
International Journal of Clinical & Experimental Dermatology(IJCED)
ISSN: 2476-2415 | DOI: 10.33140/IJCED
Impact Factor: 1.9

Case Report - (2026) Volume 11, Issue 2
Artificial Intelligence (AI) in Modern Dermatopathology Practice
2University of Wolverhampton, North Cumbria Integrated Care NHS Foundation Trust, United States
3The Midlands Medical Academy, United Kingdom
4University of Wolverhampton, School of Health & Wellbeing, United Kingdom
Received Date: Apr 08, 2026 / Accepted Date: May 13, 2026 / Published Date: May 27, 2026
Copyright: ©2026 Mohammed S Al Abadie, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Abed, N., Mahfoudh, M., Al Abadie, S., Kubba, F., Al Abadie, M. S. (2026). Artificial Intelligence (AI) in Modern Dermatopathology Practice. Int J Clin Expl Dermatol, 11(2), 01-10.
Abstract
The integration of Artificial Intelligence is fundamentally reshaping the field of dermatopathology, which traditionally suffers from high interobserver variability and reliance on subjective interpretations of histopathological features, especially in complex melanocytic lesions and the diagnostic "gray zone". Leveraging computer vision techniques, primarily through CNNs, and relying on high-resolution WSI derived from digital pathology workflows, AI models are achieving performance comparable to or exceeding human experts in many classification tasks. Furthermore, AI provides advanced capabilities such as predictive analytics and prognostic assessments through the integration of multimodal data. AI also drastically optimizes clinical workflows and reduces turnaround times by automating repetitive tasks, including mitotic figure counting, classifying diseases, and aiding in diagnosis decision-making. Despite these achievements, significant barriers to widespread clinical integration remain, notably the scarcity of adequately diverse and annotated training datasets, which can result in algorithmic bias in diverse populations.
Keywords
Artificial Intelligence, AI, Dermatopathology, Dermatology
Artificial Intelligence and Modern Dermatopathology: A Literature Review
Dermatopathology is the microscopic study of skin diseases and a subspecialty of histopathology, serves as the fundamental basis of dermatological diagnostics, providing pathogenesis, prognosis, and management for complex conditions.
The integration of artificial intelligence (AI) holds transformative potential for medical diagnostics and in dermatopathology classifications. AI systems can analyze and quantify skin lesion features far beyond human capability, leading to potential improvements in accuracy and efficiency. These technologies offer innovative solutions that can enhance the accuracy and efficiency of dermatological assessments and help democratize access to high-quality diagnostic tools [1].
The objective of this literature review is to analyze scientific literature based on the application of AI in dermatopathology and the techniques employing intelligent systems for both dermatological diagnostics and dermatopathology. Specifically, this work explores the transformative potential of AI and ML in dermatopathology, with a focus on their applications in diagnostic precision, predictive analytics, and classification of skin diseases. Ultimately, the goal of this review is to provide a comprehensive overview of the latest research, highlighting opportunities and challenges in the field, and offering a resource for researchers and practitioners to encourage interdisciplinary collaboration between AI systems and health professionals.
History of AI
“Could a man-made device act and make decisions indistinguishable from those of humans?” - Alan Turing's profound yet simple question marked the beginning of the use of AI in research and future works in various fields, including medicine [2]. The use of AI in the medical field took off in the 1970s, with the primary goal of its application being to create systems that mimic human intelligence by assisting specialists in developing diagnoses and treatment plans [3]. INTERNIST-1, the first artificial medical consultant that utilized patients’ symptoms to deliver a clinical diagnosis, was designed to assist physicians in eliminating differential diagnoses and supporting their judgment. At this juncture, the rise of AI implications showed promising potential in medicine, and continuing trends of its use began to develop, such as MYCIN, where it is used to support physicians during their practice to prescribe the correct antibiotics to their patients [4].
With the evolution of computer science in the 2000s, advancements in natural language processing and machine learning have rapidly increased in evaluating vast amounts of data as well as forming complex AI systems. In 2007, IBM created a question-and-answer system called Watson that demonstrated the growth of AI use in healthcare settings from symptom input to medical diagnosis [5]. In 2017, the Watson system was able to predict amyotrophic lateral sclerosis by identifying RNA-binding proteins [6].
AI Explained: How Does AI Work?
