
New Advances in Brain & Critical Care(NABCC)
ISSN: 2771-7887 | DOI: 10.33140/NABCC
Impact Factor: 1.01



Case Report - (2025) Volume 6, Issue 1
Bilateral Sub Dural Haemorrhage (SDH) with Sepsis Due to Citobacter Koseri Mimicking Stroke
#Equally contribution
Received Date: Oct 23, 2024 / Accepted Date: Dec 05, 2024 / Published Date: Jan 03, 2025
Copyright: ©©2025 Preeti Singh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Singh, P., Patel, H., Kumar, A. (2025). Bilateral Sub Dural Haemorrhage (SDH) with Sepsis Due to Citobacter Koseri Mimicking Stroke. New Adv Brain & Critical Care, 6(1), 01-04.
Abstract
Intracranial infections after craniotomies are an important complication of treatment in neurosurgery, especially in elderly patients that are already immunologically compromised resulting in longer treatment with antibiotics, additional surgical procedures, poorer treatment outcomes and prolonged management of primary pathology due to active infection. We report one such operated case of bilateral SDH with sepsis due to citrobacter koseri presenting with stroke like symptoms.
Keywords
Intracranial, Immunologically, Sepsis, Citobacter Koseri
Abbreviations
CNS: Central Nervous System
CPR: Cardiopulmonary Resuscitation
CT: Computed Tomography
DM: Diabetes Mellitus
IHD: Ischemic Heart Disease
MRI: Magnetic Resonance Imaging
SDH: Sub Dural Haemorrhage
Introduction
Citrobacter Koseri is a commensal organism found in air, water, soil, occasional colonizer of human and animal gastrointestinal tract. Early diagnosis and treatment are crucial in CNS infections. Etiological diagnosis can be extremely challenging in immunocompromised patients, as the effects of the infection combine with those of the underlying disease. Clinical manifestation in such cases is diverse and usually unspecific. We present a case of a 70-year male, background of hypertension, IHD, DM diagnosed with bilateral SDH and was operated for same. However, during hospital stay, patient developed sudden of left sided weakness and slurring of speech, he was initially diagnosed as a case of stroke but further evaluation showed CNS Citrobacter Koseri infection mimicking the symptoms of stroke.
Case Report
A 70-year male, background of hypertension, IHD, DM on blood thinner medications presented in Department of Neurosurgery with severe headache for 2 days. Routine blood investigations were normal. Neurological examination revealed mild right sided pronator drift. CT Brain showed bilateral acute subdural hematomas (R>L). Patient was started on iv antiepileptics, analgesics and anti- oedema drugs. Blood thinner medication was stopped and opinion from cardiologist was taken for the same. 2D echo done showed 55% EF. After 4 days of conservative management repeat CT Brain was done which showed decrease in SDH. However, on day 6 patient had sudden onset of left sided weakness and slurring of speech. Code purple was activated and MRI Brain was urgently done considering the possibility of stroke. However, MRI Brain done showed no signs of stroke and increase in SDH with 10 mm midline shift.
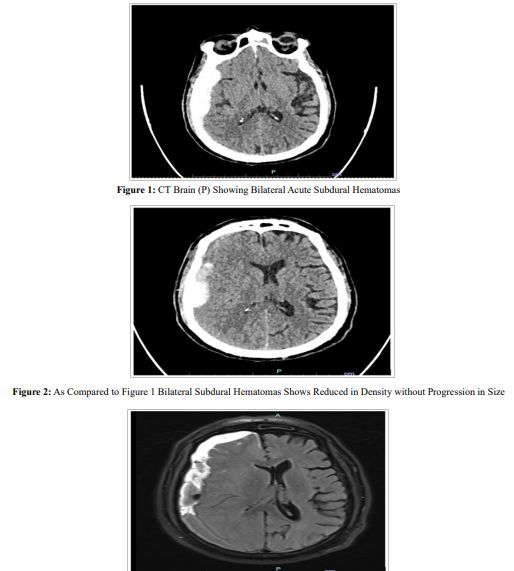
Figure 3: MRI Brain Showed Increase in Size of the Right Cerebral Convexity Subdural Hematoma with Interval Increase in the Midline Shift (Now 10 mm to the Left)
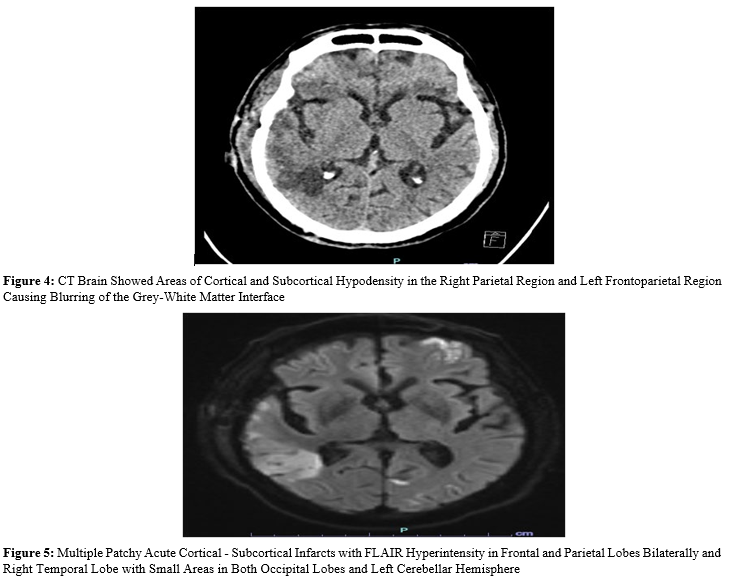
Patient underwent right FTP mini craniotomy and clot evacuation. On post-operative day 2 patient had a seizure and hyponatremia with serum Na 127 meq/L which was managed conservatively. On post-operative day 6 patient developed severe sepsis and was electively intubated due to breathing difficulty. Patient developed transient hemiparesis lasting for 24 hours. CT Brain done showed multiple hypodensity areas in frontal, temporal and parietal region. MRI Brain revealed acute cortical - subcortical infarcts in frontal and parietal lobes bilaterally and right temporal lobe with small areas in both occipital lobes and left cerebellar hemisphere.
