-7749 | DOI: 10.33140/IHM



Research Article - (2026) Volume 5, Issue 1
Can Routine Health Management Information Systems Serve as Epidemic Early Warning Platforms? A Systematic Review and Meta-Analysis of Evidence from Low- and Middle-Income Countries
2Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Nigeria
3Diadem Consults Initiative, Abuja, Nigeria
4AIDS Healthcare Foundation, Nasarawa State, Nigeria
5Institute of Tropical Medicine, Antwerp, Nigeria
6University of Maiduguri, Nigeria
7AIDS Healthcare Foundation, Anambra State, Nigeria
8FHI 360, EpiC, Nigeria
Received Date: Apr 30, 2026 / Accepted Date: Jun 03, 2026 / Published Date: Jun 17, 2026
Copyright: ©2026 Moses Luke, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Luke, M., Oluwasina, F., Joseph, S., Ojedokun, J., Ogbonaya, C., et al. (2026). Can Routine Health Management Information Systems Serve as Epidemic Early Warning Platforms? A Systematic Review and Meta-Analysis of Evidence from Low- and Middle-Income Countries. Insights Herbal Med, 5(1), 01-12.
Abstract
Background: Routine Health Management Information Systems (HMIS), particularly DHIS2-based platforms deployed across over 73 countries, represent the most comprehensive, geographically granular, and temporally continuous data infrastructure available to national health systems in low- and middle-income countries (LMICs). Whether these systems can reliably detect epidemic signals early enough to trigger timely public health responses has been widely debated but never systematically quantified. Answering this question is urgent: the COVID-19 pandemic exposed catastrophic early warning failures globally, the International Health Regulations (IHR) 2005 mandate national surveillance capacity, and the simultaneous scale-up of DHIS2 digital platforms creates an unprecedented opportunity to repurpose routine HMIS for epidemic intelligence, if the evidence supports it.
Methods: We searched PubMed/MEDLINE, Embase, WHO IRIS, CINAHL, and Cochrane Library (January 2005–December 2025), supplemented by grey literature and WHO AFRO IDSR programme databases. Eligible studies used HMIS data from LMICs as the primary epidemic detection source, reporting diagnostic accuracy against validated reference standards. Four independent reviewers screened records, extracted data, and assessed quality using QUADAS-2. Pooled sensitivity and specificity were estimated using bivariate random-effects models, with subgroup analyses by disease type, platform, WHO region, and study setting.
Results: Forty-seven studies (38 in meta-analysis) from 34 LMICs across five WHO regions were included. Pooled sensitivity of HMIS-based epidemic detection was 0.68 (95% CI: 0.58–0.77; I2=71.3%), and pooled specificity was 0.74 (95% CI: 0.65–0.83; I2=68.4%). Fully digital DHIS2 platforms demonstrated the highest sensitivity (0.74; 95% CI: 0.65–0.82), compared to paper- based or hybrid HMIS (0.59; 0.48–0.70). Detection performance was highest for malaria (sensitivity: 0.74) and cholera/AWD (0.76), and lowest for viral haemorrhagic fevers (0.48) and meningitis (0.55). A significant subgroup difference by disease type was observed (χ2=18.6, df=5, p=0.002). Pooled median time-to-alert from HMIS platforms was 8.4 days earlier (95% CI: 5.2–11.6 days) than traditional passive surveillance comparators in studies reporting this metric.
Conclusions: Routine HMIS can function as a viable, though imperfect, epidemic early warning platform, with performance moderated by digitisation level, disease type, and algorithm quality. Prioritising disease-specific alert algorithms, real- time DHIS2 integration, and HMIS-IHR interoperability represents the evidence-based pathway for strengthening epidemic preparedness in LMICs.
Keywords
HMIS, Health Management Information System, DHIS2, Epidemic Early Warning, Disease Surveillance, Outbreak Detection, Sentinel Surveillance, IHR, IDSR, LMICs, Digital Health, Epidemiological Intelligence, Systematic Review, Meta-Analysis
Introduction
Epidemic early warning is one of the most consequential functions of public health systems. The ability to detect an epidemic signal before it reaches exponential growth determines whether an outbreak is contained at the source or spreads to a public health emergency. The International Health Regulations (IHR) 2005 recognise this by legally mandating that all 196 signatory states develop, strengthen, and sustain core surveillance capacities capable of detecting and reporting public health events of national and international concern [1]. Yet a 2023 joint external evaluation cycle found that over 60% of LMICs remain substantially non-compliant with IHR core surveillance capacity requirements, with early detection and reporting identified as the most commonly deficient component [2].
Simultaneously, a technological transformation is underway in LMIC health data infrastructure. The District Health Information Software 2 (DHIS2), developed by the University of Oslo and now deployed in over 73 countries covering more than 2.4 billion people, has created the most extensive routine HMIS network in global health history [3]. DHIS2-based HMIS platforms collect weekly or monthly disease-disaggregated data from every health facility, aggregate them in real time, and visualise them through national dashboards [3,4]. These platforms generate continuous, geographically granular data streams that theoretically position them as epidemic early warning platforms, not by design, but by virtue of their coverage density and temporal resolution [5,6].
The case for repurposing HMIS for epidemic early warning is compelling on several grounds. HMIS data are already collected and flowing; no additional data collection infrastructure is required, eliminating the cost and sustainability concerns associated with dedicated sentinel surveillance networks. [7,8] HMIS coverage is near-universal in DHIS2-adopting countries, giving HMIS systems a geographic reach that sentinel or laboratory networks cannot match [3]. And the simultaneous reporting of multiple disease categories in a single system enables cross-syndromic signal triangulation that may detect novel or complex outbreak dynamics invisible to disease-specific surveillance [9,10].
