



Research Article - (2019) Volume 4, Issue 1
Arterial Hypertension in Patients Aged 15 Years and Over in the Cardiology Department of Sikasso Hospital in Mali: About 250 Cases
2Department of Cardiology, Teaching Hospital Aristide Le Dantec, Dakar, Senegal
3Department of Cardiology, Teaching Hospital Gabriel Touré, Bamako, Mali
4Department of Cardiology, Regional Hospital of Saint Louis, Saint Louis, Senegal
Received Date: Feb 11, 2019 / Accepted Date: Mar 02, 2019 / Published Date: Mar 07, 2019
Copyright: ©Sangare Zoumana, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: High blood pressure is a global public health problem due to its high prevalence and multiple complications that often lead to major disability. It is a major cardiovascular risk factor for often late diagnosis. It is emerging in Africa, particularly in Mali.
Objective: To determine the epidemiological, diagnostic and progressive aspects of high blood pressure in patients 15 years of age or older. Patients and methods: This is a descriptive cross-sectional study over a two-year period (June 1, 2008 to May 31, 2010) in the Cardiology Department of Sikasso Hospital in any patient aged 15 years and over admitted for high blood pressure.
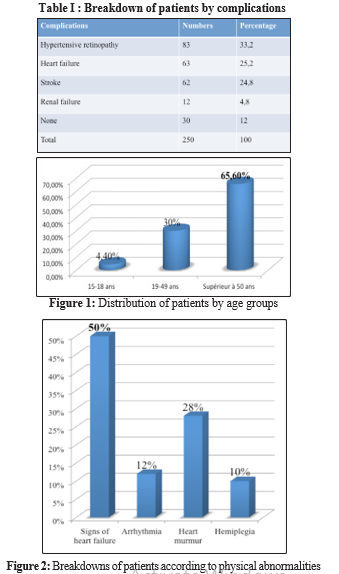
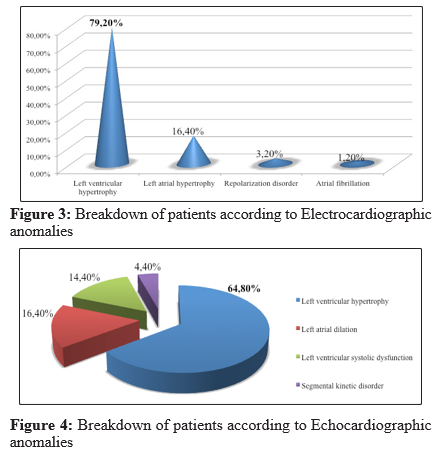
Results: Two hundred and fifty patients were selected, representing a hospital prevalence of 18.2%. High blood pressure was most common in patients 50 years of age and older (65.6%), followed by those 19 to 49 years of age (30%) and those 15 to 18 years of age. The average age of the population was 50 years (15-92 years) with a male predominance of 61.6% and a sex ratio of 1.6. The predominance of traditional housewives and farmers was 30% and 26.4%. The notion of a family history of high blood pressure was found in 56.4% of cases. High blood pressure grade 3 according to the classification of the World Health Organization was mostly found in our patients (64%). Biological abnormalities were dominated by hyperglycemia (14%), hypercreatininemia (8%). The main clinical manifestations were headache (40%), dyspnea (20%) and vertigo (16%). On physical examination, there were mainly signs of heart failure (50%), arrhythmia (12%), heart murmur (28%), hemiplegia (10%). The electrocardiogram showed left ventricular hypertrophy in 79.2% of cases, left atrial hypertrophy (16.4%), repolarization disorder (3.2%), atrial fibrillation (1.2%). Chest x-rays showed cardiomegaly in 67.2%. Echocardiographic abnormalities were left ventricular hypertrophy (64.8%), left atrial dilation (16.4%), left ventricular systolic dysfunction (14.4%). Therapeutically, diuretic combination with conversion enzyme inhibitors was the most prescribed treatment (58%), followed by combination of calcium channel blockers and conversion enzyme inhibitors (15.6%), calcium channel blockers (18%), conversion enzyme inhibitors (4.4%), beta-blockers (4%). The low-salt diet and physical activity were constantly recommended. Complications were hypertensive retinopathy (33.2%), heart failure (25.2%), stroke (24.8%), renal failure 4.8%.
Conclusion: High blood pressure is a major public health problem. This work identified a high hospital prevalence of high blood pressure in patients aged 15 years and older with a clear male predominance. Late diagnosis is responsible for serious complications that often lead to major disabilities.
Keywords
Hypertension, 15 years and older, Left ventricular hypertrophy, Sikasso (Mali).
