
New Advances in Brain & Critical Care(NABCC)
ISSN: 2771-7887 | DOI: 10.33140/NABCC
Impact Factor: 1.01



Review Article - (2025) Volume 6, Issue 1
Bridging Neural Circuits and Sacred Spaces: Integrating Neurobiological Mechanisms with Intangible Experience
Received Date: Apr 21, 2025 / Accepted Date: May 19, 2025 / Published Date: May 26, 2025
Copyright: ©Â©2025 Julian Ungar-Sargon. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ungar-Sargon, J. (2025). Bridging Neural Circuits and Sacred Spaces: Integrating Neurobiological Mechanisms with Intangible Experience. New Adv Brain & Critical Care, 6(1), 01-12.
Abstract
This integrative review explores the intersection of neurobiological mechanisms and intangible aspects of neurological disease through the complementary frameworks of CR Mukundan's neurobiological model, Iain McGilchrist's hemispheric theory, and the author's therapeutic approach. The article synthesizes current understanding of how brain structures generate consciousness and examines how the different modes of attention provided by cerebral hemispheres influence our experience of reality. Particular focus is placed on the integration of spirituality, music, and holistic healing practices in the treatment of neurological conditions. Research demonstrates that acknowledging the spiritual dimension in neurological care enhances therapeutic outcomes by recognizing both the material basis of consciousness in the brain and the immaterial experiences that arise from it. This integrated framework offers a more comprehensive understanding of neurological diseases and points toward more effective and compassionate treatment approaches that address both the neurobiological mechanisms and the lived experience of patients.
Keywords
Neurobiological Mechanisms, Hemispheric Specialization, Intangible Aspects, Spirituality, Music Therapy, McGilchrist, Therapeutic Relationship, Holistic Healing, Consciousness
Introduction
The study of the human brain has traditionally focused on its material aspects the neural structures, circuits, and biochemical processes that underlie cognition, emotion, and behaviour. While this approach has yielded remarkable insights into brain function and dysfunction, it often fails to adequately address the experiential dimensions of neurological disease. Patients with neurological conditions experience not only physical symptoms but also alterations in their sense of self, their relationship to the world, and their spiritual well-being. These intangible aspects of neurological disease are frequently overlooked in conventional biomedical frameworks, yet they significantly impact quality of life and treatment outcomes [1-6]. This article proposes an integrated framework that bridges the materialist understanding of brain function with the experiential and spiritual dimensions of neurological conditions. Drawing on the neurobiological model developed by Mukundan and colleagues, McGilchrist's theory of hemispheric specialization, and the author's own work on spirituality and healing, this framework offers a more comprehensive approach to understanding and treating neurological diseases [1-20].

Figure 2
The genesis of behaviour and mind from the brain, as detailed in Mukundan's work, provides the foundation for understanding how neural structures and processes give rise to mental phenomena [1-6]. McGilchrist's exploration of hemispheric differences offers valuable insights into how different modes of attention shape our experience of reality [7-11]. The author's research on spirituality, music, and healing complements these perspectives by addressing the experiential and transcendent dimensions of neurological conditions [12-20]. By integrating these complementary perspectives, this article aims to develop a more nuanced understanding of the relationship between brain and mind, with particular attention to the intangible aspects of neurological disease. Such an integrated approach has significant implications for clinical practice, suggesting more holistic and effective strategies for diagnosis, treatment, and support of patients with neurological conditions.
Material Foundations of Intangible Experience
The relationship between the physical brain and the experiential mind remains one of the most profound questions in neuroscience. Mukundan's extensive work on the "genesis of behaviour and mind from the brain" has established a comprehensive model of how neural structures and processes give rise to complex mental phenomena [1-6]. This model details how various brain regions, from the brainstem to the prefrontal cortex, contribute to different aspects of consciousness, cognition, and emotion. Central to this model is the understanding that mind emerges from the integrated functioning of multiple brain systems. As Mukundan states, "Mind is a strange and powerful functional character of the brain in all individuals" [3]. The mind is not located in any single brain region but arises from the coordinated activity of neural networks distributed throughout the brain. This perspective avoids the reductionist trap of equating mind with brain while acknowledging the material foundation of mental processes. The emergence of consciousness from neural activity involves complex interactions between subcortical structures, such as the thalamus and brainstem, and cortical regions, particularly the frontal and parietal lobes [1,2,6]. These interactions create the essential features of conscious experience: wakefulness, attention, self-awareness, and intentionality. However, as Mukundan emphasizes, consciousness is not merely the sum of neural activities but represents a qualitatively distinct level of organization [4,5].

Figure 3: Beyond Material Reductionism
McGilchrist's work offers a critical perspective on the limitations of material reductionism in understanding the brain-mind relationship [7-11]. His research on hemispheric specialization suggests that the different modes of attention provided by the left and right hemispheres create fundamentally different ways of experiencing and engaging with reality. In "The Master and His Emissary," McGilchrist argues that the left hemisphere specializes in a narrow, focused mode of attention that isolates, abstracts, and categorizes, while the right hemisphere provides a broad, open, and receptive mode of attention that grasps wholes and their interconnections [7].
These different modes of attention do not merely process different types of information but create distinctly different experiences of reality. McGilchrist challenges the conventional materialist view that consciousness is merely an epiphenomenon of brain activity. Instead, he proposes a more nuanced understanding where "consciousness is the stuff of the cosmos" and "matter is a phase of consciousness" [11]. This perspective suggests that consciousness is not produced by the brain but is rather channelled or constrained by it, with different brain states allowing access to different aspects of a more fundamental conscious reality.