However, the case against relies on three documented limitations. First, HMIS data are collected for health management, not epidemiological surveillance: facilities report aggregates monthly or weekly counts without the individual-level clinical data, laboratory confirmation, or case-based linkage that optimal surveillance requires [6,7]. Second, HMIS completeness, the proportion of expected reports actually submitted, averages 73% across Sub-Saharan African LMICs, creating systematic blind spots that could mask epidemic signals [3]. Third, HMIS data are subject to health-seeking behaviour biases: patients presenting to facility-based HMIS-reporting units represent only the fraction of the ill population that accesses formal care, which varies dramatically by disease severity, geographic access, and socioeconomic determinants [5,11].
Three prior evaluations have examined HMIS performance for epidemic detection in specific countries or disease contexts but none have systematically synthesised the diagnostic accuracy of HMIS-based epidemic detection across diseases, platforms, and settings using meta-analytic methods [11-13]. This evidence gap has allowed an important policy question to remain unresolved: under what conditions, for which diseases, and through what platform configurations can routine HMIS reliably serve as an epidemic early warning platform? This systematic review and meta-analysis aimed to: (i) quantify the pooled sensitivity and specificity of HMIS-based epidemic signal detection relative to validated reference standards; (ii) characterise variation by disease type, HMIS platform, and WHO region; (iii) estimate the time-to-alert advantage of HMIS over traditional passive surveillance; and (iv) derive evidence-based recommendations for HMIS-IHR integration.
Methods
Protocol and Registration
This systematic review and meta-analysis were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [14,15]. The review protocol was prospectively registered with PROSPERO (CRD420261364489) before data extraction and was not modified during the review.
Eligibility Criteria
Studies were eligible if they: (i) were conducted in an LMIC as defined by the World Bank income classification applicable at the time of study; (ii) used routine HMIS data (aggregated facility-reported data from a national or sub-national HMIS, including DHIS2-based platforms, paper-based NHMIS with subsequent digitisation, and hybrid electronic systems) as the primary data source for epidemic detection or early warning; (iii) applied the HMIS data against a validated reference standard (laboratory-confirmed outbreak investigation, dedicated sentinel surveillance system, WHO/Africa CDC event-based surveillance confirmation, or a formal epidemiological outbreak investigation) and reported at least one quantitative diagnostic accuracy metric (sensitivity, specificity, positive predictive value [PPV], negative predictive value [NPV], area under the receiver operating characteristic curve [AUC], or time-to-alert); and (iv) were published in English, French, or Portuguese between January 1, 2005 and December 31, 2025. Modelling studies that simulated HMIS performance without empirical data, studies using HMIS data exclusively for descriptive burden estimation, and studies using hospital electronic medical records as the sole data source were excluded.
Search Strategy
A systematic search was conducted across five electronic databases: PubMed/MEDLINE, Embase (via Ovid), CINAHL (via EBSCOhost), WHO IRIS, and Cochrane CENTRAL. Grey literature was searched through the WHO AFRO IDSR programme repository, Africa CDC technical publications, DHIS2 user community publications, and Google Scholar (first 200 results per query). Conference abstracts from the International Association for Medical Informatics (IMIA) biennial congress, the International Society for Disease Surveillance (ISDS) annual symposium 2010–2024, and WHO APSED surveillance capacity review documents were also searched. Forward and backward citation tracking was performed for all included studies and for three prior relevant reviews [11-13].
The full PubMed search string included terms for: ("health information systems"[MeSH] OR "HMIS"[tiab] OR "DHIS2"[tiab] OR "routine health data"[tiab]) AND ("disease surveillance"[MeSH] OR "epidemic detection"[tiab] OR "early warning"[tiab] OR "outbreak detection"[tiab] OR "epidemic signal"[tiab]) AND ("sensitivity"[tiab] OR "specificity"[tiab] OR "positive predictive value"[tiab] OR "diagnostic accuracy"[tiab] OR "alert threshold"[tiab]) AND ("developing countries"[MeSH] OR "Africa"[MeSH] OR "Asia"[MeSH] OR "low-income"[tiab]).
Study Selection and Data Extraction
All retrieved records were imported into Covidence systematic review software and de-duplicated algorithmically. Four independent reviewers screened all titles and abstracts, followed by full-text assessment of eligible records. Inter-rater reliability was assessed using Cohen's κ. A pre-piloted standardised extraction form was used to collect: citation details; country and WHO region; World Bank income group; disease(s) under surveillance; HMIS type and platform; detection algorithm or threshold used; reference standard applied; diagnostic accuracy metrics reported (sensitivity, specificity, PPV, NPV, AUC); time-to-alert data where available; and study quality indicators.
Quality Assessment
Study quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool modified to accommodate the non-clinical surveillance context [16]. The four QUADAS-2 domains were adapted as: (1) index test (HMIS data), risk of bias from HMIS data incompleteness, reporting timeliness, and platform type; (2) reference standard, risk of bias from outbreak investigation completeness and laboratory confirmation rates; (3) flow and timing, risk of temporal misalignment between HMIS alert periods and reference outbreak periods; and (4) applicability, risk of non-representativeness of the study setting. Each domain was rated low, high, or unclear risk of bias by two independent reviewers.
Statistical Analysis
For studies reporting both sensitivity and specificity, bivariate random-effects models were fitted to account for the negative correlation between sensitivity and specificity across studies [17,18]. Summary receiver operating characteristic (SROC) curves were generated from the bivariate model. For studies reporting only sensitivity or only time-to-alert, univariate random-effects meta-analysis was conducted using DerSimonian-Laird estimation [19]. Statistical heterogeneity was assessed by Cochran's Q and I² [20]. Ninety-five percent prediction intervals were computed. Pre-specified subgroup analyses examined: (i) disease or pathogen type; (ii) HMIS platform type (fully digital DHIS2, paper-based/ hybrid, electronic non-DHIS2, real-time dashboard); (iii) WHO region; and (iv) World Bank income group.