AI foundations are based on two types of learning those are machine learning (ML) and deep learning (DL). ML is an AI technique that uses statistical data and its algorithm to learn and predict the next common traits to apply the task successfully. ML utilizes logistic regression, linear regression, and random forest (RF) as its statistical learning methods, while employing K-nearest neighbor as its data classifier and regressor [7]. When ML provides the foundational principles and algorithm to the system through data, artificial neural networks (ANNs) begin to form to apply these principles. ANNs are often called neural networks that are inspired by the formation of interconnecting neurons and are organized in layers. Their role is mainly strengthening the “weight” between neurons as they process data when giving feedback. When ANNs form multiple layers, they begin to form a subset of ML, which is called Deep Learning (DL). DL is a branch of ML; it functions to recognize and learn specific features by processing data from deep neural networks with multiple layers. The computational model used in DL is an artificial neural network (ANN) that is also based on biological neural networks. This layered structure allows DL to form complex, hierarchical patterns from raw data and patterns that can process speech and medical images through a formed neural network, such as Convolutional Neural Networks (CNNs), a specialized type of deep neural network of DL. Use of ML and DL can serve each other in providing the best and accurate response to any task when fed the right information. ML is not subjective and does not depend on external factors when delivering the task. The following Figure 1 shows the conceptual hierarchy of AI.

Figure 1: Conceptual Hierarchy of AI
The following figure presents conceptual hierarchy of AI, where the “crown” of the tree represents the umbrella of AI, encompassing the broadest discipline. Within this evolving concept, machine learning resembles the “branch” as it evolved into a foundational subfield of AI, driving its initial growth and branching into various methodologies. Subsequently, Artificial Neural Networks (ANNs) resemble the “trunk”, as an organization of interconnected neurons into multiple layers to form the strength of the synaptic weight, and parallelly deepen the tree “roots”, which in AI is considered deep learning. The further data “water” we add to the tree, the more complex the system becomes, and the more new neural networks, such as CNNs, RNNs, and other neural architectures, are formed.
Applications of AI in Dermatopathology
With the innovative solutions that today’s technology has provided, from diagnosis to treatment planning, AI is on the rise in its application with skin cancer screening, and it is expanding into inflammatory and non-melanoma skin cancer cases. The following section will explore diverse applications of AI in dermatopathology.
|
Application Area |
AI Technique(s) |
Focus / Function |
Key Findings |
Reference(s) |
|
Diagnosis of Melanocytic Lesions |
CNNs, SVM, Decision Trees |
Classification of melanoma vs benign lesions |
CNN achieved 96.82% sensitivity and 93.44% specificity; outperformed other models |
[8-10] |
|
Naevoid Melanoma |
Fast Random Forest (FRF) |
Pre-screening tool for NM histopathological images |
12–17% discordance vs dermatopathologists; useful for early screening |
[11,12] |
|
Spitz Nevi Classification |
CNN |
Differentiation between Spitz and conventional nevi |
Accuracy 92% (selected WSIs), 52% (non-selected WSIs) |
[13] |
|
Acral and Mucosal Melanoma |
CNN |
Classification of melanoma subtypes |
AUC: Acral (0.928), Mucosal (0.754), Nail (0.621) |
[14,15] |
|
Inflammatory Dermatoses |
Deep Learning (Cascaded DL) |
Subtyping and classification of dermatitis and psoriasis |
Accuracy up to 99%; high diagnostic precision |
[16-19] |
|
Non-Melanoma Skin Cancer (NMSC) |
Deep Learning CNN |
Classification of BCC, SCC, AK, SK |
Accuracy 98–100%; high sensitivity (91.7%) and specificity (89.8%) |
[20-22] |
|
Predictive Analytics |
CNN, Machine Learning Models |
Predicting recurrence, treatment response, and surgery complexity |
AUC 0.91 for melanoma recurrence; 0.778 for ICI response; effective predictive performance |
[23-26] |
Table 1: Overview of AI Applications in Dermatopathology
Diagnosis of Melanocytic Lesions
The success of AI in early diagnosing and differentiating lesions has grown in the field of dermatological studies, specifically in rare conditions such as melanoma [27]. One multidimensional study was conducted to clinically diagnose melanoma by using two different modalities. The first module is CNNs, where dermatoscopic images with early-stage melanoma are taken from patients, and the second module is based on Support Vector Machines and Decision Trees, is used to analyze data from histopathology, clinical, and biomarkers (Figure 2A, 2B, 2C). The CNNs module proved a higher score with a specificity of 93.44% and a sensitivity of 96.82% compared to the second prognostic module, with disease-free survival of 87%, and metastasis prediction of 88.24%. With such studies conducted, the AI systems can be supplemented in the future for early screening and treatment planning [8].
The performance of the AI systems has achieved diagnostic accuracy similar to or better than certified dermatologists. A study was conducted to compare the CNN system to a group of 21 certified dermatologists to distinguish between melanoma from benign nevi [9]. Another study compared 18 dermatopathologists to a 3 CNN module, with a mean accuracy of 90% per dermatopathologist and 92% for the CNN system used. However, the panel of experts recorded an overall score of 98% and the discordance was at 1345% between the CNNs and dermatopathologists [10].
