
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2025) Volume 10, Issue 3
Assessment of Prevalence and Risk Factors for Anastomotic Leakage after Intestinal Resection and Anastomosis at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia: A Cross-Sectional Study
2Department of Public Health, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Received Date: Nov 03, 2025 / Accepted Date: Nov 25, 2025 / Published Date: Dec 03, 2025
Copyright: © 2026 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Lebeza, Y., Terefe, F., Kibret, A., Assefa, G., Gossa, F. (2025). Assessment of Prevalence and Risk Factors for Anastomotic Leakage after Intestinal Resection and Anastomosis at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia: A Cross-Sectional Study. Int J Women
Abstract
Background: An anastomotic leak (AL) is a serious complication of gastrointestinal surgery, characterized by a loss of integrity at the anastomotic site. Despite advancements in gastrointestinal surgery, AL remains a leading cause of postoperative mortality and morbidity worldwide.
Objective: To determine prevalence and identify associated factors of AL following intestinal resection and anastomosis. Methods: A cross-sectional study was conducted on 103 patients who underwent intestinal anastomosis at Yekatit 12 Hospital Medical College from October 2022 to July 2024. Data were collected retrospectively from patient records and analyzed using SPSS version 26. Descriptive statistics, binary logistic regression, and multivariate analysis were performed. A p-value < 0.05 was considered statistically significant.
Results: The prevalence of AL was 13.6%. Gastrointestinal (GI) contamination during the procedure demonstrated a statistically significant association with AL (AOR = 8.88, 95% CI: 1.74–45.31, p = 0.009). The median postoperative hospital stay was 8 days for the entire cohort but 21.5 days for patients with AL. The AL-related mortality rate was 28.6%.
Conclusion: The prevalence of AL in this study was higher than previously reported in other Ethiopian studies. GI contamination was a significant independent risk factor for AL, which was associated with prolonged hospitalization and high mortality. Meticulous surgical technique to minimize contamination is crucial to prevent AL and its severe consequences.
Keywords
Anastomotic Leak, Intestinal Resection, Gastrointestinal Anastomosis, Risk Factors, Ethiopia
Abbreviations
AL: Anastomotic Leak
ASA: American Society of Anesthesiologists
BMI: Body Mass Index
CT: Computed Tomography
DM: Diabetic Mellitus
GI: Gastrointestinal
HGB: Hemoglobin
HIV: Human Immunodeficiency Virus
HTN: Hypertension
IBD: Inflammatory Bowel Disease
MIIH: Menelik II Hospital
LAL: Left side Anastomotic Leak
RAL: Right side Anastomotic Leak
SPSS: Statistical Package for Social Science
TASH: Tikure Anbessa Specialized Hospital
T stage: Tumor Stage
USA: United States of America
Introduction
Anastomotic leak (AL) is a serious complication following gastrointestinal surgery. There remains a lack of a universally agreed-upon definition for AL, though most studies utilize a combination of clinical, laboratory, and radiological findings for diagnosis [1]. The International Study Group of Rectal Cancer (ISREC) defines AL as a defect in the intestinal wall at the anastomosis leading to communication between the intra- and extraluminal compartments, recommending grading based on management strategy [2]. AL can present insidiously with fever and ileus or overtly with peritonitis, abscess formation, sepsis, and multi-organ failure [3]. Established risk factors include advanced age, comorbidities, hypoalbuminemia, malignancy, intraoperative blood loss, and surgical experience [3]. AL significantly increases morbidity, prolongs hospital stays, elevates mortality, and in cancer patients, may adversely affect long-term survival due to an increased risk of local recurrence [4]. The global incidence of AL varies widely, reported between 2.6% and 15.4% [3,5-7]. Previous studies in Ethiopian teaching hospitals reported prevalence rates of 9.9%, 10.8%, and 5.2% [8-10]. Given the variability in AL incidence and associated factors worldwide, and the scarcity of data from our institution, this study aimed to determine the prevalence and identify the risk factors for AL following intestinal resection and anastomosis at Yekatit 12 Hospital Medical College
Materials and Methods
Study Design, Setting, and Period
A retrospective cross-sectional study was conducted at Yekatit 12 Hospital Medical College, reviewing medical records of patients who underwent intestinal anastomosis between October 2022 and July 2024.