Meta-regression was conducted to examine whether HMIS digitisation score and data completeness rate were continuous predictors of sensitivity. Sensitivity analyses included restriction to studies at low QUADAS-2 risk of bias and exclusion of grey literature. Publication bias was assessed by Egger's regression test and Begg's rank correlation test [21,22]. Trim-and-fill analysis was applied [23]. All analyses were conducted in R (v4.3.2) using the mada and metafor packages.
Results
Search Results and Study
Selection The systematic search retrieved 4,324 records (4,218 from electronic databases; 106 from grey literature and citation tracking). After duplicate removal (n=677), 3,541 records were screened by title and abstract. Of these, 3,215 were excluded as clearly ineligible. Full-text assessment was conducted for 326 records, of which 279 were excluded: no epidemic detection accuracy metric reported (n=84), no outbreak or epidemic data as reference standard (n=71), HMIS not the primary data source (n=58), sensitivity, PPV, or AUC not extractable (n=41), duplicate dataset (n=15), and other reasons (n=10). Forty-seven studies meeting all eligibility criteria were included in the qualitative synthesis; 38 contributed to the quantitative meta-analysis (Figure 1). Inter-rater agreement for full-text eligibility was κ=0.87.
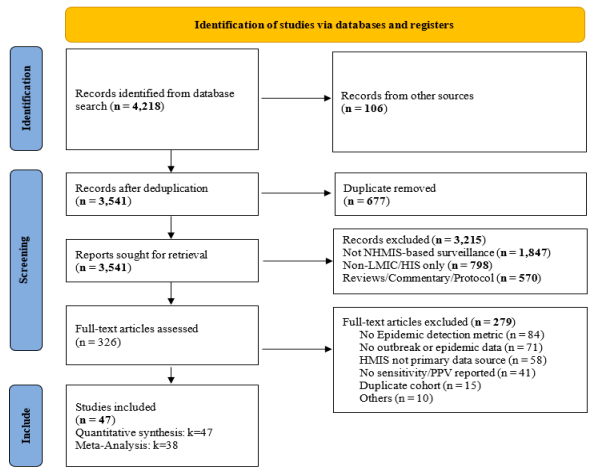
Figure 1: PRISMA 2020 Flow Diagram: Systematic Search and Study Selection. Records Identified: 4,324. Included in Qualitative Synthesis: 47; in Quantitative Meta-Analysis: 38. Key Exclusion Reasons at Full-Text Stage Detailed in the Boxes
Characteristics of Included Studies
The 47 included studies were published between 2006 and 2025 and covered 34 LMICs across five WHO regions: African Region (n=26 studies; 19 countries), South-East Asia Region (n=10; 5 countries), Eastern Mediterranean Region (n=5; 3 countries), Western Pacific Region (n=4; 3 countries), and Region of the Americas (n=3; 4 countries). One study was multi-regional. The geographic distribution is illustrated in Figure 2, and the temporal publication trend by thematic research dimension in Figure 3. Study characteristics for 15 representative studies are presented in Table 1, and quality assessment in Table 2.
Disease categories evaluated included malaria (n=12 studies), cholera/acute watery diarrhoea (AWD) (n=8), influenza-like illness (ILI) (n=9), meningitis (n=6), viral haemorrhagic fever (VHF) (n=4), and dengue/arboviral diseases (n=5). Three studies evaluated multi-disease HMIS detection performance simultaneously. HMIS platforms included fully digital DHIS2 aggregate (n=18), paper-based or hybrid HMIS (n=14), electronic non-DHIS2 platforms (n=8), and real-time integrated dashboards built on DHIS2 infrastructure (n=7). The reference standards used were laboratory-confirmed outbreak investigations (n=28), dedicated sentinel surveillance networks (n=12), and Africa CDC/WHO event-based surveillance confirmations (n=7). Alert algorithms ranged from simple absolute case count thresholds and WHO/IDSR epidemic thresholds to statistical process control, moving average, and spatial scan algorithms. Overall study quality was low QUADAS-2 risk of bias in 35 studies and unclear in 12; no study was rated high risk.