Figure 4: Integrative Approach
Building on these foundations, my own research has explored the integration of neurobiological understanding with spiritual and experiential dimensions of healing [12-20]. This approach recognizes that while neural mechanisms provide the material substrate for consciousness, the lived experience of patients with neurological conditions cannot be reduced to brain pathology alone. In my work on the spirituality of chronic pain and neurological disorders, I have emphasized how spiritual practices and beliefs influence the experience and management of these conditions [13, 14,20]. Spirituality provides a framework for finding meaning in suffering, cultivating resilience, and accessing dimensions of experience that transcend physical limitations. These aspects are not separable from neurobiological processes but represent a different level of description that captures elements of experience not adequately addressed by purely material accounts. The integration of these perspectives Mukundan's neurobiological model, McGilchrist's hemispheric theory, and my own work on spirituality and healing provides a more comprehensive framework for understanding the brain-mind relationship. This framework acknowledges the material foundations of consciousness while recognizing that the experiential dimensions of neurological conditions cannot be reduced to their neurobiological substrates.
Hemispheric Specialization and Neurological Disease
McGilchrist's research on hemispheric specialization offers profound insights into the nature of neurological disease [7-10]. According to McGilchrist, the cerebral hemispheres provide fundamentally different modes of attention to the world the left hemisphere offering a focused, analytical mode that divides the world into parts, and the right hemisphere providing a broad, holistic mode that perceives wholes and their interconnections [7]. These different modes of attention are not simply complementary but often stand in tension with each other. The left hemisphere's mode of attention tends to abstract, categorize, and control, creating a representation of reality that is manageable but partial. The right hemisphere's mode of attention is more receptive, contextual, and embodied, maintaining connection with the living reality of the world [9]. McGilchrist argues that the balance between these hemispheric perspectives is crucial for healthy functioning. When this balance is disrupted, whether through brain injury, disease, or cultural influences, our experience of reality becomes distorted [7]. In neurological conditions, this disruption can manifest in various ways, from perceptual distortions and cognitive deficits to alterations in emotional processing and spiritual experience. The concept of hemispheric imbalance offers a valuable framework for understanding a wide range of neurological conditions. Research has shown that conditions such as autism spectrum disorders, schizophrenia, and depression are associated with altered patterns of hemispheric activation [7,21-26]. For example, studies suggest that autism shares many traits with left-hemisphere dominance, including preference for familiarity, categorization, and difficulty with social-emotional processing [7]. In my clinical work with patients with neurological conditions, I have observed patterns consistent with McGilchrist's model. Patients with right-hemisphere damage often exhibit deficits in understanding metaphor, humour, and social cues, reflecting the right hemisphere's role in contextual and relational understanding [13,15]. Conversely, patients with left-hemisphere damage may show enhanced appreciation of holistic and spiritual dimensions of experience, despite impairments in language and analytical thinking [16,17]. These observations suggest that neurological conditions do not merely cause deficits in specific cognitive domains but can fundamentally alter the patient's mode of attending to and experiencing the world. Understanding these alterations in terms of hemispheric balance provides a more nuanced framework for diagnosis and treatment than approaches that focus solely on specific neural circuits or neurotransmitter systems.

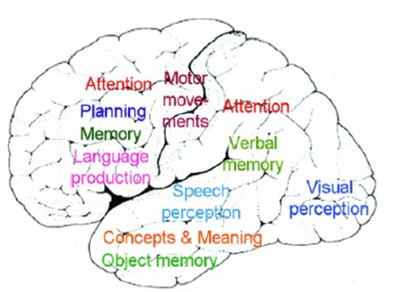
Figure 5: Neural Substrates
The physiological basis of hemispheric specialization involves complex networks of neural structures distributed throughout the brain [27-33]. While the popular conception of a "left brain" and "right brain" greatly oversimplifies neuroanatomy, research in neurophysiology has identified significant differences in connectivity patterns, neurotransmitter distributions, and functional specializations between the hemispheres [7-9]. Key structures involved in hemispheric specialization include the corpus callosum, which mediates interhemispheric communication; the frontal lobes, which regulate attention and executive functions; the temporal lobes, which process auditory, linguistic, and social information; and the limbic system, which integrates emotion, memory, and motivation [9,21-26,30-37]. The orbitofrontal cortex and anterior cingulate play particularly important roles in mediating between hemispheric perspectives [28,38-44]. These structures are involved in integrating emotional and cognitive processes, regulating attention, and resolving conflicts between competing representations of reality. Dysfunction in these regions can disrupt the balance between hemispheric perspectives, contributing to a wide range of neurological and psychiatric conditions [45-48]. Understanding the neural substrates of hemispheric specialization can inform more targeted and effective interventions for neurological conditions. By identifying specific patterns of hemispheric imbalance in individual patients, clinicians can develop personalized treatment approaches that address both the neurobiological mechanisms and the experiential dimensions of these conditions.

Figure 6: The Spiritual Dimension of Neurological Experience
While conventional neurology focuses primarily on the physical symptoms and cognitive deficits associated with neurological conditions, a growing body of research suggests that these conditions also profoundly affect the spiritual dimension of human experience [12-20]. Spirituality, understood as the search for meaning, purpose, and transcendence, represents an essential aspect of well-being that is often overlooked in biomedical approaches to neurological care. In my clinical work, I have observed how neurological conditions can disrupt patients' sense of identity, purpose, and connection to something greater than themselves [12,13,20]. These disruptions can manifest as existential distress, spiritual suffering, or a profound sense of disconnection from self, others, and the sacred. Conversely, some neurological conditions, particularly those involving altered states of consciousness, can open patients to new spiritual insights and experiences that may be transformative [13,17]. Research on the relationship between spirituality and neurological health suggests that spiritual well- being is associated with better outcomes across a range of conditions, including epilepsy, stroke, dementia, and chronic pain [14,20]. Spirituality provides resources for coping, meaning- making, and resilience that can significantly impact quality of life and functional status, independent of disease severity or prognosis [16,18,19].