Study Population and Sampling
Inclusion and Exclusion Criteria
The study initially identified 106 patients. The final analysis included 103 consecutive adult patients who underwent intestinal resection and anastomosis. Three patients were excluded due to incomplete medical records. Patients who underwent upper gastrointestinal or hepatobiliary anastomoses, as well as pediatric patients, were excluded from the study.
Sample Size Determination, Sampling Technique and Study Variables
The sample size was calculated using a double population proportion formula. Using the type of surgery (emergency vs. elective) as a key determinant for anastomotic leak (AL), and assuming a 95% Confidence Interval (CI), 80% power, a 5% margin of error, the required sample size was determined. The calculation was based on reference proportions of AL of 12.5% for emergency and 3.5% for elective surgeries from a previous study [10]. This yielded a minimum sample size of 139 patients.
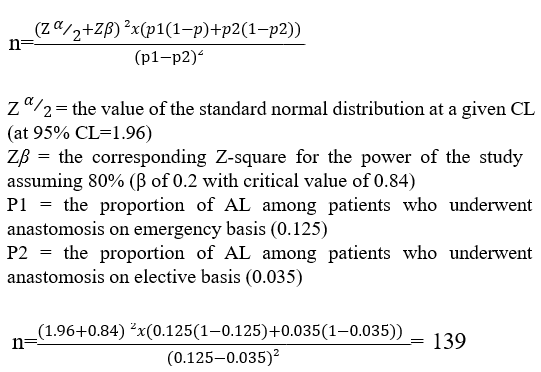
However, a consecutive sampling method was employed, and all 103 eligible patients who underwent the procedure within the study period were included in the final analysis.
The study assessed the association between clinical anastomotic leak (the outcome variable) and various independent variables, including socio-demographic factors (age, sex), patient characteristics (preoperative hemoglobin, need for intraoperative blood transfusion), urgency of surgery, disease condition, comorbidities, anastomosis technique and location, the operating physician's status, and the presence of intraoperative contamination (Figure).

Figure: Illustrates the Conceptual Framework Showing the Association Between Clinical Anastomotic Leak (the Dependent Variable) and the Various Independent Variables
Operational Definitions
• Anastomotic Leak: A full-thickness defect in the intestinal wall at the anastomotic site, leading to communication between the intraluminal and extraluminal compartments. Diagnosis was confirmed by a physician based on clinical signs (e.g., peritonitis, septic shock) and/or radiological evidence, and the condition necessitated surgical re-intervention [11].
Data Collection Tool and Procedure
Data were extracted from electronic medical records, morning reports, and operative registries using a pre-tested, structured data extraction checklist. The collected variables included demographic characteristics, indications for surgery, location and type of anastomosis, procedure duration, degree of intraoperative gastrointestinal contamination, and postoperative outcomes.
Data Quality Management
To ensure data quality, the data extraction tool was carefully designed and pre-tested. Data collectors (surgical residents) and supervisors were trained on the study protocol and data collection procedures. Throughout the data collection period, the supervisor continuously reviewed the collected data for accuracy and completeness.
Data Processing and Analysis
The collected data were cleaned, coded, and entered into SPSS version 26 for analysis. Descriptive statistics (e.g., frequencies, percentages) were used to summarize the data. To identify factors associated with anastomotic leak, binary logistic regression was employed, beginning with bivariate analysis and proceeding to multivariate analysis. Results are presented in text and tables. An Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) was computed, and a p-value < 0.05 was considered statistically significant.
Ethical Considerations
Ethical approval was obtained from the Ethical Review Committee of Yekatit 12 Hospital Medical College, and operational permission was secured from the Department of General Surgery. The requirement for individual informed consent was waived by the ethics committee due to the retrospective nature of the study and the use of anonymized secondary data. All personal identifiers were removed during data collection to ensure confidentiality. The anonymized data were stored securely and used exclusively for the purposes of this research.