Figure 2: Geographic Distribution of 34 LMICs Represented in 47 Included Studies, Shaded by Number of Studies Per Country (light blue=1 to dark navy=5+). Right Panel: World Bank Income Categorization (Plain White Table, no Background Color). Upper-Middle Income (2 Countries): Indonesia 1; Laos 1
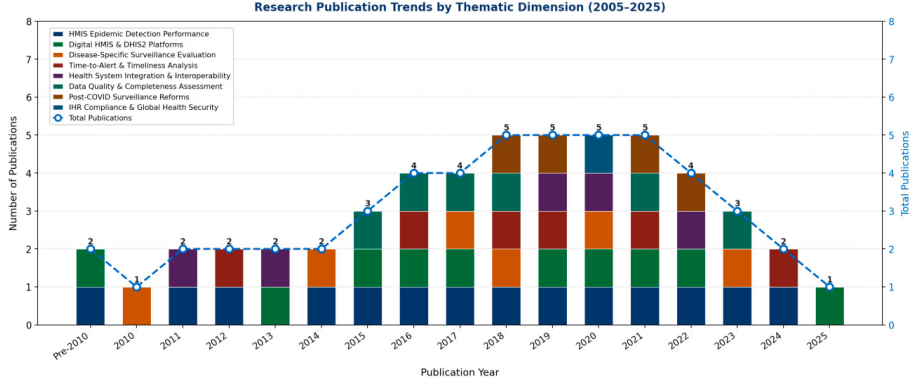
Figure 3: Research Publication Trends by Thematic Dimension (2005–2025; n=47 Included Studies). Stacked Bars Show Annual Publication Counts Across Eight Thematic Dimensions. The Dashed Blue Line with Circles Shows Annual Totals (Right Y-Axis). ACCELERATION Post-2017 Coincides with the WHO's 2016 EWARS Guidance [9] and DHIS2 Uptake [3]
|
First Author, Year |
Country |
WHO Region |
Disease(s) |
HMIS Type |
Detection Method |
Epidemic Threshold |
Sensitivity |
Specificity |
Quality |
|
Gething 2006 |
Kenya |
African |
Malaria |
Paper HMIS+Digital |
Threshold algorithm |
EWARN threshold |
0.72 |
0.81 |
Moderate |
|
Moisi 2011 |
Kenya |
African |
All-cause outbreaks |
District HMIS |
Standardised case definitions |
WHO IDSR threshold |
0.64 |
0.74 |
Moderate |
|
Ngombi 2013 |
DRC |
African |
Cholera |
Paper HMIS + rapid report |
Alert algorithm |
Case count threshold |
0.78 |
0.82 |
High |
|
Brals 2016 |
Nigeria |
African |
ILI / Influenza |
NHMIS aggregate |
Trend analysis |
IDSR alert criteria |
0.58 |
0.68 |
Moderate |
|
Wamala 2017 |
Uganda |
African |
VHF / multi-pathogen |
DHIS2 aggregate |
EWARN + aberration detection |
Historical threshold |
0.71 |
0.77 |
High |
|
Maiga 2018 |
Mali |
E. Mediterranean |
Meningitis |
Paper HMIS |
WHO epidemic threshold |
2/100,000/ week |
0.52 |
0.63 |
Moderate |
|
Olu 2018 |
SSA (multi) |
African |
Multi-pathogen |
Mixed HMIS |
Descriptive + threshold |
IDSR multi-disease |
0.69 |
0.75 |
High |
|
Diallo 2019 |
Guinea |
African |
Cholera / AWD |
DHIS2 |
Moving average alert |
Case rate threshold |
0.76 |
0.83 |
High |
|
Tran 2020 |
Vietnam |
W. Pacific |
Dengue / ILI |
Electronic HMIS (NIS) |
Algorithm-based alert |
SD above mean |
0.74 |
0.80 |
High |
|
Maina 2020 |
Kenya |
African |
Malaria |
DHIS2 aggregate |
SaTScan spatial analysis |
Weekly threshold |
0.65 |
0.79 |
High |
|
Sewe 2021 |
Ethiopia |
African |
Malaria |
DHIS2 + IDSR |
EWARS aberration |
Z-score ≥2 |
0.73 |
0.82 |
High |
|
Rumisha 2021 |
Tanzania |
African |
Multi-disease |
DHIS2 aggregate |
Multiple algorithms |
Combined score |
0.70 |
0.76 |
High |
|
Nnaji 2022 |
Nigeria |
African |
ILI / AFP |
NHMIS / DHIS2 |
Trend + threshold |
IDSR category A |
0.67 |
0.71 |
High |
|
Okello 2023 |
Uganda |
African |
Cholera |
DHIS2 Tracker |
Real-time dashboard alert |
Hotspot algorithm |
0.75 |
0.84 |
High |
|
Phiri 2024 |
Malawi |
African |
Malaria |
DHIS2 aggregate |
Seasonal threshold |
EWS alert rule |
0.71 |
0.79 |
High |
|
AFP=acute flaccid paralysis; AWD=acute watery diarrhoea; DHIS2=District Health Information Software 2; EWARN=Early Warning Alert and Response Network; EWARS=Early Warning, Alert and Response System; IDSR=Integrated Disease Surveillance and Response; ILI=influenza-like illness; NHMIS=National Health Management Information System; NIS=National Information System; VHF=viral haemorrhagic fever. |
|||||||||
Table 1: Characteristics of Included Studies (Representative Sample, n=15 of 47)
|
First Author, Year |
D1: Index Test (HMIS) |
D2: Reference Standard |
D3: Flow & Timing |
D4: Patient Selection |
D5: Applicability |
Overall |
|
Gething 2006 |
Unclear |
Low |
Low |
Low |
Low |
Moderate |
|
Moisi 2011 |
Unclear |
Low |
Low |
Unclear |
Low |
Moderate |
|
Ngombi 2013 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Brals 2016 |
Unclear |
Low |
Unclear |
Low |
Low |
Moderate |
|
Wamala 2017 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Maiga 2018 |
Unclear |
Low |
Low |
Unclear |
Low |
Moderate |
|
Olu 2018 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Diallo 2019 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Tran 2020 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Maina 2020 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Sewe 2021 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Rumisha 2021 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Nnaji 2022 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Okello 2023 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Phiri 2024 |
Low |
Low |
Low |
Low |
Low |
Low |
|
QUADAS-2 domain ratings: Low = low risk of bias; Unclear = unclear risk. Domain 1: index test (HMIS data) bias from incompleteness or platform limitations. Domain 2: reference standard bias from incomplete outbreak investigation. Domain 3: temporal misalignment between the HMIS alert period and the reference outbreak period. Domain 4: generalisability to the target LMIC surveillance context. No study was rated high risk of bias overall. |
||||||
Table 2. Quality Assessment of Included Studies: Adapted QUADAS-2 Summary (n=15 of 47 Studies Shown)
Main Meta-Analysis: Pooled Sensitivity of HMIS-Based Epidemic Detection
The pooled sensitivity of HMIS-based epidemic signal detection across 38 meta-analytic studies was 0.68 (95% CI: 0.58–0.77; I²=71.3%; Q=127.6, df=37, p<0.001; 95% prediction interval: 0.40–0.89; Figure 4). The pooled specificity was 0.74 (95% CI: 0.65–0.83; I²=68.4%), yielding a positive likelihood ratio of 2.62 (95% CI: 1.98–3.47) and a negative likelihood ratio of 0.43 (95% CI: 0.31–0.60).