Figure 7: Music as a Neural Bridge
Music offers a powerful bridge between the neural and spiritual dimensions of healing in neurological care [12,15]. My research on music and neural function has explored how music engages multiple brain regions, from the brainstem and cerebellum to the limbic system and cortical networks, creating integrated patterns of activity that transcend the typical boundaries of neural processing [12]. The unique capacity of music to simultaneously engage emotional, cognitive, and sensorimotor systems makes it an ideal medium for addressing the complex needs of patients with neurological conditions [12]. Music activates the right hemisphere's holistic, emotional, and contextual mode of processing while also engaging left-hemisphere structures involved in temporal sequencing and analytical processing [12,15]. This cross-hemispheric integration can help restore balance in conditions characterized by hemispheric imbalance [12]. Beyond its neurophysiological effects, music connects patients to dimensions of experience that transcend the physical and cognitive limitations imposed by their conditions [12,15]. In my clinical work, I have observed how music can evoke spiritual experiences of beauty, meaning, and transcendence even in patients with severe cognitive or communicative impairments [12]. These experiences are not merely psychological or aesthetic but touch on the deepest dimensions of human existence, offering patients a sense of connection to something greater than themselves [12, 15].
Therapeutic Applications
The integration of spirituality into neurological care offers promising avenues for enhancing treatment outcomes and quality of life for patients with a wide range of conditions [13- 20]. In my clinical practice, I have developed several approaches for addressing the spiritual dimension of neurological disease, including spiritual assessment, meaning-centered therapy, and contemplative practices adapted for patients with cognitive or physical limitations [13,18,19]. Spiritual assessment involves exploring the patient's beliefs, values, and sources of meaning and support, as well as identifying spiritual distress or resources that may impact their experience of illness and recovery [20]. This assessment provides essential information for developing a treatment plan that addresses the whole person, not just their neurological symptoms [19]. Meaning-centered therapy helps patients discover or create meaning in their experience of illness, drawing on their personal values, cultural traditions, and spiritual resources [18,19]. This approach has been particularly effective for patients with conditions that involve significant loss, such as stroke, traumatic brain injury, and neurodegenerative diseases [16,18]. Contemplative practices, including meditation, prayer, and sacred music, can be adapted to meet the needs and capabilities of patients with various neurological conditions [12,13,15]. These practices engage the right hemisphere's intuitive, holistic mode of processing, balancing the left hemisphere's analytical focus that often dominates medical care [15,17]. They also provide patients with tools for managing symptoms, reducing stress, and accessing inner resources for healing and growth [13,20].

Figure 8: Social Conditioning
The human brain develops and functions within a social context that profoundly shapes its structure and activity. Research on social neuroscience has demonstrated how social experiences, from early attachment to ongoing relationships and cultural influences, affect neural development, connectivity, and function [25,49,50]. These findings challenge the individualistic model that dominates much of neurology and psychiatry, suggesting that neurological health must be understood within a broader social and cultural context. Mukundan's work on social conditioning emphasizes the critical role of early social experiences in developing normal brain function, particularly in the frontal lobes [1-6]. The frontal lobes, especially the orbitofrontal cortex, are essential for inhibitory control, emotional regulation, and social cognition [45-48]. These functions develop through social interaction, with caregivers providing the external regulation that gradually becomes internalized as self-regulation [51-53]. When social conditioning is inadequate or harmful, as in cases of neglect, abuse, or trauma, neural development can be disrupted, leading to long-term alterations in brain function and behaviour [25,49,50]. These alterations can manifest as neurological and psychiatric conditions, including disinhibition syndromes, emotional dysregulation, and social-cognitive deficits [45-48]. Understanding these conditions as products of disrupted social conditioning, rather than purely individual pathology, has important implications for treatment and prevention.
McGilchrist's Critique
McGilchrist extends the analysis of social conditioning to the cultural level, arguing that Western culture has become increasingly dominated by the left hemisphere's mode of attention, with detrimental effects on individual and collective well-being [7,8]. This cultural imbalance is reflected in and reinforced by educational systems, medical models, and technological developments that prioritize abstraction, analysis, and control over embodied, relational, and contextual understanding [7]. In "The Master and His Emissary," McGilchrist traces the historical development of this hemispheric imbalance, showing how it has shaped everything from philosophical systems and scientific paradigms to artistic movements and political structures [7]. He argues that this imbalance has reached a critical point in contemporary culture, contributing to a range of social and psychological problems, including alienation, fragmentation, and a loss of meaning and connection [7,8]. For patients with neurological conditions, this cultural context adds an additional layer of challenge. Not only must they cope with the direct effects of their condition, but they must do so within a cultural environment that may exacerbate their difficulties, particularly for those with right-hemisphere deficits or conditions that affect social- emotional processing [7-10]. In my own work, I have developed an integrative approach to neurological care that addresses both the individual and social dimensions of health and healing [15- 20]. This approach recognizes that neurological conditions do not occur in isolation but are embedded in a network of relationships, cultural influences, and social structures that can either support or impede recovery and well-being.