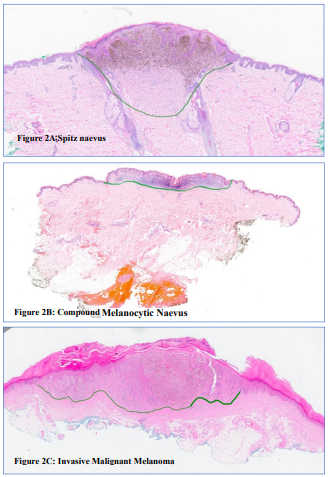
Figure 2: Shows three types of melanocytic lesions from whole slide images (WSI). The green line at the deep lesion margin varies according to the type of lesion. This WSI example is used for training deep learning models. (Courtesy of Dr F. Kubba)
Naevoid Melanoma (NM): Naevoid melanoma is a rare type of malignant melanoma that was first reported in 1980 by Levene and was called “verrucous and pseudonaevoid melanoma” [28]. In 1985, Schmoeckel reported 33 patients with similar features of benign melanocytic lesions, as well as conducting a five-year follow-up, and described the disease as “naevoid malignant melanoma” [29]. One study applied fast random forest (FRF) machine learning in 18 cases as a pre-screening tool for NM histopathological images in comparison to dermatopathologists. Results have shown a 12% lower threshold in providing efficacy in targeting dangerous cases [11]. One study has used 63 patient datasets using the FRF module and has shown results of 17%discordance with the dermatopathologist's diagnosis [12].
Spitz Nevi: Another challenge in differentiating melanoma is Spitz Nevi variant, known as “SPARK”, where it is identified as “Spitz’s” and “Clark’s” features. A recent study trained CNN to classify melanocytic malignancies into conventional melanocytic nevi and Spitz nevi. The training results based on the representative images selected by dermatopathologists have shown an accuracy of 92% [13]. However, when trained on non-selected whole-slide images (WSIs) by dermatopathologists, accuracy dropped to 52%. This concludes the importance of the data selection role in training AI models.
Acral and Mucosal Melanoma: Further types of melanoma where AI training has also been applied is in Acral and Mucosal Melanoma. A study conducted by Winkler was focused on distinguishing common benign lesions that have been matched for localization. CNN performed well in differentiating acral, mucosal, and nail melanoma, using the area under the receiver operating curves (AUCs) scale to measure the overall diagnostic or classifier test. AUC of 1.0 is an ideal and a perfect classifier, and a performance of 0.5 is no better than a random chance. Acral melanoma (AUC 0.928) was markedly higher than mucosal (0.754) and nail unit (0.621) melanomas [14]. Another study found a CNN's diagnostic accuracy in comparison with a group of dermatologists for acral melanoma was similar.
Whereas AUC results for both the CNN models and the group of experts were above 0.8 [15].
Classification of Inflammatory Dermatoses
An emerging field that is less explored in the application of AI is inflammatory skin diseases. The complex nature and wide spectrum of diseases create a major challenge for pathologists when developing reliable AI models for diagnostic applications.
Superficial Perivascular Dermatitis: One of the most common types of dermatoses, with several subtypes such as interface, psoriasiform, and spongiotic. One study developed a cascaded deep learning model to subtype classifications from pathological images. Overall, from the 3,954 pathological images, the AI model identified 13 key pathological features with an accuracy of 85.24% [16]. The performance results are noted to be similar to dermatopathologists diagnosis accuracy.
Psoriasis: A chronic immune-mediated inflammatory disease that affects 2% of the world population. Several studies have applied AI to improve the classification of psoriasis from images. One example demonstrated the application of AI to classify the psoriasis lesions' severity with average sensitivities between 93.81% and 99.76% [17]. Another study achieved the use of a U-shaped CNN to identify the types of 90 psoriasis biopsy images compared to other AI methods [18]. In addition, a group of researchers developed a future clinical implication in precision medicine by establishing an AI pipeline of immunohistochemical signals from 8 psoriatic and 6 atopic eczema patients [19].
Other Inflammatory Conditions: Chronic dermatitis, lichen planus, and acne are other inflammatory conditions that have been classified using AI applications. A study developed a classifier tool to distinguish between papulosquamous diseases to analyze 34 variants such as erythema and scaling [24]. Another study applied AI to differentiate between dermatomyositis and other types of myositis through muscle ultrasound, and the accuracy results were 76.2% and 86.6% [25].
Detection of Non-Melanoma Skin Cancers
Applied AI is on the rise in classifying non-melanoma skin cancers (NMSCs), such as squamous cell carcinoma (SCC) and basal cell carcinoma (BCC), versus benign and pre-malignant lesions.