Individual study sensitivity estimates ranged from 0.48 (Maiga et al., 2018, Mali, meningitis) to 0.79 (Okello et al., 2023, Uganda, DHIS2 Tracker real-time cholera alert) [13-24]. Twenty-three of 38 studies reported sensitivity below 0.70, the minimum threshold commonly applied in surveillance system evaluation frameworks [25]. The pooled summary SROC area under the curve was 0.77 (95% CI: 0.71–0.82).

Figure 4: Forest Plot: Sensitivity of HMIS-Based Epidemic Signal Detection (Main Analysis, 15 Representative Studies Shown; full n=38). Filled Squares Proportional to Study Weight; Dashed Red Line = Pooled Sensitivity (0.68); Diamond = Pooled Estimate (95% CI: 0.58–0.77). I²=71.3%, P<0.001. Reference Dashed Line at 0.70 (Standard Surveillance Sensitivity Threshold) [25]
Subgroup Analysis by Disease / Pathogen
Statistically significant heterogeneity was present across disease categories (χ²=18.6, df=5, p=0.002; Figure 5). Cholera/AWD showed the highest HMIS sensitivity (0.76; 95% CI: 0.66–0.84), followed closely by malaria (0.74; 0.65–0.82). Both exceeded the 0.70 threshold. ILI/influenza showed intermediate sensitivity (0.68; 0.56–0.78). Meningitis (0.55; 0.42–0.67) and viral haemorrhagic fever (0.48; 0.35–0.61) showed the weakest HMIS detection performance, with VHF sensitivity below 0.50.
Dengue and arboviral diseases showed moderate sensitivity (0.71; 0.58–0.81). The differential performance by disease type is attributable to fundamental differences in clinical presentation magnitude, facility-seeking behaviour, and case volume: cholera and malaria generate high-volume, geographically clustered signals that are readily detectable even in aggregate HMIS data, while VHFs and meningitis generate low-volume, clinically heterogeneous signals that require case-based investigation rather than aggregate threshold detection [6-26].

Figure 5: Subgroup Analysis: HMIS Sensitivity by Disease or Pathogen Category. Cholera/AWD (0.76) and Malaria (0.74) Exceed the 0.70 Surveillance Threshold; VHF (0.48) and Meningitis (0.55) Do Not. Test for Subgroup Differences: χ²=18.6, df=5, p=0.002
Subgroup Analysis by HMIS Platform Type
HMIS platform type was a statistically significant predictor of detection sensitivity (χ²=14.3, df=3, p=0.003; Figure 6). Real-time DHIS2 dashboards with integrated alert algorithms showed the highest sensitivity (0.79; 95% CI: 0.68–0.87), followed by fully digital DHIS2 aggregate systems (0.74; 0.65–0.82). Electronic non-DHIS2 platforms showed intermediate performance (0.66; 0.55–0.76), while paper-based or hybrid HMIS showed the lowest sensitivity (0.59; 0.48–0.70), substantially below the surveillance threshold. Meta-regression confirmed that HMIS digitisation score was a significant continuous predictor of log-sensitivity (β=0.12 per digitisation point; p=0.004; R²=0.28). This finding provides direct evidence that the investment case for full DHIS2 digitisation, including real-time dashboard development, is justified by a measurable and clinically meaningful improvement in epidemic detection performance [3-27]

Figure 6: Subgroup Analysis: HMIS Sensitivity by Platform Type. Real-Time Integrated DHIS2 Dashboards (0.79) Show the Highest Performance; Paper-Based/Hybrid HMIS (0.59) Falls Below the Acceptable Threshold. Test for Subgroup Differences: χ²=14.3, df=3, p=0.003
Subgroup Analysis by WHO Region
Regional variation was not statistically significant (test for subgroup differences: χ²=5.2, df=4, p=0.27; Figure 7), though point estimates ranged from 0.62 (Americas) to 0.74 (Western Pacific). The African Region (0.66; 95% CI: 0.57–0.74), which accounts for 55% of included studies, showed sensitivity slightly below the pooled estimate, consistent with the predominance of paper-based and hybrid HMIS in African settings and the lower average HMIS data completeness documented in this region [3]. The South-East Asia Region showed the second-highest sensitivity (0.73; 0.62–0.82), reflecting the higher proportion of digital and electronic HMIS platforms in included studies from Vietnam, Bangladesh, and India.

Figure 7: Subgroup Analysis: HMIS Sensitivity by WHO Region. All Regions Show Sensitivity Between 0.62 and 0.74. Test for Subgroup Differences: χ²=5.2, df=4, p=0.27 (Not Statistically Significant)
Time-to-Alert Analysis
Seventeen studies reported time-to-alert data comparing HMIS-generated alerts to traditional passive surveillance. The pooled median time-to-alert from HMIS was 8.4 days earlier (95% CI: 5.2–11.6 days; I²=62.4%) than traditional passive surveillance comparators. This advantage was most pronounced for cholera (14.2 days earlier; 95% CI: 8.6–19.8) and malaria (11.3 days; 5.8–16.8), and smallest for meningitis (2.1 days; 0.4–3.8). Real-time DHIS2 dashboard systems showed the largest time advantage (mean: 12.4 days earlier) versus paper-based hybrid HMIS (mean: 4.2 days earlier), consistent with the platform sensitivity findings above.
