




Case Report - (2023) Volume 2, Issue 1
Bouveret Syndrome : The Rare Challenging Case of the Day
2Surgical Department B, CHARLES NICOLLE Hospital, Tunis, Tunis,, Tunisia
Received Date: Jun 06, 2023 / Accepted Date: Jul 20, 2023 / Published Date: Jul 25, 2023
Copyright: ©Â©2023 Sabrine Soua, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Soua, S., Ghanem, M., Abdesselem, M. M., Bouali, M. R. (2023). Bouveret Syndrome: The Rare Challenging Case of the Day. J Surg Care, 2(1), 44-46.
Abstract
Bouveret syndrome is an extremely rare disease. We report the case of a 54-year-old man who presented to our department with acute vomiting. An upper digestive endoscopy was first done, revealing an enclaved gallstone in the second duodenum. Cross- sectional imaging was then performed to confirm the correct diagnosis of Bouveret's syndrome. Through a medline incision, cholecystectomy and extraction of the gallstone were done and the patient was discharged seven days after the operation with a good clinical outcome.
Keywords
Bouveret Syndrome, Gallstone Ileus, Pneumobilia, Surgical Treatment
Introduction
During clinical practice, complications related to cholelithiasis such as pancreatitis, cholecystitis, common bile duct lithiasis, and gallstone ileus are not uncommon [1] . During gallstone il-eus, the stone is often blocked at the level of the terminal ileum and the ileocecal valve. The impaction of the calculus at the level of the distal stomach or the proximal part of the duodenum fol¬lowing a passage via a cholecysto-duodenal, cholecysto-bulbar or cholecysto-gastric fistula defines Bouveret syndrome (BS). It’s a rare biliary complication with high mortality [2]. Given the rarity of the pathology, diagnostic and therapeutic management are not well standardized. We wrote this paper to review current literature highlighting the pathogenesis and management of the disease.
Case Report
A 54-year old male presented with acute vomiting and abdomi¬nal pain. His previous history was consistent with a diagnosis of acute necrotizing pancreatitis one year ago. Physical examina¬tion showed tenderness in the epigastric region and right upper quadrant without clinical signs of dehydration. The white blood cell count was 7.200/mm3 and the CRP was 30 mg/dL. The renal function was normal with no hydroelectrolytic disorder. Total bilirubin and alkaline phosphatase were normal. Lipasemia was normal. In front of this clinical presentation, an upper gastroin¬testinal endoscopy was performed first and showed an obstacle in the second duodenum (shown in Fig. 1).

Figure 1: Ensdocopic view of the stone enclaved in the second duodenum before (A) and after washing (B)
Abdominal magnetic resonance imaging (MRI) revealed an enclaved gallstone of three centimeters in the second duodenum (shown in Fig. 2A), gastric distension (shown in Fig. 2B), cholecystoduodenal fistula, and pneumobilia (shown in Fig. 2C).
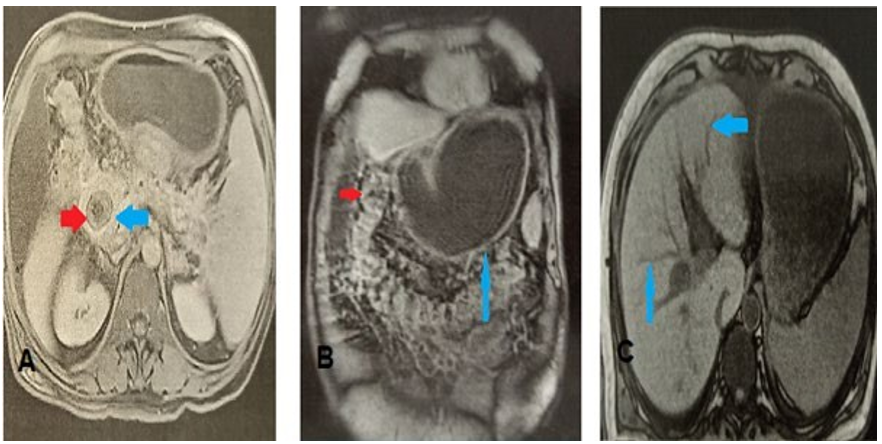
Figure 2: MRI images (A) Axial MRI slide, sequence T2, at the portal phase, showing the stone enclaved in the second duodenum(B) Coronal section of abdominal MRI T2 sequence showing gastric distension upstream of the calculus. (C) In-phase abdominal axial slide showing pneumobilia
Based on radiologic findings, the diagnosis of BS was made. Through a medline incision, cholecystectomy and extraction of the gallstone (shown in Fig. 3) were done.