Results
Sociodemographic and Baseline Characteristics
A total of 103 patients were analyzed. The majority were male (58.3%, n = 60), and the median age fell within the 31-60 years category (51.5%, n = 53). Most surgeries were elective (62.1%, n = 64), and benign conditions were the primary indication for surgery (82.5%, n = 85) (Table 1).
|
Variable |
Response |
Frequency |
Percent |
|
Sex |
Male |
60 |
58.3% |
|
Female |
43 |
41.7% |
|
|
Age in years |
15 to 30 |
29 |
28.2% |
|
31 to 60 |
53 |
51.5% |
|
|
Above 60 |
21 |
20.4% |
|
Type of admission |
Elective |
64 |
62.1% |
|
Emergency |
39 |
37.9% |
|
|
Disease Condition |
Benign |
85 |
82.5% |
|
Malignant |
18 |
17.5% |
Table 1: Demographic and Baseline Characteristics of 103 Patients Who Underwent Intestinal Anastomosis in Yekatit 12 Hospital Medical College, October 2022 to July 2024
Disease and Treatment-Related Factors
The most common indications for surgery were redundant sigmoid colon (24.3%) and stoma reversal (21.5%). Most procedures (70.9%) lasted between 2-4 hours. Colorectal (34.9%) and ileo- ileal (35.0%) were the most frequent anastomotic types. GI contamination was present in 25.2% (n = 26) of cases (Table 2). Most operations were performed by surgical residents (R3: 36.9%, R4: 46.6%).
|
Variable |
Response |
Frequency |
Percent |
|
Diagnosis |
Redundant Sigmoid |
24 |
27% |
|
Colonic cancer |
9 |
10.1% |
|
|
Colostomy |
9 |
10.1% |
|
|
Ileostomy |
11 |
12.4% |
|
|
Complicated IBD |
4 |
4.5% |
|
|
Gangrenous SBO |
5 |
5.6% |
|
|
Small bowel perforation |
4 |
4.5% |
|
|
Small bowel mass |
9 |
10.1% |
|
|
Post traumatic bowel perforation |
1 |
1.1% |
|
|
Sigmoid Volvulus |
5 |
5.6% |
|
|
Colon perforation |
3 |
3.4% |
|
|
SBO 20 to complicated hernia |
5 |
5.6% |
|
|
Duration of surgery |
Less than 2 hours |
24 |
23.3% |
|
2 to 4 hours |
73 |
70.9% |
|
|
Above 4 hours |
6 |
5.8% |
|
|
GI contamination |
Yes |
26 |
25.2% |
|
No |
77 |
74.8% |
|
|
Location of anastomosis |
Ileoileal |
36 |
35% |
|
Ileo- ascending |
2 |
1.9% |
|
|
Ileo-transverse |
18 |
17.5% |
|
|
Colo-colic |
9 |
8.7% |
|
|
Colorectal |
37 |
35.9% |
Table 2: Shows Disease and Treatment Related Factors of the Study to Assess the Prevalence and Risk Factors Associated with Anastomotic Leak after Intestinal Resection and Anastomosis
Prevalence and Outcomes of Anastomotic Leak
The overall prevalence of AL was 13.6% (14/103). Leaks were most commonly diagnosed on postoperative day 7 (median: 7 days). The majority (57.1%) were diagnosed using both clinical and radiological findings. Most leaks (78.6%) were managed with re-laparotomy and stoma formation (Table 3).
|
Variable |
Response |
Frequency |
Percent |
|
Presence of leak |
Yes |
14 |
13.6% |
|
No |
86 |
86.4% |
|
|
Postop complication |
Yes |
33 |
32% |
|
|
No |
77 |
68% |
|
Diagnosis of AL |
Clinically |
5 |
35.7% |
|
Imaging |
1 |
7.1% |
|
|
Both clinically and imaging |
8 |
57.1% |
|
|
Leak detected date |
5th day |
1 |
7.1% |
|
6th day |
4 |
28.6% |
|
|
7th day |
4 |
28.6% |
|
|
8th day |
4 |
28.6% |
|
|
9th day |
1 |
7.1% |
|
|
Management of AL |
Re-laparotomy with re- anastomosis |
3 |
21.4% |
|
Re-laparotomy with Stoma |
11 |
78.6% |
|
|
Duration of hospital stay |
Less than 1 week |
36 |
35% |
|
1 to 2 weeks |
42 |
40.8% |
|
|
Above 2 weeks |
25 |
24.3% |
|
|
Outcome of the patient |
Discharged improved |
96 |
93.2% |
|
Died in Hospital |
7 |
6.8% |
Table 3: Anastomotic leak Rate, Leak Diagnosis and Management, Duration of hospital Stay, and Outcome of 103 Patients who Underwent Intestinal Resection and Anastomosis in Yekatit 12 Hospital Medical College, from October 2022 to July 2024
Patients with AL had a significantly longer mean hospital stay (33.5 ± 22.3 days) compared to those without AL (10.1 ± 7.8 days), p<0.001. The inpatient mortality rate was significantly higher in the AL group (28.6% vs. 3.4%, p<0.001) (Table 4).