Basal Cell Carcinoma (BCC): A Series of studies has been conducted to classify BCC lesions. One study conducted the use of an AI system to analyze and classify- BCC histopathological images with an accuracy of 98.1% [30]. In another study, a deep learning AI tool was applied to achieve 100% sensitivity and 98.9% accuracy for nodular BCC [31].
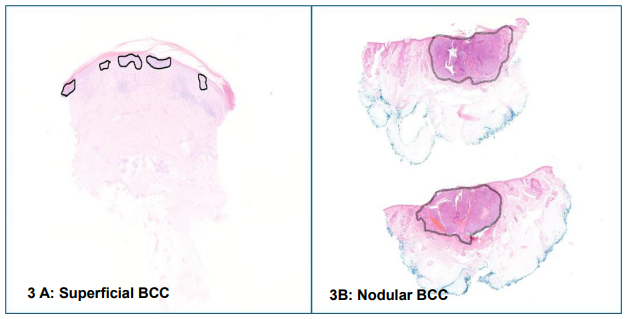
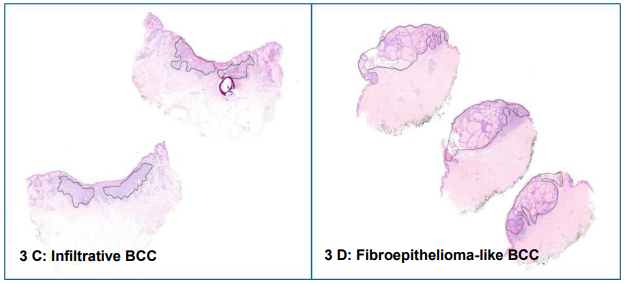
Figure 3: Shows examples of four subtypes of BCC with multiple H and E stained sections annotated for training phase, ×1 magnification. (Courtesy of Dr F. Kubba)
General NMSC and Actinic Keratosis (AK): A deep learning model was used to diagnose three common variants, which are nodular dermal nevi, BCC, and seborrheic keratosis (SK). The results have shown for all three a high diagnostic performance, with the SK achieving 100% accuracy on 123 cases. This demonstrates AI's proficiency in recognizing common benign and malignant lesions [Diagnostic Performance of Deep Learning Algorithms Applied.pdf]. While an AI model was able to distinguish normal skin images from actinic keratosis with a specificity of 89.8% and a sensitivity of 91.7% [22].
|
Condition / Disease |
AI Model |
Metric(s) |
Performance |
Compared To |
Reference |
|
Melanoma vs Benign Nevi |
CNN |
Sensitivity / Specificity |
96.82% / 93.44% |
Dermatologists |
[8,9] |
|
Nevoid Melanoma |
Fast Random Forest |
Concordance Rate |
83–88% |
Dermatopathologists |
[11,12] |
|
Spitz Nevi |
CNN |
Accuracy |
92% (selected WSIs) |
Human Experts |
[13] |
|
Acral Melanoma |
CNN |
AUC |
0.928 |
Dermatologists |
[14,15] |
|
Superficial Perivascular Dermatitis |
Cascaded DL |
Accuracy |
85.24% |
Expert Pathologists |
[16] |
|
Psoriasis |
U-shaped CNN |
Sensitivity |
93.81–99.76% |
Clinical Gold Standard |
[17,18] |
|
Basal Cell Carcinoma |
CNN / DL Models |
Accuracy |
98–100% |
Dermatopathologists |
[20,21] |
|
Actinic Keratosis |
AI Classifier |
Specificity / Sensitivity |
89.8% / 91.7% |
Clinical Diagnosis |
[22] |
|
Melanoma Recurrence |
CNN (WSI-based) |
AUC |
0.91 |
Survival Correlation |
[23] |
Table 2: Summary of Diagnostic Accuracy Metrics in Key AI Studies
Predicting Prognosis and Treatment Response
Beyond diagnosis, predicting disease outcomes and developing treatment algorithms are the cornerstones of applying AI in dermatological practices. In this section, various studies have been applied in different clinical situations.
Predicting Melanoma Recurrence and Treatment Response
One study trained a CNN on WSIs of primary melanoma tumours to predict distant metastatic recurrence (DMR). The model resulted in accuracy of 0.91 AUC and 0.88 AUCs in two sets, where its output correlated with disease-specific survival [23]. In terms of treatment response using the immune checkpoint inhibitors (ICI). A CNN analysing histology alone was able to predict ICI response with an AUC of 0.778 [24].
Predicting Psoriasis Treatment Response: An AI system was developed to predict psoriasis patients' responses to biologic therapy by using initial visit parameters such as weight and age of psoriasis onset. This preliminary model could theoretically be used to optimise therapy for individual patients [25].
Predicting Mohs Surgery Complexity: An application was created to predict the complexity of Mohs surgery based on variables such as tumour size and patient age, which could be used to triage patients and prioritize referrals [26].
