
Toxicology and Applied Pharmacology Insights(TAPI)
ISSN: 2641-0451 | DOI: 10.33140/TAPI

Research Article - (2020) Volume 3, Issue 1
Basal Cell Adenoma: About Four Cases
2Otolaryngology Service, Morocco
3Radiology Service, Morocco
Received Date: Aug 08, 2019 / Accepted Date: Aug 28, 2019 / Published Date: Jan 13, 2020
Copyright: ©Copyright: ©2020 Imane Boujguenna, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Benign tumor of the salivary glands, composed of basaloid cells of architecture most often ductal and tubular or in nests (OMS 2017). We report the case of 4 patients carrying basal cell adenoma diagnosed at the department of pathological anatomy CHU MOHAMMED VI MARRAKECH. These are three women and one man. The average age was 49 years old. The clinical examination found a unilateral parotid mass gradually increasing in size. All the patients benefited from an ultrasound which was in favor of a homogeneous hypoechoic lobulated formation with posterior reinforcement evoking a pleomorphic adenoma. The patients benefited from a total parotidectomy. Macroscopic examination found a thick-walled, hemorrhagic-cystic formation in one patient. Microscopic examination showed a benign encapsulated tumor proliferation of compact architecture, in situ clusters and in channels with eosinophilic contents. . The epithelial cells have a basaloid appearance bordered at the periphery by a palisade cell base. They are of small to medium size, provided with ovoid cores with fine chromatin. The cytoplasm is abundant basophilic. The myoepithelial cells are sometimes cuboid, sometimes fusiform. The nuclei are discreetly elongated hyperchromic. The cytoplasm is scarce eosinophilic.The basal cell adenoma is a rare salivary tumor representing less than 3.7%. It occurs mainly in the elderly with a range of 57 to 70 years. Clinically, it is in most cases a mobile solitary mass of firm consistency. The tumor has a monomorphic appearance due to the predominance of basaloid cells. The differential diagnosis is primarily with basal cell adenocarcinoma and adenoid cystic carcinoma.
Keywords
Basal cell adenoma is a benign tumor characterized by a proliferation of basaloid cells, mostly canalar and tubular or in nests (WHO 2017) and the absence of myxochondroid stroma characteristic of the pleomorphic adenoma [1, 2].
Material and methods
We report the case of 4 patients with basal cell adenoma diagnosed at the department of pathological anatomy CHU MOHAMMED VI MARRAKECH.
Results
It's about three women and a man. The average age was 49 years old. Clinical examination found a unilateral parotid mass gradually increasing in size (Table 1).
Table 1: Age and Clinical Examination
|
Observations |
Case 1 |
Case 2 |
Case 3 |
Case 4 |
|
Age |
F: 40years old |
H: 42 years old |
F: 42 years old |
F:72 years old |
|
Clinical examination |
Unilateral parotidus mass gradually increasing in size |
|||
|
Mass of firm consistency painful to palpation |
Solitary mass, firm, mobile and painless |
|||
All patients underwent ultrasonography which favored a homogeneous hypoechoic, polyhedogenic formation with posterior reinforcement evoking a pleomorphic adenoma (Table 2) (Figure 1).
Table 2: Radiological Examinations
|
Observations |
Case 1 |
Case 2 |
Case 3 |
Case 4 |
|
Echography |
Intraparotidin formation well-limited homogeneous hypoechoic |
|||
|
Scanner |
CT Rounded and well-rounded intraparotid nodule formation, homogeneously enhanced after injection of PDC - |
- |
||
|
MRI |
_ |
|
|
Intraparotid image encapsulated in hyposignal in T1 and hypersignal in T2 without locoregional infiltration |
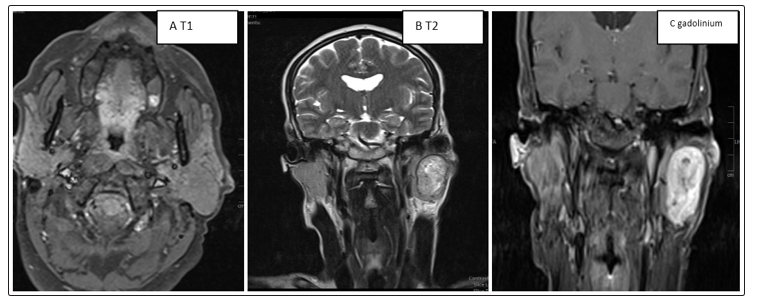
Figure 1: (A, B, C): Intraparotid image encapsulated in hyposignal in T1 and hypersignal in T2
Patients underwent total parotidectomy. The macroscopic examination found a thick-walled cystic formation with hemorrhagic contents in one patient (Table 3).