Introduction
High blood pressure is a global public health problem due to its high prevalence and multiple complications that often lead to major disability [1]. It is a major cardiovascular risk factor for often late diagnosis. It is emerging in Africa, particularly in Mali [2]. It is estimated that about one billion people worldwide suffer from high blood pressure and this number is expected to increase as the population ages [1]. In Africa, its prevalence is estimated at 21.5% in Abidjan in Côte d’Ivoire and 41% in Ibadan in Nigeria [3]. In Mali, it ranks first among cardiovascular diseases with a prevalence of 37% and represents 43.9% of the reasons for cardiovascular consultation in cardiology [2]. In addition to its high prevalence and potential morbidity, high blood pressure is the most frequent cause of left ventricular pressure overload, initially responsible for hypertrophy and dilation of the left atrium, then hypertrophy of the left ventricle, dilation and finally heart failure [4].
Objective
To determine the epidemiological, diagnostic and progressive aspects of high blood pressure in patients 15 years of age or older.
Patients and Methods
This was a descriptive cross-sectional study over a two-year period (June 1, 2008 to May 31, 2010) in the Cardiology Department of Sikasso Hospital in any patient 15 years of age or older admitted with high blood pressure. The parameters studied included epidemiological, clinical, paraclinical, therapeutic and progressive data. High blood pressure has been defined as blood pressure greater than or equal to 140/90 mmHg and/or a known history of high blood pressure. The 1999 World Health Organization classification was used to stratify the severite of high blood pressure [5]. For the control, the values used were less than 140/90mmHg. Diabetes mellitus was defined as fasting plasma glucose greater than or equal to 1.26 g/L and/or a known history of diabetes; the dosage was repeated in the event of hyperglycemia in unknown diabetic subjects. Hypercreatinemia was defined as a blood creatinine level greater than 13mg/L. The systolic function of the left ventricle was evaluated by the Simpson biplane method. It was moderately altered if the ejection fraction is between 54 and 45%, moderately altered between 44 and 30% and severely altered below 30% (ESA). The data were collected on a pre-established survey sheet, transcribed into a database and entered using the EXCEL table software version 2010. The statistical analysis of the data was performed by the SPSS software version 20.0.
Results
Two hundred and fifty patients were selected, representing a hospital prevalence of 18.2%. High blood pressure was most common in patients 50 years of age and older (65.6%), followed by those 19 to 49 years of age (30%) and those 15 to 18 years of age (Figure1).The average age of the population was 50 years (15-92 years) with a male predominance of 61.6% and a sex ratio of 1.6. The predominance of traditional housewives and farmers was 30% and 26.4%. The notion of a family history of high blood pressure was found in 56.4% of cases. High blood pressure grade 3 according to the classification of the World Health Organization was mostly found in our patients (64%). Biological abnormalities were dominated by hyperglycemia (14%), hypercreatinemia (8%). The main clinical manifestations were headache (40%), dyspnea (20%) and vertigo (16%). On physical examination, there were mainly signs of heart failure (50%), arrhythmia (12%), heart murmur (28%), hemiplegia (10%) (Figure2). The electrocardiogram showed left ventricular hypertrophy in 79.2% of cases, left atrial hypertrophy (16.4%), repolarization disorder (3.2%), atrial fibrillation (1.2%) (Figure3). Chest x-rays showed cardiomegaly in 67.2%. Echocardiographic abnormalities were left ventricular hypertrophy (64.8%), left atrial dilation (16.4%), left ventricular systolic dysfunction (14.4%), segmental kinetic disorder (4,4%) (Figure4). Therapeutically, diuretic combination with conversion enzyme inhibitors was the most prescribed treatment (58%), followed by combination of calcium channel blockers and conversion enzyme inhibitors (15.6%), calcium channel blockers (18%), conversion enzyme inhibitors (4.4%), beta-blockers (4%). The low-salt diet and physical activity were constantly recommended. Complications were hypertensive retinopathy (33.2%), heart failure (25.2%), stroke (24.8%), renal failure 4.8% (Table I).
Discussion
The hospital prevalence of high blood pressure in our study was 18.2%. This result is comparable to that of Ouologuem, which found 18.3% in Bamako [6]. This high prevalence could be explained by the increase in risk factors such as high blood pressure, age, smoking, alcoholism, sedentary lifestyle and diabetes. Our study shows that the older the individual, the higher the risk of high blood pressure. As a result, the percentage of people aged 15 to 18 rose from 4.4% to 30.0% for those aged 19 to 49 and 65.6% for those aged 50 and over. This same finding has been made by other authors who have shown that age is a risk factor for the development of high blood pressure [7-11]. We observed a male predominance. This is explained by this major risk factor, which is smoking exclusively among men. Male predominance does not appear in some studies. This is the case in Niger where the hypertensive population included 56% women and 44% men, in South Africa in an urban population where 25.8% of women were hypertensive, compared to 13.4% of men. The family concept of high blood pressure was high in our study, at 56.4% [12, 13]. This result is comparable to that of Ouologuem, which found 65.6% [6]. Studies have shown that heredity plays a role in the development of high blood pressure; this heredity refers to an increased sensitivity to sodium associated with a decrease in renal excretion of a sodium load [14,15]. The main clinical manifestations were headache (40%), dyspnea (20%), and vertigo (16%). Traoré had reported these same symptoms respectively 48.5%, 38.8% and 40.7% [16]. This difference can be explained by the size of our samples. Chest x-rays showed cardiomegaly in 67.2% of cases. This result is higher than Coulibaly’s (50.4%) [17]. The electrocardiogram showed left ventricular hypertrophy in 79.2%. This frequency is higher than that of Coulibaly (30%) and Traore (39.6%) [17,16]. Echocardiographic abnormalities were in order of frequency: left ventricular hypertrophy (64.8%), left atrial dilation (16.4%), and systolic left ventricular dysfunction (14.4%). These abnormalities are evidence of late detection and installation of heart failure
Therapeutically, diuretic combination with conversion enzyme inhibitors was the most prescribed treatment (68.0%), followed by calcium channel blockers (18.0%). This preference for conversion enzyme inhibitors and diuretics is explained by their effectiveness in preventing and managing cardiovascular and renal complications [18]. The complications encountered were hypertensive retinopathy (33.2%), heart failure (25.2%), stroke (24.8%), renal failure 4.8%. In its study, Simpara reported 43% renal failure and 33.8% stroke [19]. Lokrou found 60.6% of cases of renal failure in his study in Côte d’Ivoire [20].