AI Challenges in Dermatopathology
Beyond the implementation potential of AI in clinical practice, challenges are still affecting its functionality, whether in its application, required datasets, or ethical concerns. The common hurdles in implementing AI in clinical practice range from technological constraints to human acceptance and standardization issues.
AI continues to face significant challenges when being adopted by medical institutions. Practical challenges such as image quality, computational constraints, and data privacy are common issues that face health professionals. The requirements for deep learning models are substantial computational power and storage, which are currently limited in routine clinical environments. Implementing digital pathology (DP) and AI systems often needs high initial costs, which serve as a major obstacle for many medical centers [32].
Standardization is one of the fundamental bases of AI systems. However, various aspects of dermatological image acquisition are non-standardized, such as the room lighting, angle of the image, background, and patient positioning can affect AI decision-making results.
Regulatory hurdles from documentation and validation from authorities can further delay implementation and could lag behind the technological advancements that can benefit future practices.
Need for Large, High-Quality, and Annotated Datasets
A primary limitation of AI systems is the requirement for datasets of appropriate quality to power the algorithms and deliver accurate results.
Data volume and quality are critical as they can yield the formation of the CNNs' accurate results when implemented and trained. Insufficient or low-quality training datasets directly impact the practicability and the accuracy of AI algorithms, as they can fail to meet the demands of daily clinical applications.
Another factor that can restrict the full potential of AI applications is the lack of diversity and bias, as the performance of AI models heavily depends on the diversity of training datasets. For example, the prominent existing image datasets (such as HAM10000 and ISIC) are composed predominantly from light-skinned individuals, resulting in biased algorithms that perform suboptimally for patients with Skin of Color (SOC) [33]. This lack of diversity can exacerbate clinical practice in diverse populations.
Data labeling and annotation are critical for dataset quality. If experienced pathologists incorrectly label images, it reduces the model's performance and results in training errors. In addition to image labeling, the high pixel density and massive size of WSIs, often require 5GB or more per image, which further poses significant technical hurdles for processing [34].
Medical institutes and research teams rely on private datasets from either their own private practice or affiliated institutions, which poses significant problems for research methodology and comparing AI systems across the medical field of practice. Lack of details on the amount of data used or the training models challenges the reliability of the models [35].
Future AI Application in the Field of Dermatopathology
The future of AI technology is promising in transforming the medical landscape by taking on repetitive tasks and improving efficiency in providing the best overall healthcare for patients. From aiding diagnostic decisions to personalized medicine that is tailored to patient management.
Further studies are needed to create a synchronized workforce system between AI and healthcare professionals as an augmented intelligence in diagnostic decision-making and forming treatment algorithms that are personalized to patient care. Furthermore, practice performance can be improved by reducing strain on highly experienced experts and elevating young experts' knowledge and guidance through system application.
Expanding Horizons of AI in Dermatopathology
Interpretability and Explainability in AI Models
While AI systems have demonstrated superior accuracy in dermatopathological diagnostics, a major barrier to clinical adoption remains the interpretability of these models. The “black box” nature of deep learning algorithms poses significant challenges when explaining how specific diagnostic decisions are made [36]. Recent developments in explainable AI (XAI) aim to increase transparency by visualizing model decision pathways and highlighting the features influencing outcomes. For instance, heatmap visualization using Gradient-weighted Class Activation Mapping (Grad-CAM) allows clinicians to understand which histopathological regions contributed most to the AI’s decision [37]. This transparency is critical not only for building clinician trust but also for ensuring compliance with medical regulatory standards.
Integration into Clinical Workflow and Digital Pathology Systems
AI’s integration into digital pathology workflows promises to revolutionize diagnostic efficiency, yet practical implementation remains complex. The combination of whole-slide imaging (WSI), cloud-based computational analysis, and AI algorithms allows near real-time diagnostic support [38]. However, integrating AI systems requires interoperability with existing electronic health records (EHRs) and laboratory information systems (LIS). Institutions adopting hybrid systems that merge human expertise with automated pre-screening models report improved throughput and reduced diagnostic errors. Establishing multidisciplinary AI committees comprising dermatopathologists, computer scientists, and regulatory specialists is increasingly viewed as essential for successful deployment in clinical environments.
Global Collaboration and Future Directions
AI research in dermatopathology must embrace global collaboration to overcome limitations in dataset diversity, infrastructure, and validation. International partnerships—such as the International Skin Imaging Collaboration (ISIC) and Global Pathology AI Consortium—have begun addressing disparities in data representation by including skin of colour and rare disease variants [39]. Additionally, federated learning approaches, where AI models are trained across decentralized datasets without compromising patient privacy, are emerging as a solution to data governance challenges [40]. Future directions point toward the integration of AI-driven diagnostic tools with genomics and proteomics to create multimodal systems capable of predicting disease progression, therapeutic response, and long-term outcomes [41].