Central to this approach is the concept of the healing community a social environment that fosters connection, meaning, and wholeness, counterbalancing the fragmentation and alienation that often characterize both neurological disease and contemporary culture [17,19]. The healing community can take many forms, from supportive families and therapeutic groups to spiritual communities and social networks, but all share certain essential qualities: acceptance, presence, and a commitment to the well- being of all members [19]. In my clinical practice, I actively engage with patients' social networks, helping to transform them into healing communities that can support the patient's recovery and growth [17,19]. This often involves educating family members and caregivers about the patient's condition and needs, facilitating communication and connection, and addressing social barriers to health and well-being [17-19]. I also work at the community level, developing programs and initiatives that foster social connection, meaning, and spiritual well-being for individuals with neurological conditions [18,19]. This integrative social approach has shown promising results in improving outcomes for patients with various neurological conditions, from chronic pain and neurodegenerative diseases to acquired brain injuries and developmental disorders [17-20]. By addressing both the neurobiological and social dimensions of disease, this approach offers a more comprehensive framework for promoting health and healing in an increasingly fragmented and alienating world.

Figure 9: Beyond Mechanistic Medicine
The therapeutic relationship is not merely a context for delivering medical interventions but a powerful healing modality in its own right. Research in interpersonal neurobiology has demonstrated how the brain responds to human connection, with significant implications for understanding and enhancing the therapeutic encounter [54-58]. This research reveals that the brain is fundamentally social, with specialized systems for recognizing, interpreting, and responding to other humans [56-58]. The mirror neuron system, which activates similar patterns of neural firing when we observe others' actions and emotions as when we experience them ourselves, provides a neurobiological basis for empathy and emotional attunement [54,56]. This system enables the therapist to resonate with the patient's experience, creating a shared neural state that can promote healing and well-being [56,57]. The neurochemical basis of therapeutic connection involves several interrelated systems, including the oxytocin-vasopressin system, which promotes bonding and trust; the dopamine reward system, which reinforces positive social interactions; and the endogenous opioid system, which mediates both pain relief and social attachment [45-47,54-58]. When the therapeutic relationship activates these systems, it can reduce pain and distress, enhance immune function, and promote neuroplasticity and healing [56- 58].
Presence and Listening
In my clinical work, I have emphasized the importance of presence and active listening in the therapeutic encounter [13,14,16,17]. Presence involves a quality of attentiveness and openness that goes beyond technical skill or procedural competence. It requires the therapist to be fully engaged, both cognitively and emotionally, creating a space where the patient can feel seen, heard, and valued [13,17]. Active listening extends beyond a communication skill to become a therapeutic intervention in its own right [13]. It requires presence, engagement, and a willingness to enter into the patient's experience without judgment or premature interpretation [13,17]. When patients feel truly heard, they experience a validation of their humanity and personhood that can be profoundly healing, particularly for those whose sense of self has been disrupted by neurological disease [13,16,17]. The quality of presence and listening in the therapeutic encounter engages the right hemisphere's holistic, emotional, and relational mode of processing, balancing the left hemisphere's analytical, procedural focus that dominates much of medical practice [7-10,13,17]. This hemispheric balance creates a therapeutic space where both the physical and existential dimensions of neurological disease can be addressed [13,17].

Figure 10: The Sacred Dimension of Healing Spaces
The concept of sacred space offers a valuable framework for understanding and enhancing the therapeutic environment in neurological care [17,19]. Sacred spaces are characterized by a quality of presence, intention, and reverence that creates a container for transformation and healing [17]. While traditionally associated with religious settings, the quality of sacredness can infuse any space where healing is intended, including hospitals, clinics, and therapy rooms [17,19]. In my essay "Sacred and Profane Space in the Therapeutic Encounter," I explore how the physical, social, and energetic qualities of the healing environment influence the therapeutic process [17]. The arrangement of space, the quality of light and sound, the presence of natural elements, and the attitudes and intentions of those present all contribute to creating an environment that supports healing at multiple levels physical, emotional, mental, and spiritual [17]. The contrast between sacred and profane space is particularly relevant in contemporary healthcare settings, which often prioritize efficiency, standardization, and technical intervention over presence, connection, and meaning [17]. The mechanistic paradigm that dominates modern medicine tends to create spaces that are alienating, disempowering, and devoid of symbolic or spiritual significance [17,19]. Creating sacred healing spaces requires a conscious effort to balance these technological and procedural elements with qualities that engage the right hemisphere's holistic, embodied, and relational mode of being [17,19]. In my clinical practice, I actively work to create sacred healing spaces that support the whole person body, mind, and spirit [17,19]. This involves attention to the physical environment, the quality of presence and interaction, and the integration of elements that evoke depth, beauty, and meaning [17]. Music, art, natural elements, and symbolic objects can all contribute to creating a therapeutic environment that engages the patient's innate capacity for healing and growth [12,15,17].
Clinical Applications
The integrated framework presented in this article has significant implications for the assessment of neurological conditions. Traditional neurological assessment focuses primarily on identifying structural and functional abnormalities in the brain through physical examination, cognitive testing, and neuroimaging [24,59-65]. While these approaches provide valuable information about the material basis of neurological conditions, they often fail to capture the experiential and spiritual dimensions of disease [12-20]. An integrated assessment approach expands the scope of inquiry to include the patient's subjective experience, meaning-making processes, and spiritual resources and concerns [13,16,18,19]. This approach uses both quantitative measures, such as standardized questionnaires and functional assessments, and qualitative methods, including phenomenological inquiry and narrative exploration [13,18,19]. In my clinical practice, I have developed an assessment protocol that addresses multiple dimensions of neurological experience [13,18,19]:
Physical dimension: Symptoms, functional limitations, and neurobiological mechanisms of disease [13,18]
Cognitive dimension: Cognitive abilities and deficits, information processing, and executive functions [13,18]
Emotional dimension: Emotional responses to illness, mood states, and affective regulation [13, 18]
Social dimension: Relationship status, social support, and community resources [13,18]
Existential dimension: Meaning and purpose, identity, and life goals [13,18]
Spiritual dimension: Spiritual beliefs, practices, resources, and concerns [13,18,19]
This multidimensional assessment provides a more comprehensive understanding of the patient's condition and needs, informing a treatment plan that addresses the whole person, not just their neurological symptoms [13,18,19].