Figure 3: Iconography of calculus after surgical extraction
Faced with the significant inflammatory reaction around the du¬odenum and the presence of a large fistula, we performed a duodenostomy, pyloric exclusion, and gastro-jejunal anastomosis. The patient was discharged seven days after the operation with a good clinical outcome. The duodenostomy tube was removed one month later. During 12 months of follow-up, the patient was symptom free.
Discussion
Bouveret syndrome is a rare complication of cholelithiasis. It was first described by a Parisian internist, Leon Bouveret, in 1896 [3]. Subsequently, only 315 cases were reported between 1967 and 2016. This rare pathology most often affects elderly subjects with several comorbidities and is burdened with a high mortality rate of 12 to 30% [4]. The main risk factors for the de¬velopment of BS are: cholelithiasis, female gender, age over 60 years, and stones larger than 20 mm [5]. Our clinical case is par¬ticularly marked by the young age and the absence of comorbid¬ities. The pathophysiology of Bouveret syndrome is explained by the development of adhesions between the gallbladder and a close segment of the upper digestive tract following recurrent episodes of cholecystitis [6].
Furthermore, the huge stone's pressure induces necrosis, which leads to a bilio-digestive fistula. The most frequent type of fis-tula is a cholecysto-duodenal fistula, while cholecysto-gastric fistulas are less common. The stones at the origin of Bouveret syndrome have, in the majority of cases, a size greater than 25 mm [5]. The clinical presentation is not specific. BS can cause nausea, vomiting, abdominal pain, weight loss, anorexia, or gas-tric outlet obstruction [1]. Oesogastroduodenal endoscopy is generally the first examination to be performed. It may show gastric distension and a blocked stone at the level of the distal part of the stomach or the proximal part of the duodenum. How¬ever, the calculus is only found on endoscopy in 69% of cases. This can be explained by the food impaction upstream of the gallstone. For the biliodigestive fistula, it is only found in 13% of cases on endoscopy [7].
Ultrasonography, computed tomography (CT), and MRI are helpful examinations in diagnosis. Abdominal CT is a good test for the diagnosis of Bouveret syndrome with high sensitivity and specificity. MRI is especially interesting for better visualization of the biliary tract and for the diagnosis of isodense gallstones on the CT [8]. In our presented case, MRI was superior to com-puted tomography in the study of the biliary tree before surgical treatment. Several surgical and non-surgical treatment options have been described for BS. For non-surgical methods, we find endoscopic extraction of the stone and other techniques aimed at fragmenting the stone, such as endoscopic lithotripsy, elec¬tro-hydraulic lithotripsy, endoscopic laser lithotripsy, and extra-corporeal lithotripsy [9]. A study showed that these techniques were ineffective in 42% of cases [10]. The main limitations of endoscopic treatment are: the migration of stone fragments with the risk of distant gallstone ileus; the impossibility of repairing the fistula; the size of the stone; and the operator's experience [11]. Not to mention that the gallstone is not found on endoscopy in 30% of cases. Therefore, surgical treatment remains a refer¬ence for BS to this day. Surgical management is based on stone extraction, fistula repair, and cholecystectomy.
It can be performed in one or two steps. For the elderly with comorbidities, the two-step procedure is safer. The one-step procedure is more commonly used in young patients. Recently, with the extensive application of laparoscopy, the laparoscopic approach has become a safe and effective alternative to open surgery [12]. Cases of BS reported with duodenum exclusion and gastro-jejunal anastomosis are rare and have been mostly described in cases of unrepairable duodenal lesions or difficult localization of the gallstone, particularly at the level of D2/D3 [13]. The occurrence of Bouveret's syndrome in a young patient without comorbidities and the success of surgical treatment by gastrojejunal anastomosis, which is a rarely reported technique, makes our case original.