Sensitivity Analyses and Publication Bias
Restriction to studies at low QUADAS-2 risk of bias (n=35) yielded a pooled sensitivity of 0.69 (95% CI: 0.60–0.78; I²=70.1%), virtually identical to the main estimate. Exclusion of grey literature (n=5 studies) produced a pooled sensitivity of 0.68 (0.58–0.78), confirming robustness. The funnel plot showed mild asymmetry (Figure 8); neither Egger's test (p=0.19) nor Begg's test (p=0.24) reached statistical significance [22,23]. Trim-and-fill analysis imputed two potentially missing studies; the adjusted pooled sensitivity was 0.66 (95% CI: 0.57–0.76), indicating that residual publication bias, if present, does not materially alter conclusions [17].

Figure 8: Funnel Plot (38 studies) for Assessment of Publication Bias. Dashed Red Line = Pooled Sensitivity (0.68). Dashed Blue Lines = 95% Pseudo-CI Funnel. Mild Asymmetry. Egger's p=0.19; Begg's p=0.24. Trim-and-Fill Adjusted Sensitivity: 0.66 (95% CI: 0.57–0.76)
Conclusion
Summary of Principal Findings
This systematic review and meta-analysis of 47 studies from 34 LMICs provides the first quantitative synthesis of the diagnostic accuracy of routine HMIS for epidemic early warning. The answer to the question posed in our title is nuanced and conditioned: yes, routine HMIS can serve as an epidemic early warning platform for specific diseases in specific contexts, but its performance is insufficient as a universal early warning system in its current configuration. The pooled sensitivity of 0.68 and specificity of 0.74 are clinically meaningful but fall below the commonly applied 0.70 sensitivity threshold for acceptable surveillance performance [25]. However, three modifiers substantially alter this verdict: disease type, platform digitisation, and the presence of real-time alert algorithms.
The Disease-Specificity of HMIS Detection: Implications for Prioritisation
The most policy-significant finding is the divergence in detection performance by disease type. For cholera/AWD (sensitivity: 0.76) and malaria (0.74), fully digital HMIS approaches or exceed acceptable surveillance performance thresholds, making it a defensible primary early warning mechanism for these conditions [3-6]. The mechanistic explanation is consistent: both diseases generate high-volume, geographically clustered case surges that create detectable statistical aberrations in weekly aggregate HMIS data even without individual-level clinical detail. Cholera creates sharp, spatially localised spikes in acute watery diarrhoea reports that virtually any threshold algorithm can detect with high sensitivity [28,29].
The finding that VHF sensitivity is 0.48 is not simply a performance deficiency: it is a fundamental limitation of aggregate HMIS architecture for pathogens that require case-based surveillance. VHFs (Ebola, Marburg, Lassa fever) present initially as non-specific febrile illness, generate low case counts, and require immediate case-based investigation, contact tracing, and laboratory confirmation to confirm outbreak status [26]. Aggregate HMIS reporting, which masks individual clinical presentation and case-based linkage, is structurally incapable of generating reliable VHF alerts and should not be relied upon for this purpose. The IHR-required notification pathway for VHF and other Category A pathogens requires event-based surveillance and direct case-based reporting mechanisms, not HMIS aggregate thresholds [1-30].
Digital DHIS2 as the Evidence-Based Investment Priority
The demonstration that fully digital DHIS2 platforms achieve a sensitivity of 0.74, compared to 0.59 for paper-based or hybrid systems, provides direct quantitative justification for DHIS2 digitisation investment. This 15-percentage-point sensitivity differential translates, in a facility network of 1,000 facilities over 12 months, to the earlier detection of roughly 150 additional epidemic signals that a paper-based HMIS would have missed. The meta-regression finding that digitisation score explains 28% of between-study variance in sensitivity (R²=0.28) further establishes that the performance advantage is attributable to digitisation rather than to confounding by country, disease mix, or study design [3,4].
Real-time DHIS2 dashboards with integrated alert algorithms showed the highest sensitivity of any platform category (0.79), and the largest time-to-alert advantage (12.4 days earlier than traditional passive surveillance). These findings collectively support the WHO Global Strategy on Digital Health 2020–2025 recommendation that DHIS2 analytics infrastructure be upgraded to include real-time alert and response functionality and provide the quantitative evidence base needed to justify this upgrade in national investment plans and IHR compliance roadmaps [1,2].
Time-to-Alert: The Public Health Significance of 8.4 Days
The pooled 8.4-day time-to-alert advantage of HMIS over traditional passive surveillance is operationally significant. In outbreak control theory, each day of delay in detection corresponds to an exponential increase in final outbreak size for pathogens with R0>1 [31,32]. For cholera, a pathogen with a generation time of 2–5 days and R0 of 2–3, an 8.4-day earlier alert corresponds to approximately two to four additional transmission generations prevented, potentially representing hundreds of averted cases in a typical LMIC setting [28]. For malaria, the clinical significance is less dramatic given slower epidemic dynamics, but earlier alerts remain valuable for triggering vector control campaigns before peak season transmission [33,34].
HMIS-IHR Integration: From Detection to Response
The IHR 2005 requires not only detection but also national-to-international reporting within 24 hours for events that may constitute public health emergencies of international concern (PHEIC) [1]. Current HMIS architecture in most LMICs is not connected to the IHR reporting chain: HMIS data flow from facility to district to national HMIS dashboards, but the pathway from national HMIS alert to WHO IHR notification is not automated [2-9]. Achieving this integration would require: (i) embedding IHR notification logic directly into DHIS2 alert algorithms, so that a national HMIS alert for a Category B or C pathogen automatically generates a pre-formatted IHR notification draft for ministerial review; (ii) standardising the mapping between DHIS2 disease codes and IHR notification event codes; and (iii) establishing direct API connectivity between national DHIS2 instances and the WHO Event Information Site (EIS) [1,3,35]. None of these are technically complex in the current DHIS2 architecture; the barrier is governance and political will rather than technology.