Figure 11: Integrative Treatment Approaches
Based on this integrated framework, we need a range of treatment approaches that address both the neurobiological mechanisms and the experiential dimensions of neurological conditions [12-20]. These approaches will draw on conventional medical interventions, complementary therapies, and spiritual practices, tailored to the individual needs and preferences of each patient [13,18,19].
Key elements of this integrative approach include:
• Conventional Medical Interventions: Medications, surgery, and rehabilitation therapies that address the neurobiological mechanisms of disease [13,18]
• Neuromodulation Techniques: Non-invasive brain stimulation, neurofeedback, and meditation practices that promote neural plasticity and hemispheric balance [13,18]
• Music and Sound Therapy: Structured musical experiences that engage cross hemispheric integration, emotional processing, and spiritual awareness [12,15]
• Body-Based Practices: Movement therapies, sensory integration, and somatic awareness practices that address the embodied dimension of neurological experience [13,18]
• Meaning-Centered Therapy: Narrative, existential, and spiritual approaches that help patients discover or create meaning in their experience of illness [13,16,18,19]
• Social and Community Interventions: Family therapy, support groups, and community programs that foster connection, belonging, and mutual support [17,18,19]
These approaches are not applied in isolation but are integrated into a coherent treatment plan that addresses the unique constellation of needs, challenges, and resources presented by each patient [13,18,19]. To illustrate the application of this integrated framework in clinical practice, I present two case examples from my work with patients with neurological conditions.
Case 1: Chronic Pain and Spiritual Suffering
Sarah, a 45-year-old woman with chronic neuropathic pain following a spinal cord injury, presented with severe pain, depression, and spiritual distress [14,20]. Her conventional pain management had been only partially effective, and she expressed a profound sense of abandonment by God and loss of meaning in her life [14,20]. An integrated assessment revealed not only the neurobiological mechanisms of her pain but also the existential and spiritual dimensions of her suffering [14,20]. Her pain was exacerbated by her spiritual distress, creating a cycle of physical and existential suffering that conventional approaches alone could not address [14,20]. Treatment involved a combination of medication optimization, neuromodulation techniques, and spiritual counselling [14,20]. Music therapy sessions helped Sarah access dimensions of experience beyond her pain, reconnecting her to sources of beauty, meaning, and transcendence [12,15].
A spiritual support group provided community and solidarity with others facing similar challenges, reducing her sense of isolation and abandonment [17,19]. Over time, Sarah developed a transformed relationship with her pain and a renewed sense of purpose and connection [14,20]. While her physical pain persisted to some degree, her suffering was significantly reduced, and she reported a deeper sense of peace and meaning in her life [14,20].
Case 2: Hemispheric Imbalance in Traumatic Brain Injury
Michael, a 32-year-old man with a traumatic brain injury primarily affecting his right frontal and temporal lobes, presented with impaired social cognition, emotional processing, and spiritual awareness [13,17]. He had made good progress in conventional rehabilitation but continued to struggle with relationships, meaning-making, and a sense of disconnection from his former values and spiritual life [13,17]. Assessment revealed a pattern consistent with left-hemisphere dominance due to right-hemisphere damage, affecting his ability to grasp wholes, understand context, and process emotional and spiritual information [7,13,17]. His analytical abilities remained intact, but he had difficulty integrating these with emotional and intuitive understanding [13,17]. Treatment focused on strengthening right-hemisphere functions and promoting hemispheric integration [13,17]. Music therapy sessions engaged his emotional and intuitive capacities, bypassing his verbal deficits to access deeper dimensions of experience [12,15]. Group therapy provided opportunities to practice social cognition and emotional recognition in a supportive environment [17,19]. Contemplative practices, adapted to his cognitive abilities, helped him reconnect with his spiritual values and sense of meaning [13,17]. Michael's recovery involved not just improved cognitive and functional abilities but a reintegration of his analytical and intuitive capacities, emotional and rational understanding, and personal and spiritual dimensions of self [13,17]. This holistic recovery enabled him to rebuild relationships, find new meaning in his changed circumstances, and develop a deeper connection to his spiritual values [13,17].

Figure 12
Conclusion
This article has presented an integrated framework for understanding and addressing the intangible aspects of neurological disease, drawing on the complementary perspectives of Mukundan's neurobiological model, McGilchrist's hemispheric theory, and the author's work on spirituality and healing. This framework offers a more comprehensive approach to neurological care that addresses both the material mechanisms and the experiential dimensions of disease.
The integration of these perspectives yields several important insights:
• The mind emerges from but is not reducible to the brain, representing a distinct level of organization with unique properties and dynamics [1-11].
• The cerebral hemispheres provide fundamentally different modes of attention to the world, with the balance between these perspectives being crucial for health and well-being [7-10].
• Neurological conditions affect not only physical and cognitive functions but also the spiritual dimension of human experienceincluding meaning, purpose, and transcendence [12-20].
• Music and other creative arts engage multiple brain systems, providing unique therapeutic tools for addressing both the neural and spiritual dimensions of healing [12,15].
• Social conditioning and cultural context profoundly influence neurological health, requiring attention to both individual and collective dimensions of healing [1-10,16-20,25,49,50].
• The therapeutic relationship itself is a powerful healing modality, engaging neurobiological processes of connection, regulation, and integration [13,16,17,54-58].