Conclusion
Bouveret syndrome is a rare but scary complication of gallstones. Therefore, knowledge of its risk factors, symptoms, radiological and endoscopic findings is important for a rapid diagnosis to minimize morbidity and mortality. Treatment is based on sur¬gery. However, endoscopic treatment remains promising and needs to be improved, especially for such vulnerable patients.
Funding : None.
Conflict of Interest : None declared.
Ethical Statement
Written informed consent was obtained from the patient for pub-lication of this case report and any accompanying images.
References
- Caldwell, K. M., Lee, S. J., Leggett, P. L., Bajwa, K. S., Mehta, S. S., & Shah, S. K. (2018). Bouveret syndrome: current management strategies. Clinical and experimental gastroenterology, 69-75.
- Khaira, H. S., & Thomas, D. R. (1994). Gallstone emesis and ileus caused by common hepatic duct-duodenal fistula. Journal of British Surgery, 81(5), 723-723.
- Puri, V., Lee, R. W., Amirlak, B. A., Lanspa, S. J., & Fitzgib-bons Jr, R. J. (2007). Bouveret syndrome and gallstone ileus. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 17(4), 328-330.
- Patel, A., & Agarwal, S. (2014). The yellow brick road of Bouveret syndrome. Clinical Gastroenterology and Hepatology, 12(8), A24.
- Turner, A. R., Kudaravalli, P., Al-Musawi, J. H., & Ahmad,H. (2022). Bouveret Syndrome (Bilioduodenal Fistula). In StatPearls [Internet]. StatPearls Publishing.
- Nickel, F., Müller-Eschner, M. M., Chu, J., von Tengg-Kobligk, H., & Müller-Stich, B. P. (2013). Bouveret’s syndrome: presentation of two cases with review of the literature and development of a surgical treatment strategy. BMC surgery, 13, 1-7.
- Sadovnikov, I., Anthony, M., Mushtaq, R., Khreiss, M., Gavi-ni, H., & Arif-Tiwari, H. (2021). Role of magnetic resonance imaging in Bouveret's syndrome: A case report with review of the literature. Clinical Imaging, 77, 43-47.
- Algin, O., Ozmen, E., Metin, M. R., Ersoy, P. E., & Karaogla-noglu, M. (2013). Bouveret syndrome: evaluation with mul-tidetector computed tomography and contrast-enhanced magnetic resonance cholangiopancreatography. Ulus Travma Acil Cerrahi Derg, 19(4), 375-379.
- Dumonceau, J. M., & Devière, J. (2016). Novel treatment options for Bouveret’s syndrome: a comprehensive review of 61 cases of successful endoscopic treatment. Expert Review of Gastroenterology & Hepatology, 10(11), 1245-1255.
- Mavroeidis, V. K., Matthioudakis, D. I., Economou, N. K., & Karanikas, I. D. (2013). Bouveret syndrome—the rarest variant of gallstone ileus: a case report and literature review. Case Reports in Surgery, 2013.
- Cappell, M. S., & Davis, M. (2006). Characterization of Bouveret's syndrome: a comprehensive review of 128 cases. Official journal of the American College of Gastroenterology| ACG, 101(9), 2139-2146.
- Kudaravalli, P., Saleem, S. A., Goodman, A., Pendela, V. S., & Arif, M. O. (2020, April). Bouveret syndrome as a rare cause of gastric outlet obstruction. In Baylor University Medical Center Proceedings (Vol. 33, No. 2, pp. 235-236). Taylor & Francis.
- Kostakis, I. D., Garoufalia, Z., Feretis, T., Kykalos, S., & Mantas, D. (2017). A case of Bouveret’s syndrome treated with gastrojejunal anastomosis. Journal of Surgical Case Reports, 2017(10), rjx213.