MR Angiogram showed normal circle of Willis vessels. No signs of arterial occlusion. MR Venograms showed no Dural venous sinus thrombosis. Echocardiography (LVEF 50%). LP was done. CSF showed raised count 1000 leukocytes (85% polymorphs), 1 mg/ dl glucose and 400 mg/dl proteins. CSF culture grew citrobacter koseri. Systemic cultures were sent. Patient was started on iv meropenem. On postoperative day 10. Patient had a asystole for which CPR was given. Patient was revived. Patient was continued on antibiotics. Patient underwent tracheostomy and was slowly weaned off from the ventilatory support and discharged.
Discussion
Citrobacter koseri, formerly known as Citrobacter divers us, is a Gram-negative non-spore forming, rod-shaped bacterium. It is a facultative anaerobe capable of aerobic respiration. It is motile via peritrichous flagella [1]. The members of this family are part of the normal flora and commonly found in the digestive tracts of humans and animals [2]. C koseri may act as an opportunistic pathogen in individuals who are immunocompromised mainly occurs as hospital-acquired infections [3]. Infections caused by C. koseri can lead to various symptoms, including fever, chills, diarrhoea, and abdominal pain. In severe cases, the bacterium can cause sepsis, meningitis, or brain abscesses [4]. Arterial and venous infarctions are possible because of the bacterial infiltration along the main vessel; exudates within the ventricles and ventriculitis may obstruct the ventricular foramina and result in multi-cystic hydrocephalus with consequent long-lasting shunting difficulties and necrotizing meningoencephalitis with pneumocephalus has been reported [5].
Early and massive tissue necrosis is a specific feature of C. koseri brain infection. The early stage of the disease predominates in the white matter, causing cerebritis; the later stage is marked with necrotic cavities in multiple locations. In samples collected from cerebrospinal fluid, C. koseri grows well on any ordinary medium; they produce unpigmented, colourless mucoid colonies. If incubated for 24 hours in other media such as indole, citrate, and adonitol, C. koseri will be positive, hydrogen sulphide negative in Kligers’ iron agar, and negative results in lactose, silicon, and sucrose broth as well [6]. A broad spectrum cephalosporin and meropenem are often used because of the good penetration into the central nervous system [7,8]. The prognosis of the C. koseri infection is 20 to 30% of neonates die, and 75% of survivors have significant neurologic damage such as complex hydrocephalus, neurologic deficits, mental delay, and epilepsy [5].
Conclusion
Early diagnosis and treatment are crucial in CNS infections. Etiological diagnosis can be extremely challenging in immunocompromised patients, as the effects of the infection combine with those of the underlying disease. Stroke as a neurosurgical postoperative complication is relatively common with cerebrovascular disease frequently appearing as an underlying condition. Stroke mimics are common. Around a quarter of patients initially suspected to have a stroke are subsequently found to have an alternative diagnosis. Possibility of active infection should be considered while dealing with stroke like presentation.
References
- Ong, C. L. Y., Beatson, S. A., Totsika, M., Forestier, C., McEwan, A. G., & Schembri, M. A. (2010). Molecular analysis of type 3 fimbrial genes from Escherichia coli, Klebsiella and Citrobacter species. BMC microbiology, 10, 1-12.
- Species Citrobacter koseri. (2023). LPSN.
- Pennington, K., Van Zyl, M., & Escalante, P. (2016). Citrobacter koseri pneumonia as initial presentation of underlying pulmonary adenocarcinoma. Clinical Medicine Insights: Case Reports, 9, CCRep-S40616.
- Greenwood, D., Slack, R. C. B., Peutherer, J. F., Barer, M.R. (2007). Medical Microbiology: A Guide to Microbial Infections: Pathogenesis, Immunity, Laboratory Diagnosis and Control. Elsevier, 1264-1266.
- Babyn, P. S. (2011). Section I: Neuroradiology: Case 3. Teaching Atlas of Pediatric Imaging. Thieme, 44-47.
- Doran, T. I. (1999). The role of Citrobacter in clinical disease of children. Clinical infectious diseases, 28(2), 384-394.
- Feferbaum, R., Diniz, E., Valente, M., Giolo, C. R., Vieira,R. A., Galvani, A. L., ... & Vaz, F. A. (2000). Brain abscess by citrobacter diversus in infancy: case report. Arquivos de Neuro-Psiquiatria, 58, 736-740.
- McPherson, C., Gal, P., & Ransom, J. L. (2008). Treatment of Citrobacter kosen Infection with Ciprofloxacin and Cefotaxime in a Preterm Infant. Annals of Pharmacotherapy, 42(7-8), 1134-1138