|
Variable |
|
No anastomosis leak |
Anastomosis leaked |
P-value |
||
|
|
|
N |
Percent |
N |
Percent |
|
|
Hospital stays |
Mean ± SD in days |
10.09 ± 7.80 |
33.50 ± 22.31 |
0.001 |
||
|
Less than 1 week |
35 |
39.3% |
1 |
7.1% |
||
|
1 to 2weeks |
41 |
46% |
1 |
7.1% |
||
|
2 to 3weeks |
10 |
11.3% |
5 |
35.7% |
||
|
3 to 4 weeks |
0 |
0 |
1 |
7.1% |
||
|
Above 4 weeks |
3 |
3.4% |
6 |
42.8% |
||
|
Total |
89 |
100% |
14 |
100% |
||
|
Outcome of the patient |
Discharged improved |
86 |
96.6% |
10 |
71.4% |
0.001 |
|
Died in the Hospital |
3 |
3.4% |
4 |
28.6% |
||
Table 4: The Effect of AL on Postoperative Outcomes on Patients who Underwent Intestinal Anastomosis in Yekatit 12 Hospital Medical College, October 2022 to July 2024
Risk Factors for Anastomotic Leak
In bivariate analysis, factors such as age, ASA grade, type of admission (emergency), and GI contamination showed an association with AL (p < 0.25). On multivariate logistic regression, only GI contamination remained an independent significant risk factor. Patients with GI contamination had 8.88 times higher odds of developing AL (AOR = 8.88, 95% CI: 1.74–45.31, (p = 0.009) (Table 5).
|
Variable |
Response |
Anastomosis leak |
No anastomosis leak |
Pvalue |
|
|
|
N(Percent) |
N(Percent) |
|
|
Sex |
Male |
8(13.3%) |
52(76.7%) |
0.955 |
|
|
Female |
6(13.9%) |
37(84.1%) |
|
ASA grading |
I |
3(6.5%) |
43(93.5%) |
|
|
II |
9(18.3%) |
40(81.7%) |
||
|
III |
2(25%) |
6(75%) |
||
|
GI contamination |
Yes |
10(38.5%) |
16(61.5%) |
<0.001 |
|
No |
4(5.3%) |
72(94.7%) |
||
|
Type of admission |
Elective |
4(6.3%) |
60(93.7%) |
0.001 |
|
Emergency |
10(25.6%) |
29(74.4%) |
Table 5: Shows Association of Possible Risk Factors with AL in Patient who Underwent Intestinal Anastomosis in Yekatit 12 Hospital Medical College in the study Period
Discussion
Understanding the prevalence and risk factors for anastomotic leak (AL) is critical for improving surgical outcomes. In our study, the AL prevalence was 13.6%. This rate is higher than those reported in similar Ethiopian studies from Addis Ababa teaching hospitals, which ranged from 5.2% to 10.8%, [8-10]. The median time to AL detection in our study was 7 days (IQR: 5-9), which is earlier than the 10 days (range: 3-14) reported by one of these comparable studies [10,12]. We found no significant association between patient sex and the rate of AL, a finding consistent with some Ethiopian studies [9,10]. though the literature remains conflicting, with other studies reporting higher rates in either males or females [6,8,13]. Several established risk factors for AL were observed in our population. Patients undergoing emergency procedures developed AL more frequently than those having elective surgery (25.6% vs. 6.3%), although this difference was not statistically significant (p=0.496). This trend aligns with numerous other studies [5,8,9,14,15]. Emergency surgery inherently carries a higher risk of gastrointestinal contamination, peritoneal infection, and physiological derangement, often requiring resuscitation with vasopressors or blood products all of which are confounding factors that can compromise anastomotic healing. Furthermore, we observed a non-significant trend (p = 0.053) towards higher AL rates in patients with ASA scores of II and III compared to ASA I (18.4% & 25% vs. 6.5%), consistent with previous reports [9,14,15]. A higher ASA score, often reflecting advanced age and comorbidities, is a well-documented risk factor for poor postoperative outcomes.