Clinical Validation and Performance Benchmarking
Clinical validation remains one of the most critical steps before integrating AI tools into dermatopathology. Although numerous studies have demonstrated superior accuracy of AI in classifying skin lesions, large-scale multicenter trials are still limited. Establishing standardized validation frameworks—such as those proposed by the FDA’s Software as a Medical Device (SaMD) guidelines—ensures reproducibility and safety in clinical environments [36]. Performance benchmarking against pathologists under real-world conditions, including varied slide quality and patient demographics, is essential to ensure generalizability and reliability. Furthermore, prospective trials comparing AI-assisted diagnoses to standard pathology workflows are emerging as the gold standard for regulatory approval.
Ethical and Legal Considerations
As AI continues to permeate clinical dermatopathology, ethical concerns regarding patient privacy, data bias, and accountability must be addressed. Biased datasets can lead to diagnostic disparities, particularly among underrepresented populations with darker skin tones [42]. Ethical frameworks emphasizing transparency, informed consent, and equitable dataset representation are therefore critical. Legal liability remains another challenge—when AI and human diagnoses conflict, determining accountability for errors can be complex. International organizations such as the World Health Organization (WHO) and the European Commission are now working toward ethical AI governance models to ensure responsible innovation [38].
Future Prospects and Precision Dermatopathology
The next frontier of AI in dermatopathology lies in multi-omics integration—combining histopathological imaging with genomic, proteomic, and metabolomic data for personalized treatment prediction [43]. Emerging models like transformer-based networks and self-supervised learning architectures have shown remarkable capability in feature extraction from unlabelled histopathological data [44]. These innovations could enable AI systems to not only classify lesions but also predict therapeutic responses and disease progression. As digital pathology infrastructure grows globally, interdisciplinary collaboration will remain the key driver of safe and equitable AI adoption in clinical dermatopathology.
|
Emerging Area |
Description / Focus |
Expected Outcome |
Example / Reference |
|
Explainable AI (XAI) |
Visualizes neural network decision pathways |
Builds clinician trust; regulatory compliance |
Grad-CAM visualization [37] |
|
Integration with Digital Pathology |
Combines AI, WSI, and cloud analytics |
Near real-time diagnostic support |
[38] |
|
Federated Learning |
Distributed model training without data sharing |
Enhances privacy and data diversity |
[40] |
|
Multi-Omics Integration |
Combines imaging with genomic/proteomic data |
Enables precision dermatopathology |
[43,44] |
|
Clinical Validation Frameworks |
FDA’s SaMD and multicenter benchmarking |
Ensures reproducibility and safety |
[36] |
|
Ethical AI Governance |
WHO and EU-led transparency initiatives |
Promotes fairness and accountability |
[38] |
Table 3: Future Directions and Innovations
Conclusion
AI is rapidly transforming dermatopathology by enhancing computer vision to innovate and produce effective medical approaches. These technologies demonstrate significant potential in improving diagnostic precision and efficiency for image-intense analyses, often achieving high accuracy results in classifying lesions such as basal cell carcinoma (BCC), dermal nevi (DN), and seborrheic keratosis (SK), and assisting in challenging cases such as differentiation of melanoma from benign variants. Furthermore, AI, particularly when integrated with Whole-Slide Imaging (WSI), is employed to streamline workflows, reducing pathologists interference variability and dedicating time to complex cases. In addition to classification, AI enables advanced predictive analytics, utilizing multimodal integration of histopathological and parametric clinical data for personalized patient management and prognostic assessments. Despite the promising potential, significant challenges must be overcome, including the quantity of high-quality and diverse datasets. However, AI is currently positioned as a powerful diagnostic decision support tool to support human expertise in multidisciplinary collaboration to provide safe and ethical conditions in daily clinical practice.
References
- Aksoy, S., Demircioglu, P., & Bogrekci, I. (2024). Advanced artificial intelligence techniques for comprehensive dermatological image analysis and diagnosis. Dermato, 4(4), 173-186.
- Hirani, R., Noruzi, K., Khuram, H., Hussaini, A. S., & Aifuwa,E. I., et al. (2024). Artificial intelligence and healthcare: a journey through history, present innovations, and future possibilities. Life, 14(5), 557.
- Olawade, D. B., Wada, O. J., David-Olawade, A. C., Kunonga, E., & Abaire, O., et al. (2023). Using artificial intelligence to improve public health: a narrative review. Frontiers in Public Health, 11, 1196397.
- Shortliffe, E. H. (1977, October). Mycin: A knowledge-based computer program applied to infectious diseases. In Proceedings of the annual symposium on computer application in medical care (p. 66).