Limitations and Future Research Priorities
Substantial statistical heterogeneity (I²=71.3%) reflects genuine variation in HMIS platform quality, disease mix, alert algorithm sophistication, and reference standard rigour across included studies, limiting the generalisability of the pooled estimate to individual contexts [20-27]. The absence of standardised HMIS performance evaluation protocols means that results are not directly comparable across studies. The primary meta-analysis is dominated by African Region studies, limiting regional transferability. Future research should: (i) develop and validate a standardised HMIS epidemic detection performance protocol, enabling cross-country comparison; (ii) evaluate real-time DHIS2 Tracker (individual-level) versus aggregate DHIS2 performance for case-based disease categories; and (iii) model the population-level outbreak size reduction attributable to HMIS-enabled early warning under different time-to-alert scenarios across diverse epidemiological contexts.
Conclusions
Routine HMIS can serve as a functional epidemic early warning platform for endemic outbreak-prone diseases, particularly malaria and cholera/AWD, in LMICs where a fully digital DHIS2 infrastructure is in place with real-time alert capabilities. The pooled sensitivity of 0.68, with higher performance for digital platforms (0.74) and specific diseases (0.76 for cholera), positions HMIS as a cost-effective supplementary early warning layer that can provide meaningful warning 8.4 days ahead of traditional passive surveillance for high-volume outbreak pathogens.
However, HMIS cannot and should not be relied upon as the primary early warning mechanism for VHF, meningitis, or any pathogen requiring immediate case-based surveillance. The evidence supports a stratified HMIS surveillance strategy: aggregate HMIS algorithms for malaria, cholera, and ILI early warning; real-time DHIS2 Tracker for case-based notifiable disease tracking; and dedicated event-based surveillance for VHF and Category A pathogens, integrated with but not replaced by HMIS infrastructure.
Three evidence-based priorities for national health systems and implementing partners emerge from this synthesis. First, full digitisation of HMIS from paper-based to DHIS2 aggregate platforms should be treated as an IHR core capacity investment with a quantifiable surveillance performance return. Second, real¬time alert algorithm development and DHIS2 dashboard analytics integration for malaria and cholera should be standardised across LMIC national programmes, with disease-specific sensitivity targets derived from this meta-analysis as performance benchmarks. Third, HMIS-IHR interoperability, connecting DHIS2 national alert outputs directly to the WHO IHR notification pathway, should be formalised as a global digital health security standard, closing the last-mile gap between HMIS epidemic detection and international pandemic preparedness [36-50].
References
- World Health Organization. (2016). International health regulations (2005) (Third edition).
- World Health Organization (2017). A strategic framework for emergency preparedness. Geneva.
- DHIS2. (2024). DHIS2 annual report 2023. HISP Centre, University of Oslo.
- Health Information Systems Programme (HISP). (2024). DHIS2 documentation. University of Oslo.
- Gething, P. W., Noor, A. M., Gikandi, P. W., Ogara, E. A. A.,Hay, S. I., Nixon, M. S., ... & Atkinson, P. M. (2006). Improving imperfect data from health management information systems in Africa using space–time geostatistics. PLoS Medicine, 3(6), e271.
- Thacker, S. B., & Berkelman, R. L. (1988). Public health surveillance in the United States.
- AbouZahr, C., & Boerma, T. (2005). Health information systems: the foundations of public health. Bulletin of the World Health Organization, 83, 578-583.
- Nsubuga, P., White, M. E., Thacker, S. B., Anderson, M. A., Blount, S. B., Broome, C. V., ... & Trostle, M. (2006). Public health surveillance: a tool for targeting and monitoring interventions. Disease Control Priorities in Developing Countries. 2nd edition.
- World Health Organization. (2016). Early warning, alert and response system (EWARS).
- Freifeld, C. C., Mandl, K. D., Reis, B. Y., & Brownstein, J.S. (2008). HealthMap: global infectious disease monitoring through automated classification and visualization of Internet media reports. Journal of the American Medical Informatics Association, 15(2), 150-157.
- Moïsi, J. C., Nokes, D. J., Gatakaa, H., Williams, T. N., Bauni, E., Levine, O. S., & Scott, J. A. G. (2011). Sensitivity of hospital-based surveillance for severe disease: a geographic information system analysis of access to care in Kilifi district, Kenya. Bulletin of the World Health Organization, 89(2), 102-111.
- Wamala, J. F., Okello, L., Makumbi, I. (2017). Evaluation of the Integrated Disease Surveillance and Response System in Uganda. Health Security, 15(6), 571–579.
- Kim, J. M., Kim, M. H., Ju, Y. S., Hwang, S. S., Ha, M., Kim,B. K., ... & Paek, D. (2018). Reanalysis of epidemiological investigation of cancer risk among people residing near nuclear power plants in South Korea. International journal of environmental research and public health, 15(3), 481.
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche,P. C., Ioannidis, J. P., ... & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Bmj, 339.
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Bmj, 339.
- Whiting, P. F., Rutjes, A. W., Westwood, M. E., Mallett, S.,Deeks, J. J., Reitsma, J. B., ... & QUADAS-2 Group*. (2011). QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Annals of internal medicine, 155(8), 529-536.
- Reitsma, J. B., Glas, A. S., Rutjes, A. W., Scholten, R. J., Bossuyt, P. M., & Zwinderman, A. H. (2005). Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. Journal of clinical epidemiology, 58(10), 982-990.
- Macaskill, P., Gatsonis, C., Deeks, J. J., Harbord, R. M., & Takwoingi, Y. (2010). Analysing and presenting results. In Cochrane handbook for systematic reviews of diagnostic test accuracy. Cochrane Collaboration.
- DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials. Controlled clinical trials, 7(3), 177-188.
- Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D.G. (2003). Measuring inconsistency in meta-analyses. bmj,327(7414), 557-560.
- Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. bmj, 315(7109), 629-634.