A statistically significant predictor of AL in our study was the presence of gastrointestinal contamination at surgery (AOR 8.877; 95% CI 1.739-45.306). This finding is strongly supported by the literature [16-18]. The pathophysiological mechanism is likely multifactorial: bacterial overgrowth and local infection can weaken the anastomotic tissue, disrupt normal immune responses and tissue regeneration, compromise suture integrity, and impair local blood flow, thereby creating a vulnerable environment for leak. The clinical impact of AL was profound. The mean hospital stay was significantly longer for patients with AL compared to those without (33.50 ± 22.31 days vs. 10.09 ± 7.80 days; p = 0.001), a finding consistent with other studies [8,10,19]. This extended hospitalization is attributable to increased healing time and a higher susceptibility to postoperative complications, such as surgical site infections, which may necessitate repeated returns to the operating room and prolonged exposure to medical interventions. Finally, AL was associated with a substantially higher inpatient mortality rate of 28.6%, compared to 3.4% in patients without AL. This mortality rate is lower than the rates of 48-65.3% reported in three earlier Ethiopian studies a difference that may be partly explained by our earlier median time to AL detection, allowing for more prompt intervention [8-10]. Conversely, our mortality rate is higher than the 2.6-10.9% reported in some international studies a disparity that may be influenced by differences in sample size, patient populations, and available institutional resources [6,14,20,21].
Limitations
This study has limitations. Its single-center, retrospective design and relatively small sample size limit the generalizability of the findings and the power to detect other potential risk factors. The findings should be interpreted with this context in mind.
Conclusion and Recommendations
The rate of anastomotic leak in this study was high. GI contamination during surgery was identified as a significant independent risk factor. AL was associated with dramatically prolonged hospital stays and increased mortality. We recommend that surgeons and trainees exercise utmost care to minimize GI contamination during intestinal anastomosis. Adherence to principles of septic surgery, judicious use of drains, and considering staged procedures in contaminated emergency cases may help reduce the rate of AL and its devastating consequences. Further large-scale, multi-center prospective studies are recommended to identify other modifiable risk factors.
Data Availability Statement
All data supporting the case report is available with the correspondence.
Acknowledgements
The authors would like to express their sincere gratitude to Yekatit 12 Hospital Medical College, Department of Surgery, for providing the opportunity to conduct this study. We are deeply thankful to all the individuals involved in data collection and case management. Our heartfelt appreciation goes to the data collectors and our friends for their diligent work and valuable comments. This research would not have been possible without the participation of all involved individuals. Lastly, we extend our thanks to the emergency nurses, interns, liaison staff, operating room staff, surgeons, residents, anesthesia teams, and supporting staff for their dedicated management of the patients.
References
- Bruce, J., Krukowski, Z. H., Alâ?Khairy, G., Russell, E. M., & Park, K. G. M. (2001). Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. British Journal of Surgery, 88(9), 1157-1168.
- Cong, Z. J., Hu, L. H., Bian, Z. Q., Ye, G. Y., Yu, M. H.,Gao, Y. H., ... & Zhong, M. (2013). Systematic review of anastomotic leakage rate according to an international grading system following anterior resection for rectal cancer. PLoS One, 8(9), e75519.
- Sakr A, Emile SH, Abdallah E, Thabet W, KhafagyW. Predictive Factors for Small Intestinal and Colonic Anastomotic Leak: A Multivariate Analysis. Indian J Surg. 2016 Oct;79(5):555-62.
- Zarnescu, E. C., Zarnescu, N. O., & Costea, R. (2021). Updates of risk factors for anastomotic leakage after colorectal surgery. Diagnostics, 11(12), 2382.
- Nikolian, V. C., Kamdar, N. S., Regenbogen, S. E., Morris, A. M., Byrn, J. C., Suwanabol, P. A., ... & Hendren, S. (2017). Anastomotic leak after colorectal resection: a population-based study of risk factors and hospital variation. Surgery, 161(6), 1619-1627.