• Clinical applications of this integrated framework include multidimensional assessment, integrative treatment approaches, and attention to the quality of the healing environment [12-20].
These insights point toward a unified understanding of mind and brain that honours both the materiality of neural processes and the immateriality of conscious experience. This understanding has profound implications for the field of neurology, suggesting a more humanistic and holistic approach to the study and treatment of neurological conditions. By addressing both the tangible and intangible aspects of neurological disease, this integrated approach offers new possibilities for healing and growth, even in conditions where complete physical recovery is not possible. It recognizes that the ultimate goal of neurological care is not merely the restoration of brain function but the support of the whole person in their journey toward meaning, connection, and well-being. As we continue to advance our understanding of the brain's material mechanisms, we must not lose sight of the immaterial dimensions of mind and spirit that give human life its depth and significance. By integrating these complementary perspectives, we can develop a more comprehensive and compassionate approach to neurological care that addresses the full spectrum of human experience [24,66- 87].
References
- Mukundan, C. R. (2023). The virtual world of the mind. Psychol Psychother Res Stud, 6(3), PPRS.000638.
- Mukundan, C. R., Kamarajan, C., Kacker, P. (2023). The world, created by human minds. GAP BODHI TARU: A Global Journal of Humanities, 56(1), 22-28.
- Mukundan, C. R., Kamarajan, C. (2022). Brain to mind- cognitive and emotional journey within the human brain. EC Neurol,14(2), 01-08.
- Mukundan, C. R., Kamarajan, C. (2021). Brain to mind: Creation of the virtual world. Adv Soc Sci Res J, 8(10), 513- 544.
- Mukundan, C. R., & Kamarajan, C. (2020). The real physical world and the virtual mental world. J Psychol Clin Psychiatry, 11(6), 170-175.
- Mukundan, C. R., & Kacker, P. (2020). Brain and Mind: Mind Created from the Brain–Dependent on Material: Scientific Principles and Relationships in the Brain, and on the Independently Created Mind Relationships and Principles. GAP Indian Journal of Forensics and Behavioural Sciences, 1, 62-65.
- McGilchrist, I. (2019). The master and his emissary: The divided brain and the making of the western world. Yale University Press.
- McGilchrist, I. (2021). The Matter with Things Our Brains, Our Delusions and the Unmaking of the World. Volume I, The Ways to the Truth.
- McGilchrist, I. (2010). Reciprocal organization of the cerebral hemispheres. Dialogues in clinical neuroscience, 12(4), 503- 515.
- McGilchrist, I. (2018). Ways of attending: How our divided brain constructs the world. Routledge.
- McGilchrist, I. (2021). Consciousness is the stuff of thecosmos. [Presentation] Science of Consciousness Conference.
- Ungar-Sargon, J. (2025). Music and neural function in spiritual healing. J Healing Arts.
- Ungar-Sargon, J. (2024). Effective listening affects patientoutcomes. J Healing Arts.
- Ungar-Sargon, J. (2024). The neuroscience behind the placeboeffect. J Healing Arts.
- Ungar-Sargon, J. (2025). Hermeneutic approaches to medicine. J Healing Arts.
- Ungar-Sargon, J. (2025). The crisis of language in therapeutic spaces. J Healing Arts.
- Ungar-Sargon, J. (2025). Sacred and profane space in the therapeutic encounter. J Healing Arts.
- Ungar-Sargon, J. (2025). A new vision for the physician- patient relationship. J Healing Arts.
- Ungar-Sargon, J. (2025). Comparing and integrating the 12 Step Recovery and classical medical models. J Healing Arts.
- Ungar-Sargon, J. (2023). Spirituality of chronic pain and healing approaches. American Journal of Neurological Practice, 15(2), 78-92.
- Luria, A. R. (1969). Frontal lobe syndromes.
- Luria, A. R. (1980). Higher cortical functions in man. New York.
- Luria, A. R. (1981). Human brain and psychological processes. New York: Harper & Row.
- Petrides, M., Alivisatos, B., Meyer, E., & Evans, A. C. (1993). Functional activation of the human frontal cortex during the performance of verbal working memory tasks. Proceedings of the National Academy of Sciences, 90(3), 878-882.
- Petrides, M., & Milner, B. (1982). Deficits on subject- ordered tasks after frontal-and temporal-lobe lesions in man. Neuropsychologia, 20(3), 249-262.
- Teuber, H. L. (2009). The riddle of frontal lobe function in man. Neuropsychology review, 19(1), 25-46.
- Warren, J. M., & Akert, K. (1964). The frontal granular cortex and behaviour, 410-444.
- Mukundan, C. R. (1999). Power of Words: Neuro-cognitive approach for understanding brain mechanisms of awareness. Scientific and Philosophical Studies on Consciousness. National institute of Advanced Studies, Bangalore, India, 127- 136.
- Abe, N., Suzuki, M., Tsukiura, T., Mori, E., Yamaguchi, K., Itoh, M., & Fujii, T. (2006). Dissociable roles of prefrontal and anterior cingulate cortices in deception. Cerebral cortex, 16(2), 192-199.
- Goleman, D. (1998). Working with emotional intelligence.Bantam.
- LeDoux, J. (1996). Emotional networks and motor control: a fearful view. Progress in brain research, 107, 437-446.
- LeDoux, J. (1998). Fear and the brain: where have we been, and where are we going. Biological psychiatry, 44(12), 1229- 1238.
- LeDoux, J., Heller, M., Brożek, B., & DÄ?biec, J. (2002). Theemotional brain revisited. The synaptic self, 200-234.