- Johnson, K. B., Wei, W. Q., Weeraratne, D., Frisse, M. E., & Misulis, K., et al. (2021). Precision medicine, AI, and the future of personalized health care. Clinical and translational science, 14(1), 86-93.
- Bakkar, N., Kovalik, T., Lorenzini, I., Spangler, S., & Lacoste, A., et al. (2018). Artificial intelligence in neurodegenerative disease research: use of IBM Watson to identify additional RNA-binding proteins altered in amyotrophic lateral sclerosis. Acta neuropathologica, 135(2), 227-247.
- Regression, N. (1992). An introduction to kernel and nearest-neighbor. Am. Stat, 46, 175-185.
- Diaz-Ramon, J. L., Gardeazabal, J., Izu, R. M., Garrote, E., & Rasero, J., et al. (2023). Melanoma clinical decision support system: An artificial intelligence-based tool to diagnose and predict disease outcome in early-stage melanoma patients. Cancers, 15(7), 2174.
- Esteva, A., Kuprel, B., Novoa, R. A., Ko, J., & Swetter, S. M., et al. (2017). Dermatologist-level classification of skin cancer with deep neural networks. nature, 542(7639), 115-118.
- Brinker, T. J., Schmitt, M., Krieghoff-Henning, E. I., Barnhill, R., & Beltraminelli, H., et al. (2022). Diagnostic performance of artificial intelligence for histologic melanoma recognition compared to 18 international expert pathologists. Journal of the American Academy of Dermatology, 86(3), 640-642.
- Cazzato, G., Massaro, A., Colagrande, A., Trilli, I., & Ingravallo, G., et al. (2023). Artificial intelligence applied to a first screening of naevoid melanoma: A new use of fast random forest algorithm in dermatopathology. Current Oncology, 30(7), 6066-6078.
- Cazzato, G., Massaro, A., Colagrande, A., Lettini, T., & Cicco,S., et al. (2022). Dermatopathology of malignant melanoma in the era of artificial intelligence: a single institutional experience. Diagnostics, 12(8), 1972.
- Hart, S. N., Flotte, W., Andrew, F., Shah, K. K., & Buchan,Z. R., et al. (2019). Classification of melanocytic lesions in selected and whole-slide images via convolutional neural networks. Journal of Pathology Informatics, 10(1), 5.
- Winkler, J. K., Sies, K., Fink, C., Toberer, F., & Enk, A., et al. (2020). Melanoma recognition by a deep learning convolutional neural network—performance in different melanoma subtypes and localisations. European Journal of Cancer, 127, 21-29.
- Yu, C., Yang, S., Kim, W., Jung, J., & Chung, K. Y., et al. (2018). Acral melanoma detection using a convolutional neural network for dermoscopy images. PloS one, 13(3), e0193321.
- Bao, Y., Zhang, J., Zhang, Q., Chang, J., & Lu, D., et al. (2021). Artificial Intelligence-aided recognition of pathological characteristics and subtype classification of superficial perivascular dermatitis. Frontiers in Medicine, 8, 696305.
- Shrivastava, V. K., Londhe, N. D., Sonawane, R. S., & Suri, J. S. (2017).Anovel and robust Bayesian approach for segmentation of psoriasis lesions and its risk stratification. Computer methods and programs in biomedicine, 150, 9-22.
- Abedini, M., von Cavallar, S., Chakravorty, R., Davis, M., & Garnavi, R. (2015, January). A Cloud-Based Infrastructure for Feedback-Driven Training and Image Recognition. In MedInfo (pp. 691-695).
- Ding, Y., Dhawan, G., Jones, C., Ness, T., & Nichols, E., et al. (2023). An open source pipeline for quantitative immunohistochemistry image analysis of inflammatory skin disease using artificial intelligence. Journal of the European Academy of Dermatology and Venereology, 37(3), 605-614.
- Arevalo, J., Cruz-Roa, A., Arias, V., Romero, E., & González,F. A. (2015). An unsupervised feature learning framework for basal cell carcinoma image analysis. Artificial intelligence in medicine, 64(2), 131-145.
- Olsen, T. G., Jackson, B. H., Feeser, T. A., Kent, M. N., & Moad, J. C., et al. (2018). Diagnostic performance of deep learning algorithms applied to three common diagnoses in dermatopathology. Journal of pathology informatics, 9(1), 32.
- Spyridonos, P., Gaitanis, G., Likas, A., & Bassukas, I. D. (2017). Automatic discrimination of actinic keratoses from clinical photographs. Computers in biology and medicine, 88, 50-59.