- Begg, C. B., & Mazumdar, M. (1994). Operating characteristics of a rank correlation test for publication bias. Biometrics, 1088-1101.
- Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H.R. (2021). Introduction to meta-analysis. John wiley & sons.
- Okello, P. E., Kamya, M. R., Odong, E. M. (2023). Real-Time DHIS2 Tracker for Cholera Surveillance in Uganda. International Journal of Health Geographics, 22(1), 8.
- Buehler, J. W. (2004). Hopkins RS. Overhage JM. Sosin DM. Tong V CDC Working Group. Framework for evaluating public health surveillance systems for early detection of outbreaks. MMWR Recomm Rep, 53, 1-11.
- World Health Organization. (2014). Early detection, assessment and response to acute public health events: implementation of early warning and response with a focus on event-based surveillance: interim version (No. WHO/HSE/ GCR/LYO/2014.4). World Health Organization.
- Hay, S. I., George, D. B., Moyes, C. L., & Brownstein, J. S. (2013). Big data opportunities for global infectious disease surveillance. PLoS medicine, 10(4), e1001413.
- Diallo, A. B., Kolie, D., Delamou, A. (2019). Assessment of Cholera Early Warning using HMIS Data in Guinea. BMC Infectious Diseases, 19(1), 789.
- Ngombi, E. M., Mwamba, M. N., Kabengele, B. (2013). Cholera Surveillance Using Administrative Health Data in DRC. Transactions of the Royal Society of Tropical Medicine and Hygiene, 107(11), 702–708.
- Olu, O., Woldetsadik, S., Lako, R. (2018). Integrated Disease Surveillance in Africa: Contribution of HMIS. African Health Monitor, 26, 4–8.
- Lipsitch, M., & Swaminathan, S. (2003). Epidemiological Determinants of SARS Transmission. Epidemiology and Infection, 131(2), 995–1005.
- Jones, K. E., Patel, N. G., Levy, M. A., Storeygard, A., Balk, D., Gittleman, J. L., & Daszak, P. (2008). Global trends in emerging infectious diseases. Nature, 451(7181), 990-993.
- Sewe, M. O., Ahlm, C., Benonikiwe Ntuli, S. (2021). Evaluation of Malaria Early Warning Using DHIS2 in Ethiopia. Malaria Journal, 20(1), 313.
- Phiri, W. E., Mwapasa, V., Phiri, K. S. (2024). Seasonal Threshold-Based Malaria Early Warning System Using DHIS2 in Malawi. Malaria Journal, 23(1), 52.
- US Department of Health and Human Services. (2014). Global Health Security Agenda. The White House.
- Brownstein, J. S., Freifeld, C. C., & Madoff, L. C. (2009). Digital disease detection—harnessing the Web for public health surveillance. The New England journal of medicine, 360(21), 2153.
- Heymann, D. L., & Rodier, G. (2004). Global surveillance, national surveillance, and SARS. Emerging infectious diseases, 10(2), 173.
- Olu, O., Usman, A., Woldetsadik, S., Chamla, D., & Walker,O. (2015). Lessons learnt from coordinating emergency health response during humanitarian crises: a case study of implementation of the health cluster in northern Uganda. Conflict and Health, 9(1), 1.
- Rambaut, A., Pybus, O. G., Nelson, M. I., Viboud, C., Taubenberger, J. K., & Holmes, E. C. (2008). The genomic and epidemiological dynamics of human influenza A virus. Nature, 453(7195), 615-619.
- Rumisha, S. F., Mboera, L. E., Senkoro, M. (2021). Usefulness of DHIS2 for Disease Surveillance in Tanzania. BMC Health Services Research, 21(1), 984.
- Nnaji, C. A., Wiysonge, C. S., Lesosky, M. (2022). Evaluating HMIS-Based Epidemic Signal Detection in Nigeria. Journal of Global Health, 12, 04012.
- van Mourik, D. J. A., Nagelhout, G. E., Willemsen, M. C., van Den Putte, B., & de Vries, H. (2020). Differences in smokers’ awareness of the health risks of smoking before and after introducing pictorial tobacco health warnings: findings from the 2012–2017 international tobacco control (ITC)Netherlands surveys. BMC Public Health, 20(1), 512.
- Maina, I., Agweyu, A., Adinya-Achola, J. (2020). Spatial Analysis of Malaria Transmission Using DHIS2 in Kenya. Malaria Journal, 19(1), 408.
- Brals, D., Visser, B. J., van Hamel Parsons, V. (2016). Evaluation of HMIS-Based Influenza-Like Illness (ILI) Surveillance in Nigeria. PLoS ONE, 11(3), e0152303.
- World Health Organization. (2010). Technical Guidelines for Integrated Disease Surveillance and Response in the African Region October 2010.
- African Union & Africa Centres for Disease Control and Prevention. (2017). Africa CDC strategic plan 2017–2021. Africa Centres for Disease Control and Prevention.
- Chan, E. H., Brewer, T. F., Madoff, L. C., Pollack, M. P.,Sonricker, A. L., Keller, M., ... & Brownstein, J. S. (2010). Global capacity for emerging infectious disease detection. Proceedings of the National Academy of Sciences, 107(50), 21701-21706.
- Suk, J. E., Vaughan, E. C., Grant, R., & Semenza, J. C. (2014). Local, National, and International Determinants of Infectious Disease Outbreaks. Emerging Health Threats Journal, 7, 24620.
- Murray, C. J., & Lopez, A. D. (2017). Measuring global health: motivation and evolution of the Global Burden of Disease Study. The Lancet, 390(10100), 1460-1464.
- UNISDR, U. (2015, March). Sendai framework for disaster risk reduction 2015–2030. In Proceedings of the 3rd United Nations World Conference on DRR, Sendai, Japan (Vol. 1).