- LeDoux, J. (2003). The emotional brain, fear, and the amygdala. Cellular and molecular neurobiology, 23, 727-738.
- Milner, B. (2005). The medial temporal-lobe amnesic syndrome. Psychiatric Clinics, 28(3), 599-611.
- Milner, B., Petrides, M., & Smith, M. L. (1985). Frontal lobes and the temporal organization of memory. Human neurobiology, 4(3), 137-142.
- Milner, A. D., Paulignan, Y., Dijkerman, H. C., Michel, F., & Jeannerod, M. (1999). A paradoxical improvement ofmisreaching in optic ataxia: new evidence for two separate neural systems for visual localization. Proceedings of the Royal Society of London. Series B: Biological Sciences, 266(1434), 2225-2229.
- Milner, A. D., Perrett, D. I., Johnston, R. S., Benson, P. J.,Jordan, T. R., Heeley, D. W., ... & Davidson, D. L. W. (1991). Perception and action in ‘visual form agnosia’. Brain, 114(1), 405-428.
- Cummings, J. L. (1993). Frontal-subcortical circuits and human behavior. Archives of neurology, 50(8), 873-880.
- D'esposito, M., Detre, J. A., Alsop, D. C., Shin, R. K., Atlas, S., & Grossman, M. (1995). The neural basis of the central executive system of working memory. Nature, 378(6554), 279-281.
- Posner, M. I., & DiGirolamo, G. J. (1998). Executiveattention: Conflict, target detection, and cognitive control. InR. Parasuraman (Ed.), The attentive brain (pp. 401–423). The MIT Press.
- Frith, C. D., Friston, K. J., Liddle, P. F., & Frackowiak, R. S. (1991). Willed action and the prefrontal cortex in man: a study with PET. Proceedings of the Royal Society of London. Series B: Biological Sciences, 244(1311), 241-246.
- Botvinick, M., Nystrom, L. E., Fissell, K., Carter, C. S., & Cohen, J. D. (1999). Conflict monitoring versus selection-for- action in anterior cingulate cortex. Nature, 402(6758), 179- 181.
- Bush, G., Luu, P., & Posner, M. I. (2000). Cognitive and emotional influences in anterior cingulate cortex. Trends in cognitive sciences, 4(6), 215-222.
- Bush, G., Vogt, B. A., Holmes, J., Dale, A. M., Greve, D., Jenike, M. A., & Rosen, B. R. (2002). Dorsal anterior cingulate cortex: a role in reward-based decision making. Proceedings of the National Academy of Sciences, 99(1), 523-528.
- Kandel, E. (1992). Biology, violence, and antisocial personality. Journal of Forensic Sciences, 37(3), 912-918.
- Goldar, J. C., Rojas, D., & Outes, M. (1993). A neurobiological model of mind. Acta Psiquiatrica y Psicologica de America Latina, 39(1), 33-44.
- Starkstein, S. E., & Robinson, R. G. (1997). Mechanism of disinhibition after brain lesions. The Journal of nervous and mental disease, 185(2), 108-114.
- Schmitz, M. F. (2003). Influences of race and family environment on child hyperactivity and antisocial behavior. Journal of Marriage and Family, 65(4), 835-849.
- Miles, D. R., & Carey, G. (1997). Genetic and environmental architecture on human aggression. Journal of personality and social psychology, 72(1), 207-217.
- Garnefski, N., & Okma, S. (1996). Addiction-risk and aggressive/criminal behaviour in adolescence: Influence of family, school and peers. Journal of adolescence, 19(6), 503- 512.
- Mukundan, C. R. (1986). Schizophrenia: an attention deficit syndrome. In: Menon MS, Nagaswami V, editors. Biology of Schizophrenia: State of the Art. Proceedings of the SCARF Symposium on New Vistas in Biological Understanding of Schizophrenia, Bombay. SCARF Publication, 26-42.
- Mukundan, C. R. (1986). Some psychophysiological and neuropsychological findings in abstinent alcoholics. In: Ray RR, Perkins W, editors. Proceedings of Indo US symposium on Alcohol and Drug Abuse, Bangalore, NIMHANS Publication, 227-236.
- Mukundan, C. R. (1997). On mind, memory and brain. Indian Journal of Clinical Psychology, 24, 103-112.
- Sperry, R. W. (1950). Neural basis of the spontaneous optokinetic response produced by visual inversion. Journal of comparative and physiological psychology, 43(6), 482-489.
- Baddeley, A., & Hitch, G. (1974). Baddeley's model of working memory.
- Baddeley, A. (1986). Working memory (vol. 11).
- Troyer, A.K., & Craik, F.I. (2000). The effect of divided attention on memory for items and their context. Canadian Journal of Experimental Psychology/Revue canadienne de psychology experimentale , 54 (3), 161-171.
- Troyer, A. K., Winocur, G., Craik, F. I., & Moscovitch, M. (1999). Source memory and divided attention: reciprocal costs to primary and secondary tasks. Neuropsychology, 13(4), 467- 473.
- Smith, E. E., & Jonides, J. (1998). Neuroimaging analyses of human working memory. Proceedings of the National Academy of Sciences, 95(20), 12061-12068.
- Smith, E. E., & Jonides, J. (1999). Storage and executive processes in the frontal lobes. Science, 283(5408), 1657-1661.
- Cohen, J. D., Perlstein, W. M., Braver, T. S., Nystrom, L. E., Noll, D. C., Jonides, J., & Smith, E. E. (1997). Temporal dynamics of brain activation during a working memory task. Nature, 386(6625), 604-608.