Conclusion
High blood pressure is a major public health problem. This work identified a high hospital prevalence of high blood pressure with a clear male predominance among patients 15 years of age and older.
Late diagnosis is responsible for serious complications that often lead to major disability, hence the need for prevention through early detection and proper management
References
- Chobanian AV, Bakris GL, Black HR (2003) The Seventh Report of Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood pressure; the JNC7 report. JAMA 289: 2560-2572.
- Sanogo KM (1980) Complication de l’HTA et leurs évolutions observées en milieu hospitalier. Thèse Med, Bamako N°184.
- Dubourg O, Boudarias JP (1996) Exploration échographique doppler des myocardiopathiesArch mal Cœur vx 2: 39-45.
- Makalou D (2009) La cardiomyopathie hypertensive dans le service de cardiologie de l’hôpital Gabriel TOURE. Thèse Med, Bamako N°70.
- Guidelines sub-committee 1999 World Health Organization/ International Society of Hypertension guidelines for the management of hypertension. J Hypertens 17: 151-183.
- Ouologuem N (2005) Place de l’HTA dans la pathologie cardiovasculaire dans le district de Bamako en 2002. Thèse Med. Bamako N°170.
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, et al. (2005) « Global Burden of hypertension : analysis of worldwide data». The Lancet 365: 217-223.
- Franklin SS, Gustin W 4th, Wong ND, Larson MG, Weber MA, et al. (1997) Hemodynamics patterns of age related changes in blood pressure. The Framingham Heart Study. Circulation 96: 308-315.
- Mial WE, Kass EH, Ling J, Stuart KL (1962) Factors influencing arterial pressure in general population of Jamaica. BNJ 2: 497- 506.
- Klatsky AL, Friedman G D, Siegelaub AB, Gérard MJ (1977) Alcohol consumption and blood pressure. KAISER-Permanente multiphasic health examination Dtaat. N Engl J Med 296: 194-200.
- Savage DD (1987) Left ventricular hypertrophy and diastolic fonctional abnormalities in black and white hypertensive patients. J Natl Med Assoc 79: 13-6.
- Cenac A, Mounis OM, Develoux M, et al. (1985) Les cardiopathies de l’adulte à Niamey (Niger). Enquête épidémiologiqueprospective à propos de 162 observations. Cardiol Trop 11: 125-133.
- Seedat YK (1983) Race environment and blood pressure : the South African experience. J Hypertens 1: 7-12
- Prineas RJ, Gillum RF (1985) US epidemiology of hypertension in blacks. In: Hall WD, Saunders E, ShulmanNB, Eds. Hypertension in blacks: epidemiology, pathophysiology and treatment. Year book Med, Chicago 17: 36.
- Bertrand Ed (1976) Etude de la prévalence et certains aspects épidémiologiques de l’HTA en Côte d’Ivoire. Bull OMS 54: 449-454.
- Traoré BM. L’hypertension chez les personnes âgées dans le service de cardiologie du CHU Gabriel TOURE. Thèse Med Bamako N°173.
- Coulibaly OM (2011) Hypertension artérielle et la prise encharge thérapeutique dans le service de cardiologie «A » de l’hôpital du point G. Thèse Med, Bamako N°114.
- Michel Bertrand (2007) Place des IEC en cardiologie et neurologie, Phase 5, Editions médicales.
- Simpara M (1993) Surveillance de l’hypertension artérielle en milieu hospitalier et en ambulatoire de l’Hôpital Gabriel Touré à propos 565 cas. Thèse Med, Bamako N°15.
- Lokrou A, Diallo TT, Ouedraogo Y, et al. (1987) Hypertension artérielle et diabète en Côte d’Ivoire. Med Afr Noire: 34: 605- 610.