- Degiuli, M., Elmore, U., De Luca, R., De Nardi, P., Tomatis, M., Biondi, A., ... & D’Ugo, D. (2022). Risk factors for anastomotic leakage after anterior resection for rectal cancer (RALAR study): A nationwide retrospective study of the Italian Society of Surgical Oncology Colorectal Cancer Network Collaborative Group. Colorectal Disease, 24(3), 264-276.
- El-Badawy, H. A. A. E. (2014). Anastomotic leakage after gastrointestinal surgery: risk factors, presentation and outcome. The Egyptian Journal of Hospital Medicine, 57(1), 494-512.
- Mekete A, Kotisso B, Ersumo T. A Retrospective Descriptive Study of Gastrointestinal Leak and Risk Factors in Four University Hospitals in Addis Ababa, Ethiopia. Ethiop Med J. 2022 Jan;60(1):49-56.
- Zemenfes, D., & Tamirat, E. (2019). Prevalence of and factors associated with anastomotic leakage among surgical patients at 2 teaching hospitals in Addis Ababa, Ethiopia. East and Central African Journal of Surgery, 24(2), 89-93IJWHC-25-29.docx.
- Wako, G., Teshome, H., & Abebe, E. (2019). Colorectal anastomosis leak: rate, risk factors and outcome in a Tertiary Teaching Hospital, Addis Ababa Ethiopia, a five year retrospective study. Ethiopian journal of health sciences, 29(6).
- Rahbari, N. N., Weitz, J., Hohenberger, W., Heald, R. J., Moran, B., Ulrich, A., ... & Büchler, M. W. (2010). Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery, 147(3), 339-351.
- Gessler, B., Eriksson, O., & Angenete, E. (2017). Diagnosis, treatment, and consequences of anastomotic leakage in colorectal surgery. International Journal of colorectal disease, 32(4), 549-556.
- Lipska, M. A., Bissett, I. P., Parry, B. R., & Merrie, A. E. (2006). Anastomotic leakage after lower gastrointestinal anastomosis: men are at a higher risk. ANZ journal of surgery, 76(7), 579-585.
- Bakker, I. S., Grossmann, I., Henneman, D., Havenga, K., & Wiggers, T. (2014). Risk factors for anastomotic leakage and leak-related mortality after colonic cancer surgery in a nationwide audit. Journal of British Surgery, 101(4), 424-432.
- Isik, O., Yilmazlar, T., Ozturk, E., & Sarkut, P. (2015). Anastomotic leak after colorectal surgery: leak rate for right hemicolectomy may be higher than expected. Journal Integrative Oncology, 2329-6771.
- Dyegura, O. J., & MAGOHE, N. (2024). Prevalence and factors associated with anastomotic leakage among patients undergoing bowel resection and anastomosis. Int J Health Med Nurs Pract, 6(1), 1-14.
- Van Rooijen, S. J., Huisman, D., Stuijvenberg, M., Stens, J., Roumen, R. M. H., Daams, F., & Slooter, G. D. (2016). Intraoperative modifiable risk factors of colorectal anastomotic leakage: why surgeons and anesthesiologists should act together. International Journal of Surgery, 36, 183-200.
- Leichtle, S. W., Mouawad, N. J., Welch, K. B., Lampman,R. M., & Cleary, R. K. (2012). Risk factors for anastomotic leakage after colectomy. Diseases of the Colon & Rectum, 55(5), 569-575.
- Numaro, Y. T., Kebede, M. A., Mariam, S. N. G., Abebe, N.S., Gossaye, B. T., Shenga, S. D., ... & Kassa, H. B. (2025). Clinical anastomosis leakage and determinant factors among patients who underwent intestinal anastomosis in two Ethiopian tertiary hospitals. BMC gastroenterology, 25(1), 610.
- Veyrie, N., Ata, T., Muscari, F., Couchard, A. C., Msika, S., Hay, J. M., ... & French Associations for Surgical Research. (2007). Anastomotic leakage after elective right versus left colectomy for cancer: prevalence and independent risk factors. Journal of the American College of Surgeons, 205(6), 785-793.
- McArdle, C. S., McMillan, D. C., & Hole, D. (2005). Impact of anastomotic leakage on long-term survival of patients undergoing curative resection for colorectal cancer. Journal of British Surgery, 92(9), 1150-1154