Table 3: Macroscopic Examination
|
Observations |
Cas 1 |
Cas 2 |
Cas 3 |
Cas 4 |
|
Matérials |
Parotidectomy Piece: Fragmented Material |
|||
|
Macroscopy |
|
-Thick wall
|
||
- Microscopic examination showed a benign tumor proliferation encapsulated compact architecture, in situ clusters and channels with eosinophilic content. The epithelial cells have a basaloid appearance bordered at the periphery by a palisade cell base. They are of small to medium size, provided with ovoid cores with fine chromatin. The cytoplasm is abundant basophilic. The myoepithelial cells are sometimes cuboid, sometimes fusiform. The nuclei are discreetly elongated hyperchromic. The cytoplasm is scarce eosinophilic (Figures 2, 3, 4). The massive elm form (3 cases) and the menbranous form (1 case)
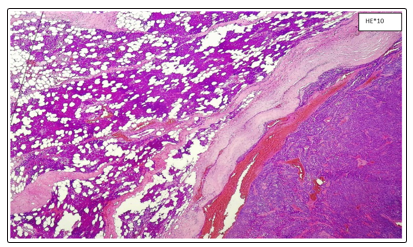
Figure 2: Parotid Salivary Parenchyma With Well-Limited Tumor Proliferation Encapsulated
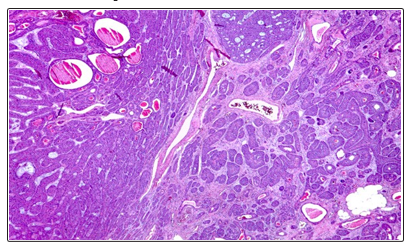
Figure 3: Encapsulated Benign Tumor Proliferation Of Compact Architecture, In Situ Clusters And In Channels With Eosinophic Content
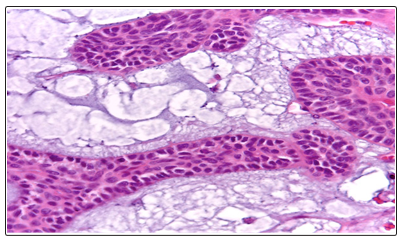
Figure 4: The epithelial cells have a basaloid appearance bordered at the periphery by a palisade cell base
The cells are small to medium in size, with ovoid nuclei of fine chromatin. The cytoplasm is abundant basophilic. The myoepithelial cells are sometimes cuboid, sometimes fusiform. The nuclei are discreetly elongated hyperchromic. Cytoplasm is scarce eosinophilic
Discussion
It is a benign epithelial tumor composed mainly of basaloid cells. The demarcation between the epithelial proliferation and the tumor stroma is very clear and the tumor is devoid of the chondromyxoid tissue characteristic of the pleomorphic adenoma. Depending on the architectural organization, there are several types: massive, trabecular, tubular or membranous. The incidence: 1.5% of salivary gland tumors and 2.4% of benign tumors. The parotid in 75% of cases and the upper lip in 8% of cases. The average age is 58 years old. There is a female predominance. Membrane-type basal cell adenomas are sometimes associated with the presence of an adnexal skin tumor. It is most often a cutaneous cylindroma, but other tumors have been described: trichoepithelioma, trichilemmome, eccrine spiradenoma [1-4]. Macroscopically it is a single nodule well limited, "encapsulated" unfixed and measuring less than 3cm with sometimes cystic reworkings. The membranous architectural type is usually poorly limited and multifocal. Histologically: the aspect is monomorphic by the predominance of basaloid cells [1,5-11]. These are small round cells with round or oval nuclei and pale and poorly limited cytoplasm, which may correspond either to true basal cells or to ductal or myoepithelial cells. The term basaloid allows to group these different cell types that can not easily be distinguished without immunohistochemistry. Two morphological types of basaloid cells are described: Dark basaloid cells have a hyperchromatic nucleus and a scanty cytoplasm. They are arranged in a palissadic manner on the periphery of the massifs. The light basaloid cells have a pale nucleus and abundant cytoplasm. They are located in the center of the massifs. There are also some ductal cells that form small glandular lumens, especially