- Andreasen, N. C., O'Leary, D. S., Arndt, S., Cizadlo, T.,Hurtig, R., Rezai, K., ... & Hichwa, R. D. (1995). Short- term and long-term verbal memory: a positron emission tomography study. Proceedings of the National Academy of Sciences, 92(11), 5111-5115.
- Squire, L. R., Ojemann, J. G., Miezin, F. M., Petersen, S. E., Videen, T. O., & Raichle, M. E. (1992). Activation of the hippocampus in normal humans: a functional anatomical study of memory. Proceedings of the National Academy of Sciences, 89(5), 1837-1841.
- Buckner, R. L., Kelley, W. M., & Petersen, S. E. (1999). Frontal cortex contributes to human memory formation. Nature neuroscience, 2(4), 311-314.
- Borod, J. C., Cicero, B. A., Obler, L. K., Welkowitz, J.,Erhan, H. M., Santschi, C., ... & Whalen, J. R. (1998). Right hemisphere emotional perception: evidence across multiple channels. Neuropsychology, 12(3), 446-458.
- Joseph, J. (2001). Is crime in the genes? A critical review of twin and adoption studies of criminality and antisocial behavior. The journal of mind and behavior, 179-218.
- Morley, K. I., & Hall, W. D. (2003). Is there a genetic susceptibility to engage in criminal acts? Trends & Issues in Crime & Criminal Justice, (263), 1-6.
- Lowenstein, L. F. (2004). The genetic aspects of criminality. Journal of human behavior in the social environment, 8(1), 63-78.
- Tehrani, J. A., & Mednick, S. A. (2000). Genetic Factors and Criminal Behaviors. Fed. Probation, 64, 24.
- Dalton, A. L., & Daneman, M. (2006). Social suggestibility to central and peripheral misinformation. Memory, 14(4), 486- 501.
- Ruchkin, D. S., Canoune, H. L., Johnson Jr, R., & Ritter,W. (1995). Working memory and preparation elicit different patterns of slow wave eventâ?related brain potentials. Psychophysiology, 32(4), 399-410.
- Ruchkin, D. S., Johnson Jr, R., Grafman, J., Canoune, H., & Ritter, W. (1992). Distinctions and similarities among working memory processes: An event-related potential study. Cognitive Brain Research, 1(1), 53-66.
- Owen, A. M., Downes, J. J., Sahakian, B. J., Polkey, C. E., & Robbins, T. W. (1990). Planning and spatial working memory following frontal lobe lesions in man. Neuropsychologia, 28(10), 1021-1034.
- Jonides, J., Smith, E. E., Koeppe, R. A., Awh, E., Minoshima, S., & Mintun, M. A. (1993). Spatial working memory in humans as revealed by PET. Nature, 363(6430), 623-625.
- Jonides, J., Schumacher, E. H., Smith, E. E., Koeppe, R. A.,Awh, E., Reuter-Lorenz, P. A., ... & Willis, C. R. (1998). The role of parietal cortex in verbal working memory. Journal of neuroscience, 18(13), 5026-5034.
- Tulving, E., Kapur, S., Craik, F. I., Moscovitch, M., & Houle,S. (1994). Hemispheric encoding/retrieval asymmetry in episodic memory: positron emission tomography findings. Proceedings of the National Academy of Sciences, 91(6), 2016-2020.
- Tulving, E., Kapur, S., Markowitsch, H. J., Craik, F. I., Habib, R., & Houle, S. (1994). Neuroanatomical correlates of retrieval in episodic memory: auditory sentence recognition. Proceedings of the National Academy of Sciences, 91(6), 2012-2015.
- Henson, R. N. A., Shallice, T., & Dolan, R. J. (1999). Right prefrontal cortex and episodic memory retrieval: a functional MRI test of the monitoring hypothesis. Brain, 122(7), 1367- 1381.
- Stevens, A. A. (2004). Dissociating the cortical basis of memory for voices, words and tones. Cognitive Brain Research, 18(2), 162-171.
- Shallice, T., Fletcher, P., Frith, C. D., Grasby, P., Frackowiak,R. S., & Dolan, R. J. (1994). Brain regions associated with acquisition and retrieval of verbal episodic memory. Nature, 368(6472), 633-635.
- Kapur, S., Craik, F. I. M., Jones, C., Brown, G. M., Houle, S., & Tulving, E. (1995). Functional role of the prefrontal cortex in retrieval of memories: A PET study. Neuroreport: An International Journal for the Rapid Communication of Research in Neuroscience, 6 (14), 1880–1884.
- Kapur, S., Rose, R., Liddle, P. F., Zipursky, R. B., Brown, G. M., Stuss, D., ... & Tulving, E. (1994). The role of the left prefrontal cortex in verbal processing: semantic processing or willed action? Neuroreport, 5(16), 2193-2196.
- Fletcher, P. C., Shallice, T., & Dolan, R. J. (1998). The functional roles of prefrontal cortex in episodic memory. I. Encoding. Brain: a journal of neurology, 121(7), 1239-1248.
- Fletcher, P. C., Shallice, T., Frith, C. D., Frackowiak, R. S., & Dolan, R. J. (1998). The functional roles of prefrontal cortex in episodic memory. II. Retrieval. Brain: a journal of neurology, 121(7), 1249-1256.
- Cabeza, R., Prince, S. E., Daselaar, S. M., Greenberg, D. L., Budde, M., Dolcos, F., ... & Rubin, D. C. (2004). Brain activity during episodic retrieval of autobiographical and laboratory events: an fMRI study using a novel photo paradigm. Journal of cognitive neuroscience, 16(9), 1583-1594.
- Wickelgren, I. (1997). Cognitive Neuroscience: Getting a Grasp on Working Memory. Science, 275(5306), 1580-1580.