- Kulkarni, P. M., Robinson, E. J., Sarin Pradhan, J., Gartrell-Corrado, R. D., & Rohr, B. R., et al. (2020). Deep learning based on standard H&E images of primary melanoma tumors identifies patients at risk for visceral recurrence and death. Clinical Cancer Research, 26(5), 1126-1134.
- Johannet, P., Coudray, N., Donnelly, D. M., Jour, G., & Illa-Bochaca, I., et al. (2021). Using machine learning algorithms to predict immunotherapy response in patients with advanced melanoma. Clinical Cancer Research, 27(1), 131-140.
- Surmanowicz, P., Emam, S., Du, A., Thomsen, S. F., & Greiner, R., et al. (2020). 17850 Predicting the long-term outcomes of biologics in psoriasis patients using machine learning. Journal of the American Academy of Dermatology, 83(6), AB86.
- Tan, E., Lin, F., Sheck, L., Salmon, P., & Ng, S. (2017). A practical decision-tree model to predict complexity of reconstructive surgery after periocular basal cell carcinoma excision. Journal of the European Academy of Dermatology and Venereology, 31(4), 717-723.
- Waseh, S., & Lee, J. B. (2023). Advances in melanoma: epidemiology, diagnosis, and prognosis. Frontiers in medicine, 10, 1268479.
- Levene, A. R. N. O. L. D. (1980). On the histological diagnosis and prognosis of malignant melanoma. Journal of clinical pathology, 33(2), 101-124.
- Schmoeckel, C., Castro, C. E., & Braun-Falco, O. (1985). Nevoid malignant melanoma. Archives of dermatological research, 277(5), 362-369.
- Huang, M. L., Hung, Y. H., Lee, W. M., Li, R. K., & Jiang,B. R. (2014). SVM-RFE based feature selection and Taguchi parameters optimization for multiclass SVM classifier. The Scientific World Journal, 2014(1), 795624.
- Burlina, P., Billings, S., Joshi, N., & Albayda, J. (2017). Automated diagnosis of myositis from muscle ultrasound: exploring the use of machine learning and deep learning methods. PloS one, 12(8), e0184059.
- Cocuz, I. G., Niculescu, R., Popelea, M. C., Cocuz,M. E., & Sabau, A. H., et al. (2025). Current trends and future directions of digital pathology and artificial intelligence in dermatopathology: a scientometric-based review. Diagnostics, 15(17), 2196.
- Rezk, E., Eltorki, M., & El-Dakhakhni, W. (2022). Leveraging artificial intelligence to improve the diversity of dermatological skin color pathology: protocol for an algorithm development and validation study. JMIR Research Protocols, 11(3), e34896.
- Farahani, N., Parwani, A. V., & Pantanowitz, L. (2015). Whole slide imaging in pathology: advantages, limitations, and emerging perspectives. Pathology and Laboratory Medicine International, 23-33.
- Vezeteu, P. V., Andronescu, A. D., & Nastac, D. I. (2025). A Literature Review on Artificial Intelligence in Dermatological Diagnosis and Tissue Microscopy. IEEE Photonics Journal.
- Holzinger, A., Langs, G., Denk, H., Zatloukal, K., & Müller, H. (2019). Causability and explainability of artificial intelligence in medicine. Wiley interdisciplinary reviews: data mining and knowledge discovery, 9(4), e1312.
- Selvaraju, R. R., Cogswell, M., Das, A., Vedantam, R., & Parikh, D., et al. (2017). Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE international conference on computer vision (pp. 618-626).
- Komura, D., & Ishikawa, S. (2018). Machine learning methods for histopathological image analysis. Computational and structural biotechnology journal, 16, 34-42.
- Rotemberg, V., Kurtansky, N., Betz-Stablein, B., Caffery, L., & Chousakos, E., et al. (2021). A patient-centric dataset of images and metadata for identifying melanomas using clinical context. Scientific data, 8(1), 34.
- Li, T., Sahu,A. K., Talwalkar, A., & Smith, V. (2020). Federated learning: Challenges, methods, and future directions. IEEE signal processing magazine, 37(3), 50-60.
- Madabhushi, A., & Lee, G. (2016). Image analysis and machine learning in digital pathology: Challenges and opportunities. Medical image analysis, 33, 170-175.
- Selvaraju, R. R., Cogswell, M., Das, A., Vedantam, R., & Parikh, D., et al. (2017). Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE international conference on computer vision (pp. 618-626).
- Rotemberg, V., Kurtansky, N., Betz-Stablein, B., Caffery, L., & Chousakos, E., et al. (2021). A patient-centric dataset of images and metadata for identifying melanomas using clinical context. Scientific data, 8(1), 34.
- Li, T., Sahu,A. K., Talwalkar, A., & Smith, V. (2020). Federated learning: Challenges, methods, and future directions. IEEE signal processing magazine, 37(3), 50-60.