in the tubular type. In the massive type. The cells can be grouped in massive, in large more or less anastomotic trabeculae, in nodules of big size or small size (architecture of insular type). The stroma is dense collagenous. There may be areas of squamous metaplasia sometimes incomplete (swirls) or mature (horny globes). Cystic changes are common especially at the subcapsular level.The trabecular type characterized by cells that form thin anastomotic trabeculae in a loose stroma. The palisade appearance of dark basaloid cells is less marked than in the massive type. There are in some cases many cystic duct formations more or less cystic. It is this form that raises a problem of differential diagnosis with ductal adenoma. The membranous type is made of thick PAS + hyaline strips that surround each cellar, which gives a low magnification a puzzle appearance. These bands correspond to an excessive production of basement membrane. The hyaline material can also be observed in intercellular situation in the form of hyaline balls P AS + more or less coalescent. These aspects may during extemporaneous examination evoke adenoid cystic carcinoma.
Most often, several types of architecture are represented in the same tumor, which is then classified according to the predominant architectural mode. It is especially important to distinguish the membranous type from other architectural types because it involves an association with skin tumors and a poor prognosis.
The use of immunohistochemistry is not systematic [12-14]: The antibodies that can be used are:
• Cytokeratin: constant positivity but the number of labeled cells is very variable.
• Anti-actin, anti-PS-100 and anti-vimentin: positivity in most basal cell adenomas, in the basaloid cells located at the periphery of the massifs.
• Anti-EMA and anti-ACE mark small ductal formations.
• Anti-myosin and anti-GFAP sometimes mark a few cells.
• The differential diagnosis is done with [1,6,7,13, 14]:
• Basal cell carcinoma
• If the skin is infiltrated or very close to the basal cell adenoma, the latter may be confused with basal cell carcinoma.
• Adenoid cystic carcinoma
The predominance of basaloid cells in massive cystic adenoid carcinoma, and conversely, focal cribriform features or basement membrane accumulation in basal cell adenomas may make the differential diagnosis difficult. The following criteria must be used
|
|
Adenoma with basal cells |
Adenoid cystic carcinoma |
|
Limitation |
Good limitation |
Macroscopic infiltration |
|
|
encapsulation |
|
|
Nerve infiltration |
No |
Frequent |
|
Cribriform architecture |
Rare and focale |
Frequent |
|
Anisokaryosis |
No |
Yes |
|
Form of nucleus |
Rounded |
Angular |
|
Clair cells |
No |
Yes |
|
Squamous metaplasia |
Yes |
No |
|
Necrosis |
Rare |
Frequent |
• Basal cell adenocarcinoma
A mitotic activity greater than 3 mitoses per 10 fields is very suspect, but it is the infiltrating character (involvement of adipose, muscular, cutaneous or bone tissue, nerve or vascular infiltration) which indicates the malignancy of this lesion.
• Adenoma Pleomorph in its cellular variant
Epithelial masses that characterize the pleomorphic adenoma. A strong expression of GFAP is also in favor of a pleomorphic adenoma. A weak expression of GFAP brings no element for the differential diagnosis.
• Canalicular adenoma
|
|
Adenoma with basal cells |
Ductal adenoma |
|
Site |
Parotid (75%) |
Upper lip (75%) |
|
|
Upper lip (6%) |
Oral mucosa (12%) |
|
|
Submaxillary (5%) |
|
|
Age |
58 years old |
65 years old (adult only) |
|
Association |
Similarity and association with |
None |
|
(ou diathesis) |
eccrine skin tumors and cylindroma |
|
|
|
« dermal analoge tumor » |
|
|
Cells |
Basaloïd |
Cylindrical |
|
Stroma |
Most often dense |
Little visible finely fibrillary Very richly vascularized |
Except for the membranous type, recurrences are extremely rare. Total excision of the lesion is therefore performed in a conservative manner. The membranous type is to individualize other types. It recurs in 25% of cases and undergoes carcinomatous transformation in 28% of cases against 4% for other types of architecture. This transformation most often corresponds to basal cell adenocarcinoma,but it may also be another tumor type. In addition there is an association with cutaneous tumors (cylindrome +++).
Pleomorphic adenomas, basal cell adenomas and myoepitheliomas x are part of the same tumor spectrum. There are forms of passage between epithelial and myopithelial cells making their immunohistochemical distinction sometimes difficult [1,3,14].
Conclusion
The basal cell adenoma is a rare benign tumor of the salivary glands often reaching the parotid. It is differentiated from basal cell adenocarcinoma by several histological criteria, especially when the clinical presentation is also ambiguous. Management requires good anatomo-clinical correlation.
References
- Histoseminaire Carrefour Pathologie (2017) http://www. sfpathol.org/histoseminaires-2017.html
- BARNES L, EVERSON JW, REICHART P, SIDRANSKY D(2005) DE ARAUJO VC. Basal cell adenoma. In; eds. World Health Organization Classification of Tumors. Pathology and genetics of Head and Neck Tumours. Lyon: IARC Press 9: 261-2.
- Daley TD, Gardner DG, Smuot MS (1984) Canalicular adenoma: not a basal cell adenoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 57: 181-7.
- Yu GY, Ubmuller J, Donath K (1998) Membranous basal cell adenoma of the salivary gland: a clinicopathologic study of 12 cases. Acta Otolaryngol 118: 588-93.
- Nagao T, Sugano I, Ishida Y, et al. (1998) Basal Cell Adenocarcinoma of the Salivary Glands. Comparison with Basal Cell Adenoma through Assessment of Cell Proliferation, Apoptosis, and Expression of p53 and bcl-2. Cancer 82: 439-47
- Querioz LMG, Da Silveira EJD, Arruda MLS, Ramos CCF (2004) A rare salivary gland neoplasm: multiple canalicular adenoma. A case report. Auris Nasus Larynx 31: 189-93.
- Gardner DG, Daley TD (1983) The use of the terms monomorphic adenoma, basal cell adenoma, and canalicular cell adenoma as applied to salivary gland tumors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 56: 608-15.
- Batsakis JG (1991) Oral monomorphic adenomas. Ann Otol Rhinol Laryngol 100: 348-350.
- Seifert G, Sobin LH (1991) Histological classification of salivary gland tumours. Berlin: Springer Verlag.
- Ellis GL, Auclair PL (1995) Tumors of the salivary glands. Third series ed. Washington : Armed Forces Institute of Pathology.
- Batsakis JG, Luna MA, el Naggar AK (1991) Basaloid monomorphic adenomas. Ann Otol Rhinol Laryngol 100: 687-690.
- Sousa SOM, Araujo NS, Correa L, Soubhia AMP, Araujo VC (2001) Immunohistochemical aspects of basal cell adenoma and canalicular adenoma of salivary glands. Oral Oncol 37: 365-8.
- Barnes L, Eveson JW, Reichart P, Sidransky D (2005) Pathology and genetics of Head and neck tumours. IARC press.
- Choi HR, Batsakis JG, Callender DL, Prieto VG, Luna MA,et al. (2002) Molecular analysis of chromosome 16q regions in dermal analogue tumors of salivary glands : a genetic link to dermal cylindroma ? Am J Surg Pathol 26: 778-783